Melanoma incidence has been rising in fair-skinned populations over the past several decades. However, since 2011, melanoma-related mortality has declined by approximately 30%, primarily due to the Food and Drug Administration's (FDA) approval of targeted therapies, including immune checkpoint inhibitors (ICIs) and small-molecule kinase inhibitors.
These ICIs are indicated for various cancers, including melanoma,
Retrospective studies have reported that 10 to 25% of patients with metastatic melanoma have preexisting autoimmune diseases (AIDs).
Prospective studies have documented higher irAE frequencies in patients with autoimmune conditions, such as psoriasis (Pso), rheumatoid arthritis (RA), polymyalgia rheumatica (PMR), chronic cutaneous lupus, and others.
The BRAF/MEK inhibitors, another class of targeted therapies, are used to treat melanoma with specific kinase mutations.
This study aims to evaluate the best therapeutic approaches for patients with metastatic melanoma and immune-mediated diseases based on a narrative literature review and a case series of patients treated at the A.C.Camargo Cancer Center's outpatient clinic.
This retrospective study included 10 adults with disseminated melanoma and AIDs who attended the Rheumatology Outpatient Clinic at the A.C.Camargo Cancer Center in Brazil, between January 2020 and September 2024.
A narrative literature review was conducted using Scopus and PubMed, incorporating the following Medical Subject Headings (MeSH) keywords: “melanoma”, “immune checkpoint inhibitors”, “targeted therapy”, “pre-existing autoimmune disorder”, “rheumatic disorder”, “immune-mediated adverse event”, “disease-modifying antirheumatic drug (DMARD)”, “anti-PD-1/PD-L1”, and “anti-CTLA-4”.
The study was approved by the institution's Ethics Committee, and all patients provided written informed consent.
There were six patients with preexisting AID, three with RA, one with systemic lupus erythematosus (SLE), one with Pso, and one with inflammatory recurrent serositis. Furthermore, four patients developed rheumatic irAEs after treatment. The patients were followed for 6 months after symptom onset.
There were 6 patients with preexisting AID and stage III to IV melanoma required DMARD for either disease flare or de novo irAEs (n = 4), as shown in
| Case | S, A | Preexisting autoimmune disease/Ab | Stage* | OST | OST duration | AE after OST/CTCAE grade | IS | Response to IS | Response to OST | OST status |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F, 70 | RA/FR+ | IV | nivolumab | 0,5 | RA flare grade 4 | PRED SSZ HCQ TCZ | Complete | Progression | Restarted |
| 2 | F, 34 | SLE/Ro + LAC+ | IV | nivolumab | 7 | SLE Flare grade 2 | PRED HCQ | Complete | Complete | Completed |
| 3 | M, 59 | Psoriasis/No | III | nivolumab | 7 | APs and Pso flare grade 4 | PRED TNFi MTX COS | Complete | Progression | Restarted |
| 4 | F, 75 | RA/FR+ | IV | ipilimumab nivolumab | 7 | Herpes on the tongue | MTX TCZ | Complete | Complete | Ongoing |
| 5 | F, 69 | RA/FR+ | III | nivolumab | 6 | − | MTX | Complete | Complete | Ongoing |
| 6 | M, 49 | Inflammatory recurrent serositis/No | III | dabrafetinib and trametinib | 3 | AR-like grade 3 | PRED MTX | Complete | Stable | Ongoing |
Abbreviations: A, age, in years; Ab, autoantibody; AE, adverse event; AID, autoimmune disease; APs, activator proteins; COS, cosentyx; CTCAE, Common Terminology Criteria for Adverse Events; F, female; FR, rheumatoid factor; HCQ, hydroxychloroquine; IS, rheumatic immunosuppressant; LAC + , lupus anticoagulant positive; M, male; MTX, methotrexate; OST, oncologic systemic therapy; PRED, prednisone; Pso, psoriasis; RA, rheumatoid arthritis; Ro + , anti-Ro/SSA positive; S, sex; SLE, systemic lupus erythematosus; SSZ, sulfasalazine; TCZ, tocilizumab; TNFi, TNF inhibitor.
Notes: *Stage of melanoma. The AE was measured after OST onset. The OST duration was measured in months, OST status was measured after 6 months of IS onset, and response to OST was measured as oncological outcome after 6 months. Response to IS was measured as rheumatic disease response after 6 months of IS.
Patient 1 (RA in remission) was not on immunosuppressants when cancer treatment began. However, she experienced RA reactivation after the first nivolumab (anti-programmed cell death protein 1 [PD1]) infusion. She discontinued ICI therapy and was treated with sulfasalazine (SSZ) and hydroxychloroquine (HCQ). Unfortunately, she developed SSZ hypersensitivity, leading to hepatotoxicity and myelotoxicity, which were managed with prednisone (1 mg/kg). She was later transitioned to tocilizumab (TCZ, an interleukin-6 [IL-6] inhibitor, 4 mg/kg every 4 weeks), which enabled her to resume nivolumab while maintaining RA control. Then, ICI was reintroduced, but the patient experienced cancer progression.
Patient 2 (SLE) experienced a mild flare with inflammatory arthralgia in the hands and wrists, which was resolved with low-dose prednisone (< 10 mg/day) and HCQ (5 mg/kg/day). Prednisone was tapered, and the patient remained in rheumatic and cancer remission with HCQ alone.
Patient 3 (Pso in remission) developed severe psoriatic arthritis (PsA) and Pso relapse after the seventh nivolumab dose. Initially managed with prednisone (10–20 mg/day) and one infusion of infliximab (IFX, anti-tumor necrosis factor alpha [TNFα]), the patient later experienced tumor progression and was switched to methotrexate (MTX) plus secukinumab (SCK, anti-IL17A). This regimen controlled symptoms while allowing corticosteroid tapering.
Patients 4 and 5 (RA in remission) remained stable while receiving ICI therapy and achieved a complete response to cancer. Patient 4 (MTX 15 mg/week, TCZ 162 mg every 2 weeks, and immunotherapy) developed a herpetic tongue ulcer after the fourth dose of nivolumab/ipilimumab, treated with valacyclovir.
Patient 5 (history of scleritis and mild arthritis) was on MTX 20 mg/week during nivolumab therapy and did not experience irAEs.
Patient 6 (inflammatory recurrent serositis) developed hand and wrist arthritis after starting dabrafenib (BRAF inhibitor) and trametinib (MEK1/2 inhibitor). Treatment included prednisone 20 mg/day (discontinued in 1–2 months), colchicine, and MTX 15 mg/week to manage symptoms. Targeted therapy was continued, and cancer stabilized.
In retrospective studies, the frequency of AID flares during ICI ranges from 20 to 50%. These flares often resemble previous disease activity, as observed in patients 1, 2, and 3 (
Reduced anti-tumor efficacy of systemic therapy due to immunosuppressants treating AID flares is a concern. Brown et al.
Some retrospective studies showed an association between the use of glucocorticoids at the beginning of ICI treatment for metastatic melanoma and reduced OS. However, these studies did not report the reasons for using glucocorticoids, making any conclusions speculative.
Other retrospective studies revealed comparable OS in metastatic melanoma and non-small-cell lung cancer patients, whether they had AID or not.
The HCQ is a DMARD frequently used as a first-line treatment for inflammatory arthropathy secondary to AID or ICI. It has demonstrated safety and effectiveness in managing mild symptoms, as seen in patients 1 and 2, as well as in several case series.
Sharma et al. revealed that HCQ enhanced the antitumor efficacy of anti-PD-1 therapy in mouse models by inhibiting palmitoyl-protein thioesterase 1 (PPT1).
A phase-I/II trial evaluating patients with advanced BRAFV600 mutant melanoma indicated that HCQ combined with dabrafenib and trametinib was safe and effective, with an antitumor effect. It may improve response rates to MAPK-targeted therapy due to its role as a lysosomal inhibitor that blocks autophagy, making it a potentially safe option for treating arthralgia induced by BRAF/MEK inhibitors.
Retrospective studies involving patients with RA and PMR showed the safety and effectiveness of MTX therapy for those receiving ICIs.
Some retrospective studies indicated that SSZ monotherapy leads to poorer control of arthritis induced by ICI and a higher incidence of hypersensitivity reactions compared to its use in treating RA patients.
The use of TCZ is an effective treatment for AID flares and irAEs, as evidenced by patients 1 and 4. Observational retrospective studies demonstrated the effectiveness and safety of IL-6 inhibitors in treating rheumatic irAEs and AID flares, such as RA, psoriatic arthritis (APs), and PMR.
Preclinical studies found that IL-6 inhibitors enhance the tumor-infiltrating T-cell response induced by anti-CTLA-4 therapy in murine models, demonstrating an antitumoral effect.
Furthermore, in a retrospective study by Petit et al.,
Tumor necrosis factor inhibitors (TNFi) are another option for treating AID and rheumatic irAEs and may help prevent the latter. Retrospective studies showed that TNFi leads to quicker resolution of colitis and inflammatory arthritis related to ICI treatment, without compromising OS compared to corticosteroid monotherapy.
However, a cohort of 1,250 melanoma patients treated with ICI revealed lower OS in those using TNFi compared to those receiving glucocorticoids alone for irAE treatment, independent of sex, performance status, comorbidities, disease stage, metastasis, and ICI subtype.
The use of IL-17 inhibitors effectively controlled preexisting APs, Pso, and arthritis induced by ICI treatment while maintaining the anti-tumor effect of immunotherapy in case reports.
In this case series, four patients diagnosed with stage II to III melanoma received DMARD as a treatment for de novo irAEs (
| Case | S, A | Preexisting AID/Ab | Stage* | OST | OST duration | AE after OST | IS | Response to IS | Response to OST | OST status |
|---|---|---|---|---|---|---|---|---|---|---|
| 7 | F, 46 | No/No | III | nivolumab | 10 | Oligoarthritis grade 3 | NSAID PRED MTX HCQ | Complete | Stable | Completed |
| 8 | F, 74 | No/No | III | nivolumab | 12 | AR-like grade 2 | SSZ | Complete | Complete | Completed |
| 9 | F, 63 | No/No | II | nivolumab and ipilimumab | 2 | Myocarditis and myositis grade 3 | PRED MMF | Complete | Stable | Suspended |
| 10 | F, 42 | No/No | III | trametinib dabrafenib encorafenib binimetinibe | 1 | Nodosum erythema, myalgia grade 3 | PRED MTX | Complete | Stable | Continued |
Abbreviations: A, age, in years; Ab, autoantibody; AE, adverse event; AID, autoimmune disease; F, female; HCQ, hydroxychloroquine; irAEs, immune-related adverse events; IS, rheumatic immunosuppressant; M, male; MMF, mycophenolate mofetil; MTX, methotrexate; NSAID, non-steroidal anti-inflammatory drugs; OST, oncologic systemic therapy used; PRED, prednisone; S, sex; SSZ, sulfasalazine.
Notes: *Stage of melanoma. The AE was measured after OST onset. The OST duration was measured in months, OST status was measured after 6 months of IS onset, and response to OST was measured as oncological outcome after 6 months. Response to IS was measured as rheumatic disease response after 6 months of IS.
Patient 7 developed oligoarthritis affecting the bilateral knees and ankles, which did not respond to nonsteroidal anti-inflammatory drugs (NSAIDs) after the tenth dose of nivolumab. She required low-dose prednisone (maximum 20 mg/day) and was treated with HCQ and MTX to control symptoms. She achieved remission within 6 months and was able to maintain HCQ while discontinuing MTX. The patient achieved a complete response with ICI therapy.
Patient 8 had arthritis in the wrists and hands, negative rheumatoid factor, and antinuclear antibodies following the last nivolumab infusion. We introduced SSZ to control the arthritis after completing anti-PD1 therapy, with a good response. She also used acetaminophen and codeine to manage pain symptoms.
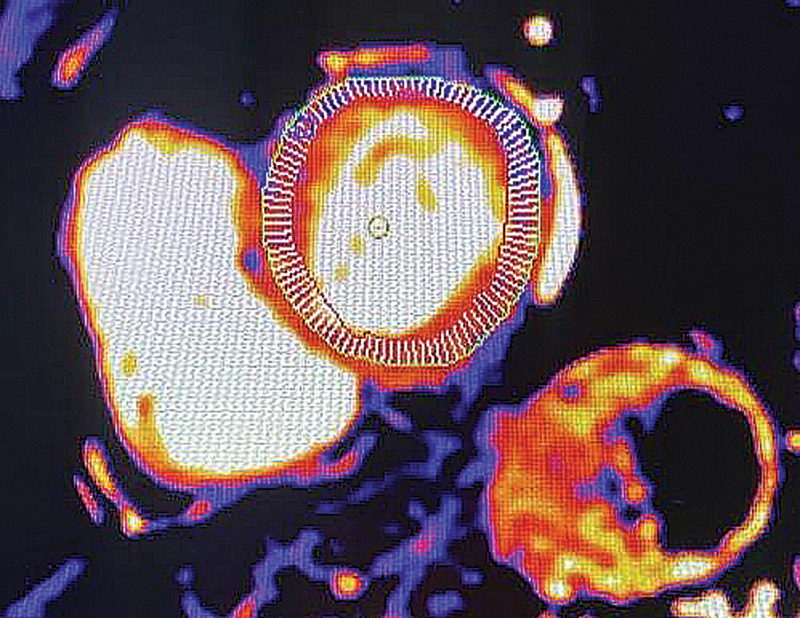
Patient 9 developed myocarditis and myositis after the second nivolumab infusion, presenting with chest pain and CTCA grade 3 proximal limb weakness. Laboratory results indicated elevated creatine kinase and troponin levels. Cardiac and proximal muscle imaging showed inflammatory changes (
Fig. 1 A T2-weighted (T2)/short-Tau inversion recovery (STIR) magnetic resonance imaging (MRI) scan of Patient 9's thigh muscles. A mild increase in T2/STIR signal (green arrow) was noted in the right gluteus minimus muscle after pulsotherapy with methylprednisolone, suggesting inflammatory myositis.
Fig. 2 An MRI scan of Patient 9's heart muscles. Tissue analysis using T1-weighted MAPA sequences demonstrates elevated values (1,010 ms, 1.5T) after pulsotherapy with methylprednisolone, suggesting the presence of inflammatory myocarditis.
Patient 10 developed grade-4 ICI-induced hepatitis, leading to the interruption of ipilimumab combined with nivolumab therapy before starting BRAF/MEK inhibitor treatment. After beginning trametinib and dabrafenib, she developed painful erythematous cutaneous nodules on her extremities, along with myalgia. She initiated prednisone, improving symptoms, but her condition worsened when trying to reduce the corticosteroid dosage. The targeted therapy was changed to encorafenib/binimetinib, but the patient continued to experience skin lesions that were refractory to corticoid-sparing treatment due to prior immunotherapy use. Then, MTX started with 10 mg/day of prednisone. After discontinuing steroids, the patient achieved resolution of erythema nodosum-like lesions using a weekly dose of 20 mg MTX combined with encorafenib/binimetinib, despite experiencing mild nausea and hair loss. She had a complete response to systemic cancer therapy.
Rheumatologic irAE occurred in around 16% of the patients with metastatic cutaneous melanoma who received immunotherapy, according to a retrospective study of 415 patients between 2014 and 2020.
In some cases, high-dose corticosteroids are required, particularly for severe ICI-related myositis, a potentially life-threatening condition.
American and European guidelines recommend 1 to 2 mg/kg of intravenous methylprednisolone or a higher dose bolus (500–1,000 mg/day for 3 days) for ICI-related myositis and myocarditis in the presence of severe symptoms of weakness or cardiac compromise.
The use of BRAF/MEK inhibitors rarely lead to severe irAEs requiring corticosteroid pulses, such as small vessel vasculitis, uveitis, and papillitis.
Preclinical studies have shown that BRAF inhibitors enhance antigen presentation and boost T-cell recognition of tumor antigens. Meanwhile, MEK inhibitors promote an increase in effector CD8 + T-cells within the tumor microenvironment. As a result, patients treated with BRAF/MEK inhibitors following ICI may experience enhanced immune-cell function and antigen presentation, along with an extended half-life of monoclonal antibodies induced by immunotherapy.
In the present case series, all patients with AID continued systemic cancer therapy after controlling irAEs or flares. Furthermore, seven of ten patients received a low dose of a DMARD (MTX in the majority) to maintain stable immune-mediated disease while minimizing corticosteroid use. In clinical practice, we avoid using glucocorticoids or doses exceeding 10 mg/day when an alternative therapy is available, particularly in older patients.
Although this study had a limited sample size and lasted 6 months, it reported two cases where the combination of MTX therapy with BRAF/MEK inhibitors effectively controlled inflammatory symptoms in both joints and skin. Most case series described corticosteroid monotherapy, dose reduction, or suspension of small-molecule kinase inhibitors to manage irAE. Some reports of irAEs induced by BRAF/MEK inhibitors described the use of MTX to treat asymptomatic aortitis in preexisting RA, rituximab for granulomatosis with polyangiitis, and etanercept for toxic epidermal necrolysis.
Patients who required enhanced immunosuppression to control inflammatory activity were preferentially treated with TCZ due to its antitumor properties and effectiveness as a DMARD. Some studies suggested that IL-6 inhibitors may be an alternative DMARD for patients at high risk for irAEs, with intense activity of preexisting AID, or for patients requiring ICI rechallenge (NCT03999749, NCT04940299).
On the other hand, prospective studies are needed to clarify the safety of TNFi in melanoma patients treated with ICI. The use of ABA should be avoided as a DMARD for ICI-induced arthritis, as it inhibits T-cell activation.
When prescribing SSZ to anti-PD-1/PD-L1 users, caution is necessary due to the risk of hypersensitivity. The present case series highlights two patients with differing outcomes: one experienced severe adverse events induced by SSZ during ICI treatment, and another managed her arthritis successfully with SSZ after discontinuing ICI.
Furthermore, leflunomide (LFN) reduces T-cell clonal expansion and may impair the antitumoral effects of ICI.
The limited understanding of the pathophysiology of irAEs hinders the application of more effective therapeutic strategies. Targeting cytokines or their receptors is crucial for managing inflammatory symptoms, mitigating levels of immunosuppression, and enhancing oncological outcomes. Further studies are necessary to evaluate the effectiveness of agents targeting IL-6, IL-12, IL-17, and IL-23 in managing and preventing rheumatic, dermatological, and gastrointestinal irAEs.
Selecting a DMARD for metastatic melanoma patients requires consideration of its potential synergistic or detrimental effects on tumor behavior, patients' risk profile for irAE, the severity of rheumatic manifestations, ongoing cancer treatments, and any comorbidities. Individual cytokine profiles and specific immune cell types may direct future research for managing irAE. Additionally, the degree of immunosuppression experienced by a patient undergoing concurrent rheumatic and cancer therapy may significantly impact their prognosis and warrants further investigation.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Saginala, K and Barsouk, A and Aluru, J S and Rawla, P and Barsouk, A. Epidemiology of Melanoma. Med Sci (Basel) [online]. 2021, vol. 9, p. 63. https://doi.org/10.3390/medsci9040063 Ver referência
2. Evangelista, GFdB and Figueiredo, A B and Silva, MJdBe and Gollob, K J. Balancing the good and the bad: controlling immune-related adverse events versus anti-tumor responses in cancer patients treated with immune checkpoint inhibitors. Immunother Adv [online]. 2022, vol. 2, p. ltac008. https://doi.org/10.1093/immadv/ltac008 Ver referência
3. Xu, C and Chen, Y P and Du, X J. Comparative safety of immune checkpoint inhibitors in cancer: systematic review and network meta-analysis. BMJ [online]. 2018, vol. 363, p. k4226. https://doi.org/10.1136/bmj.k4226 Ver referência
4. Pantuck, M and McDermott, D and Drakaki, A. To treat or not to treat: Patient exclusion in immune oncology clinical trials due to preexisting autoimmune disease. Cancer [online]. 2019, vol. 125, p. 3506-3513. https://doi.org/10.1002/cncr.32326 Ver referência
5. Leipe, J and Mariette, X. Management of rheumatic complications of ICI therapy: a rheumatology viewpoint. Rheumatology (Oxford) [online]. 2019, vol. 58, p. vii49-vii58. https://doi.org/10.1093/rheumatology/kez360 Ver referência
6. Khan, S A and Pruitt, S L and Xuan, L and Gerber, D E. Prevalence of Autoimmune Disease Among Patients With Lung Cancer: Implications for Immunotherapy Treatment Options. JAMA Oncol [online]. 2016, vol. 2, p. 1507-1508. https://doi.org/10.1001/jamaoncol.2016.2238 Ver referência
7. Cortellini, A and Buti, S and Santini, D. Clinical Outcomes of Patients with Advanced Cancer and Pre-Existing Autoimmune Diseases Treated with Anti-Programmed Death-1 Immunotherapy: A Real-World Transverse Study. Oncologist [online]. 2019, vol. 24, p. e327-e337. https://doi.org/10.1634/theoncologist.2018-0618 Ver referência
8. Cappelli, L C and Gutierrez, A K and Bingham, C O and Shah, A A. Rheumatic and Musculoskeletal Immune-Related Adverse Events Due to Immune Checkpoint Inhibitors: A Systematic Review of the Literature. Arthritis Care Res (Hoboken) [online]. 2017, vol. 69, p. 1751-1763. https://doi.org/10.1002/acr.23177 Ver referência
9. Danlos, F X and Voisin, A L and Dyevre, V. Safety and efficacy of anti-programmed death 1 antibodies in patients with cancer and pre-existing autoimmune or inflammatory disease. Eur J Cancer [online]. 2018, vol. 91, p. 21-29. https://doi.org/10.1016/j.ejca.2017.12.008 Ver referência
10. Haanen, J and Ernstoff, M S and Wang, Y. Autoimmune diseases and immune-checkpoint inhibitors for cancer therapy: review of the literature and personalized risk-based prevention strategy. Ann Oncol [online]. 2020, vol. 31, p. 724-744. https://doi.org/10.1016/j.annonc.2020.03.285 Ver referência
11. Min, H Y and Lee, H Y. Molecular targeted therapy for anticancer treatment. Exp Mol Med [online]. 2022, vol. 54, p. 1670-1694. https://doi.org/10.1038/s12276-022-00864-3 Ver referência
12. Salzmann, M and Benesova, K and Buder-Bakhaya, K. Arthralgia Induced by BRAF Inhibitor Therapy in Melanoma Patients. Cancers (Basel) [online]. 2020, vol. 12, p. 3004. https://doi.org/10.3390/cancers12103004 Ver referência
13. Heinzerling, L and Eigentler, T K and Fluck, M. Tolerability of BRAF/MEK inhibitor combinations: adverse event evaluation and management. ESMO Open [online]. 2019, vol. 4, p. e000491. https://doi.org/10.1136/esmoopen-2019-000491 Ver referência
14. Penel, N and Blay, J Y and Adenis, A. Imatinib as a possible cause of severe rhabdomyolysis. N Engl J Med [online]. 2008, vol. 358, p. 2746-2747. https://doi.org/10.1056/NEJMc0708896 Ver referência
15. Brown, L J and Weppler, A and Bhave, P. Combination anti-PD1 and ipilimumab therapy in patients with advanced melanoma and pre-existing autoimmune disorders. J Immunother Cancer [online]. 2021, vol. 9, p. e002121. https://doi.org/10.1136/jitc-2020-002121 Ver referência
16. Abdel-Wahab, N and Shah, M and Lopez-Olivo, M A and Suarez-Almazor, M E. Use of Immune Checkpoint Inhibitors in the Treatment of Patients With Cancer and Preexisting Autoimmune Disease: A Systematic Review. Ann Intern Med [online]. 2018, vol. 168, p. 121-130. https://doi.org/10.7326/M17-2073 Ver referência
17. Pan, E Y and Merl, M Y and Lin, K. The impact of corticosteroid use during anti-PD1 treatment. J Oncol Pharm Pract [online]. 2020, vol. 26, p. 814-822. https://doi.org/10.1177/1078155219872786 Ver referência
18. Chasset, F and Pages, C and Biard, L. Single-center study under a French Temporary Authorization for Use (TAU) protocol for ipilimumab in metastatic melanoma: negative impact of baseline corticosteroids. Eur J Dermatol [online]. 2015, vol. 25, p. 36-44. https://doi.org/10.1684/ejd.2014.2471 Ver referência
19. Ricciuti, B and Dahlberg, S E and Adeni, A and Sholl, L M and Nishino, M and Awad, M M. Immune Checkpoint Inhibitor Outcomes for Patients With Non-Small-Cell Lung Cancer Receiving Baseline Corticosteroids for Palliative Versus Nonpalliative Indications. J Clin Oncol [online]. 2019, vol. 37, p. 1927-1934. https://doi.org/10.1200/JCO.19.00189 Ver referência
20. Yeung, C and Kartolo, A and Holstead, R. Safety and Clinical Outcomes of Immune Checkpoint Inhibitors in Patients With Cancer and Preexisting Autoimmune Diseases. J Immunother [online]. 2021, vol. 44, p. 362-370. https://doi.org/10.1097/CJI.0000000000000377 Ver referência
21. Paderi, A and Gambale, E and Botteri, C. Association of Systemic Steroid Treatment and Outcome in Patients Treated with Immune Checkpoint Inhibitors: A Real-World Analysis. Molecules [online]. 2021, vol. 26, p. 5789. https://doi.org/10.3390/molecules26195789 Ver referência
22. Johnson, D B and Sullivan, R J and Menzies, A M. Immune checkpoint inhibitors in challenging populations. Cancer [online]. 2017, vol. 123, p. 1904-1911. https://doi.org/10.1002/cncr.30642 Ver referência
23. Roberts, J and Smylie, M and Walker, J. Hydroxychloroquine is a safe and effective steroid-sparing agent for immune checkpoint inhibitor-induced inflammatory arthritis. Clin Rheumatol [online]. 2019, vol. 38, p. 1513-1519. https://doi.org/10.1007/s10067-019-04451-2 Ver referência
24. Richter, M D and Crowson, C and Kottschade, L A and Finnes, H D and Markovic, S N and Thanarajasingam, U. Rheumatic Syndromes Associated With Immune Checkpoint Inhibitors: A Single-Center Cohort of Sixty-One Patients. Arthritis Rheumatol [online]. 2019, vol. 71, p. 468-475. https://doi.org/10.1002/art.40745 Ver referência
25. Zitouni, N B and Arnault, J P and Dadban, A and Attencourt, C and Lok, C C and Chaby, G. Subacute cutaneous lupus erythematosus induced by nivolumab: two case reports and a literature review. Melanoma Res [online]. 2019, vol. 29, p. 212-215. https://doi.org/10.1097/CMR.0000000000000536 Ver referência
26. Sharma, G and Ojha, R and Noguera-Ortega, E. PPT1 inhibition enhances the antitumor activity of anti-PD-1 antibody in melanoma. JCI Insight [online]. 2020, vol. 5, p. e133225. https://doi.org/10.1172/jci.insight.133225 Ver referência
27. Wabitsch, S and McVey, J C and Ma, C. Hydroxychloroquine can impair tumor response to anti-PD1 in subcutaneous mouse models. iScience [online]. 2020, vol. 24, p. 101990. https://doi.org/10.1016/j.isci.2020.101990 Ver referência
28. Mehnert, J M and Mitchell, T C and Huang, A C. BAMM (BRAF Autophagy and MEK Inhibition in Melanoma): A Phase I/II Trial of Dabrafenib, Trametinib, and Hydroxychloroquine in Advanced BRAFV600-mutant Melanoma. Clin Cancer Res [online]. 2022, vol. 28, p. 1098-1106. https://doi.org/10.1158/1078-0432.CCR-21-3382 Ver referência
29. McCarter, K R and Arabelovic, S and Wang, X. Immunomodulator use, risk factors and management of flares, and mortality for patients with pre-existing rheumatoid arthritis after immune checkpoint inhibitors for cancer. Semin Arthritis Rheum [online]. 2024, vol. 64, p. 152335. https://doi.org/10.1016/j.semarthrit.2023.152335 Ver referência
30. Vermeulen, O CB and Brouwer, E and Slart, R HJA. Immune checkpoint inhibitor-mediated polymyalgia rheumatica versus primary polymyalgia rheumatica: comparison of disease characteristics and treatment requirement. Rheumatology (Oxford) [online]. 2024, vol. 64, p. 771-779. https://doi.org/10.1093/rheumatology/keae099 Ver referência
31. Papadopoulos, T and Santinon, F and Hudson, M and Del Rincon, S V. Examining methotrexate's safety and efficacy in combination with immune checkpoint inhibitors to control immune related inflammatory arthritis in cancer. J Immunol [online]. 2023, vol. 210, p. 68.03. https://doi.org/10.4049/jimmunol.210.Supp.68.03 Ver referência
32. Ichikawa, K and Ohno, S and Kubo, S and Nakajima, H. Large-vessel vasculitis possibly induced by BRAF and MEK inhibitors for BRAF V600E positive lung adenocarcinoma. BMJ Case Rep [online]. 2024, vol. 17, p. e255958. https://doi.org/10.1136/bcr-2023-255958 Ver referência
33. Challener, G and Kohler, M J and Yokose, C and Yinh, J and Choi, H. POS0139 Safety and efficacy of sulfasalazine in treatment of immune checkpoint inhibitor-inflammatory arthritis. Ann Rheum Dis [online]. 2024, vol. 83, p. 419. https://doi.org/10.1136/annrheumdis-2024-eular.6118 Ver referência
34. Ford, M and Sahbudin, I and Filer, A and Steven, N and Fisher, B A. High proportion of drug hypersensitivity reactions to sulfasalazine following its use in anti-PD-1-associated inflammatory arthritis. Rheumatology (Oxford) [online]. 2018, vol. 57, p. 2244-2246. https://doi.org/10.1093/rheumatology/key234 Ver referência
35. Hammond, S and Olsson-Brown, A and Grice, S. Checkpoint Inhibition Reduces the Threshold for Drug-Specific T-Cell Priming and Increases the Incidence of Sulfasalazine Hypersensitivity. Toxicol Sci [online]. 2022, vol. 186, p. 58-69. https://doi.org/10.1093/toxsci/kfab144 Ver referência
36. Dimitriou, F and Hogan, S and Menzies, A M and Dummer, R and Long, G V. Interleukin-6 blockade for prophylaxis and management of immune-related adverse events in cancer immunotherapy. Eur J Cancer [online]. 2021, vol. 157, p. 214-224. https://doi.org/10.1016/j.ejca.2021.08.031 Ver referência
37. Fa'ak, F and Buni, M and Falohun, A. Selective immune suppression using interleukin-6 receptor inhibitors for management of immune-related adverse events. J Immunother Cancer [online]. 2023, vol. 11, p. e006814. https://doi.org/10.1136/jitc-2023-006814 Ver referência
38. Holmstroem, R B and Nielsen, O H and Jacobsen, S. COLAR: open-label clinical study of IL-6 blockade with tocilizumab for the treatment of immune checkpoint inhibitor-induced colitis and arthritis. J Immunother Cancer [online]. 2022, vol. 10, p. e005111. https://doi.org/10.1136/jitc-2022-005111 Ver referência
39. Hailemichael, Y and Johnson, D H and Abdel-Wahab, N. Interleukin-6 blockade abrogates immunotherapy toxicity and promotes tumor immunity. Cancer Cell [online]. 2022, vol. 40, p. 509-523.e6. https://doi.org/10.1016/j.ccell.2022.04.004 Ver referência
40. Weber, J S and Puranik, A and Mitzutani, T. Interleukin-6 receptor blockade with tocilizumab to reduce immune-related toxicity with ipilimumab and nivolumab in metastatic melanoma. J Clin Oncol [online]. 2024, vol. 42, p. 9538. https://doi.org/10.1200/JCO.2024.42.16_suppl.9538 Ver referência
41. Petit, P F and Daoudlarian, D and Latifyan, S. Tocilizumab provides dual benefits in treating immune checkpoint inhibitor-associated arthritis and preventing relapse during ICI rechallenge: the TAPIR study. Ann Oncol [online]. 2025, vol. 36, p. 43-53. https://doi.org/10.1016/j.annonc.2024.08.2340 Ver referência
42. Johnson, D H and Zobniw, C M and Trinh, V A. Infliximab associated with faster symptom resolution compared with corticosteroids alone for the management of immune-related enterocolitis. J Immunother Cancer [online]. 2018, vol. 6, p. 103. https://doi.org/10.1186/s40425-018-0412-0 Ver referência
43. Cappelli, L C and Brahmer, J R and Forde, P M. Clinical presentation of immune checkpoint inhibitor-induced inflammatory arthritis differs by immunotherapy regimen. Semin Arthritis Rheum [online]. 2018, vol. 48, p. 553-557. https://doi.org/10.1016/j.semarthrit.2018.02.011 Ver referência
44. Montfort, A and Filleron, T and Virazels, M. Combining Nivolumab and Ipilimumab with Infliximab or Certolizumab in Patients with Advanced Melanoma: First Results of a Phase Ib Clinical Trial. Clin Cancer Res [online]. 2021, vol. 27, p. 1037-1047. https://doi.org/10.1158/1078-0432.CCR-20-3449 Ver referência
45. Van Not, O J and Verheijden, R J and Van den Eertwegh, A JM. Association of Immune-Related Adverse Event Management With Survival in Patients With Advanced Melanoma. JAMA Oncol [online]. 2022, vol. 8, p. 1794-1801. https://doi.org/10.1001/jamaoncol.2022.5041 Ver referência
46. Bass, A R and Abdel-Wahab, N and Reid, P D. Comparative safety and effectiveness of TNF inhibitors, IL6 inhibitors and methotrexate for the treatment of immune checkpoint inhibitor-associated arthritis. Ann Rheum Dis [online]. 2023, vol. 82, p. 920-926. https://doi.org/10.1136/ard-2023-223885 Ver referência
47. Ma, V T and Lao, C D and Fecher, L A and Schiopu, E. Successful use of secukinumab in two melanoma patients with immune checkpoint inhibitor-induced inflammatory arthropathy. Immunotherapy [online]. 2022, vol. 14, p. 593-598. https://doi.org/10.2217/imt-2021-0274 Ver referência
48. Li, Y J and Msaouel, P and Campbell, M and Hwu, P and Diab, A and Kim, S T. Successful management of pre-existing psoriatic arthritis through targeting the IL-23/IL-17 axis in cancer patients receiving immune checkpoint inhibitor therapy: a case series. RMD Open [online]. 2024, vol. 10, p. e004308. https://doi.org/10.1136/rmdopen-2024-004308 Ver referência
49. Dimitriou, F and Cheng, P F and Saltari, A. [object Object]. Nat Cancer [online]. 2024, vol. 5, p. 1390-1408. https://doi.org/10.1038/s43018-024-00810-4 Ver referência
50. Asher, N and Bar-Hai, N and Ben-Betzalel, G. Exploring the clinical significance of specific immune-related adverse events in melanoma patients undergoing immune checkpoint inhibitor therapy. Melanoma Res [online]. 2024, vol. 34, p. 439-449. https://doi.org/10.1097/CMR.0000000000000985 Ver referência
51. Nakagomi, Y and Tajiri, K and Shimada, S. Immune Checkpoint Inhibitor-Related Myositis Overlapping With Myocarditis: An Institutional Case Series and a Systematic Review of Literature. Front Pharmacol [online]. 2022, vol. 13, p. 884776. https://doi.org/10.3389/fphar.2022.884776 Ver referência
52. YCU irAE Working Group. Incidence and Distinct Features of Immune Checkpoint Inhibitor-Related Myositis From Idiopathic Inflammatory Myositis: A Single-Center Experience With Systematic Literature Review and Meta-Analysis. Front Immunol [online]. 2021, vol. 12, p. 803410. https://doi.org/10.3389/fimmu.2021.803410 Ver referência
53. Schneider, B J and Naidoo, J and Santomasso, B D. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J Clin Oncol [online]. 2021, vol. 39, p. 4073-4126. https://doi.org/10.1200/JCO.21.01440 Ver referência
54. ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol [online]. 2022, vol. 33, p. 1217-1238. https://doi.org/10.1016/j.annonc.2022.10.001 Ver referência
55. Jespersen, M S and Fanø, S and Stenør, C and Møller, A K. A case report of immune checkpoint inhibitor-related steroid-refractory myocarditis and myasthenia gravis-like myositis treated with abatacept and mycophenolate mofetil. Eur Heart J Case Rep [online]. 2021, vol. 5, p. ytab342. https://doi.org/10.1093/ehjcr/ytab342 Ver referência
56. Solimando, A G and Crudele, L and Leone, P. Immune Checkpoint Inhibitor-Related Myositis: From Biology to Bedside. Int J Mol Sci [online]. 2020, vol. 21, p. 3054. https://doi.org/10.3390/ijms21093054 Ver referência
57. Salem, J E and Bretagne, M and Abbar, B. Abatacept/Ruxolitinib and Screening for Concomitant Respiratory Muscle Failure to Mitigate Fatality of Immune-Checkpoint Inhibitor Myocarditis. Cancer Discov [online]. 2023, vol. 13, p. 1100-1115. https://doi.org/10.1158/2159-8290.CD-22-1180 Ver referência
58. Mössner, R and Zimmer, L and Berking, C. Erythema nodosum-like lesions during BRAF inhibitor therapy: Report on 16 new cases and review of the literature. J Eur Acad Dermatol Venereol [online]. 2015, vol. 29, p. 1797-1806. https://doi.org/10.1111/jdv.13039 Ver referência
59. Grogan, N and Swami, U and Bossler, A D and Zakharia, Y and Milhem, M. Toxicities with targeted therapies after immunotherapy in metastatic melanoma. Melanoma Res [online]. 2018, vol. 28, p. 600-604. https://doi.org/10.1097/CMR.0000000000000493 Ver referência
60. Xia, C Y and Wang, D Y and Mason, R. Activity of targeted therapy after failure of first-line immunotherapy in BRAF-mutant metastatic melanoma. J Clin Oncol [online]. 2018, vol. 36, p. 9532. https://doi.org/10.1200/JCO.2018.36.15_suppl.9532 Ver referência
61. Vanneman, M and Dranoff, G. Combining immunotherapy and targeted therapies in cancer treatment. Nat Rev Cancer [online]. 2012, vol. 12, p. 237-251. https://doi.org/10.1038/nrc3237 Ver referência
62. Yordanova, K and Pföhler, C and Schweitzer, L F and Bourg, C and Adam, L and Vogt, T. Etanercept leads to a rapid recovery of a Dabrafenib-/Trametinib-associated toxic epidermal necrolysis-like severe skin reaction. Skin Health Dis [online]. 2022, vol. 3, p. e185. https://doi.org/10.1002/ski2.185 Ver referência
63. Cappelli, L C and Shah, A A and Bingham, C O. Immune-Related Adverse Effects of Cancer Immunotherapy- Implications for Rheumatology. Rheum Dis Clin North Am [online]. 2017, vol. 43, p. 65-78. https://doi.org/10.1016/j.rdc.2016.09.007 Ver referência
64. Salem, J E and Allenbach, Y and Vozy, A. Abatacept for Severe Immune Checkpoint Inhibitor-Associated Myocarditis. N Engl J Med [online]. 2019, vol. 380, p. 2377-2379. https://doi.org/10.1056/NEJMc1901677 Ver referência

Dados de acesso insuficientes para visualização no mapa.