Stewart-Treves syndrome, first described in 1948 by Fred Stewart and Norman Treves, is a rare and malignant pathology. It originates from vascular and lymphatic endothelial cells and is generally observed in post-mastectomy patients with axillary dissection, with submission to radiotherapy and consequent lymphatic stasis as a risk factor.(
Female, 68 years old, Caucasian, smoker, admitted to the hospital service in 2010, with extensive lymphedema in the right forearm, on physical examination it was noted a painful and extensive area of raised ulceration of a necrotic and hemorrhagic character (
Figura 1 Cutaneous lesion showing erythematous plaque with coalescing, purple, bullous, and easily bleeding lesions on the right forearm, surrounded by satellite blood blisters, showing diffuse edema.
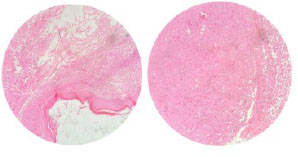
Figura 2 Microscopy shows a malignant tumor of fusiform, hyperchromatic, high-grade pleomorphic endothelial cells with formation of vascular channels and extravasation of red blood cells at the dermal-subcutaneous junction.
Berger’s surgery (
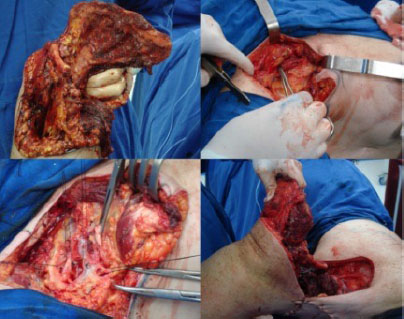
Figura 3 Resection of the entire upper limb and shoulder girdle, including the scapula and a portion of the clavicle.
Figura 4A. Immediate postoperative period after Berger surgery, with drain; B. Surgical specimen removed in the Berger procedure; C-E. Late postoperative images of the Berger surgery, showing the healing and evolution of the procedure.
In 2017, the patient was hospitalized with heterogeneous complications, of a renal nature classified as chronic kidney disease stage IIIa, and cardiac, characterized by paroxysmal atrial fibrillation, being controlled with clinical measures within the hospital environment and discharged with drug treatment. In the year 2020, the patient returns with complaints of nausea and weight loss, performing multiple biopsies, being diagnosed with esophageal cancer, obtaining a complete response to radiotherapy and gastrostomy with adjustments and changes throughout her life. In 2022, the patient is diagnosed with a new malignant neoplasm in the left breast, requiring hospitalization, as she is a smoker and has chronic obstructive pulmonary disease, she had complications that prevented her from having the surgery to remove the neoplastic nodule, evolving with pneumonia and subsequent sepsis, which led the patient to death.
Stewart-Treves syndrome (STS) is a highly rare, fatally aggressive condition with a poor prognosis, first described in 1948 by Fred Stewart and Norman Treves. The syndrome consists of a tumor originating from endothelial cells with a vascular component resembling a hemangiosarcoma and a lymphatic component resembling a lymphangiosarcoma,(
The age of greatest occurrence of Stewart-Treves syndrome is between 65 and 70 years, representing the predisposition to breast cancer and latency for the progression of chronic lymphedema, and the incidence is 0.07%-0.45% after radical mastectomy. Although STS mostly develops after radical mastectomy, it can manifest as congenital or acquired lymphedema, related to trauma, filariasis, idiopathic lymphoma, venous stasis, morbid obesity, ulcerations in the lower limbs and invasion of the inguinal region by a cervical or penile tumor. The risk of developing the syndrome increases by 15.9% when undergoing postoperative radiotherapy.(
In case of clinical suspicion of Stewart-Treves syndrome, surgical biopsy is essential to prove the disease and rule out other differential diagnoses, as was done in the present case. Currently, immunohistochemistry has been used to prove the epithelial nature of tumor cells.(
In the present case, it was possible to observe a 12-year evolution, much higher than what has been described so far, the patient’s clinical condition and the interventions performed may have contributed to the favorable evolution and survival presented. Treatment possibilities have limited success, being individualized on a case-by-case basis, ranging from large resections, amputation or disarticulation, such as the Berger surgery,(
Chemotherapy therapy can be beneficial when there is a response to the first treatment, radiotherapy is reserved for patients with severe clinical instability or palliative and supportive conditions, the chemotherapy drugs used are: 5-fluorouracil, methotrexate, bleomycin and/or a combination of actinomycin D, vincristine, doxorubicin and cyclophosphamide.(
Clinical follow-up of patients who underwent mastectomy with axillary dissection, radioactive therapy or who had chronic lymphedema is essential, both for a preventive approach and for biopsy of suspicious lesions, corroborating a favorable outcome. In addition, research must be carried out to optimize treatment, aiming at less aggressive interventions and better quality of life for victims of Stewart-Treves syndrome.
EF Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
EF Data analysis and interpretation
LFD Conception and design, Final approval of manuscript, Provision of study materials or patient
LCN Final approval of manuscript
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Wierzbicka-Hainaut, E and Guillet, G. Syndrome de Stewart-Treves (angiosarcome sur lymphœdème): complication rare du lymphųdème. Presse Med [online]. 2010, vol. 39, p. 1305-8.
2. Wang, LL and Cui, LF and Gao, Y and Jiang, ZC. Clinicopathologic features of Stewart-Treves syndrome. Int J Clin Exp Pathol [online]. 2019, vol. 12, p. 680-8.
3. Pereira, ESP and Moraes, ET and Siqueira, DM and Santos, MAS. Stewart-Treves syndrome. An Bras Dermatol [online]. 2015, vol. 90, p. 229-31.
4. Mesli, SN and Ghouali, AK and Benamara, F and Taleb, FA and Tahraoui, H and Abi-Ayad, C. Stewart-Treves syndrome involving chronic lymphedema after mastectomy of breast cancer. Case Rep Surg [online]. 2017, vol. 2017, p. 1-4.
5. Sevil, A and Aktas, H and Ömer, FE and Aktümen, A and Erol, H. Stewart Treves syndrome in a woman with mastectomy. J Clin Diagn Res [online]. 2016, vol. 10, p. WD1-WD2.
6. Vieira, LJ and Vieira, JP and Oliveira, AF and Freitas, RR and Rabêlo, FT and Mira, RRL. Tratamento cirúrgico de tumores malignos envolvendo ombro e membro superior: estudo de 10 casos. Rev Bras Cancerol [online]. 2004, vol. 50, p. 127-32.
7. Rev Col Bras Cir. 2013;40(5) [online]. Available from: <>.
8. Khatri, VP. Atlas de técnicas avançadas em cirurgia [Internet]. Grupo GEN, 2014.
9. Esbeen, LV and Rocket-Gravy, PP. Improvement of Stewart-Treves angiosarcoma through interleukin 23p19 inhibition. JAAD Case Rep [online]. 2021, vol. 17, p. 84-6.


Dados de acesso insuficientes para visualização no mapa.