Colorectal cancer (CRC) is the third most common neoplasm and the second most lethal worldwide.
The most common histological type is adenocarcinoma, characterized by its glandular pattern.
MCC morphologically presents itself with layers of malignant cells with vesicular nuclei, prominent nucleoli, and infiltration by intraepithelial lymphocytes, with little or no glandular differentiation.
Due to its clinical, immunohistology, and genetic peculiarities, and because it has recently been recognized by the World Health Organization (WHO) as a histological variant distinct from the others,
The present study reports a case in an academic general surgery service of a 74-year-old patient who presented with a tumor of the ascending colon, histologically with exuberant lymphocytic infiltrate, suggestive of large cell lymphoma, but which by subsequent immunohistochemistry was revealed to be medullary colon carcinoma with microsatellite instability (MSI).
Furthermore, due to the rarity of the pathology, a literature review was carried out on the subject to contribute to the knowledge of the disease, facilitating the recognition of the pathology and the management of future similar cases.
Retrospective cross-sectional observational study, carried out by collecting data from medical records and reviewing narrative literature, searching for articles, and using related keywords, on the main medical research platforms (PubMed and SciELO). Furthermore, an informed consent form was provided, with guidance on the possible risks of the research, guaranteeing data anonymity and authorization to analyze data from the patient’s medical records to report the case.
A 74-year-old female patient with a history of hypertension presented with a history of anorexia, asthenia, and weight loss of 14kg over a period of 3 months, without other associated symptoms. During physical examination, an abdominal mass was identified at the epigastrium-umbilical transition, which continued the investigation with abdominal ultrasound and subsequent contrast-enhanced CT scan of the abdomen, which revealed an expansive lesion in the right iliac fossa measuring 68x66mm.
A colonoscopy was performed, which revealed a lesion with a neoplastic appearance, ulcerative-infiltrative in the topography of the cecum (
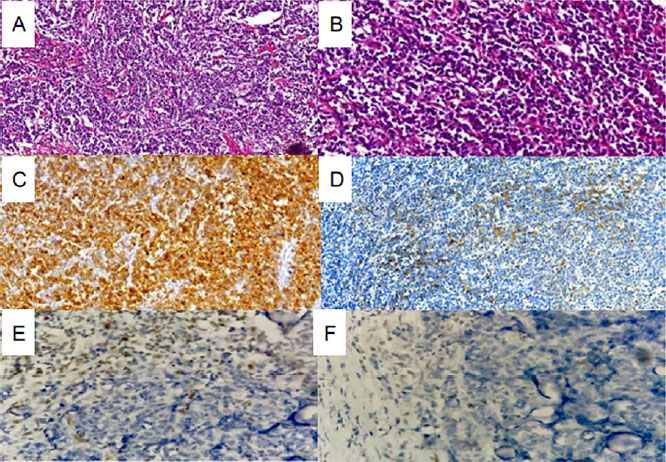
Figure 1 Histopathological and immunohistocheinistry findings. Table 2. (A and B) MCC sections showed an infiltrative edge-pushing pattern and a focal anaplastic and discohesive appearance (H&E. × 100 and × 400. respectively). (C and D) CK Pool with diffuse positivity and CK7 with focal positivity (immunohistochemistry). (E And F) neoplastic cell nuclei in both images completely devoid of immunohistochemical staining, while adjacent lymphocytes that permeate the tumor show nuclear staining for MLH1 and PMS2 respectively.
A surgical approach was chosen for the patient, and a large tumor mass located in the cecum was found intraoperatively, with a segment of the small intestine attached to it and multiple lymph nodes adjacent to the mesentery. An enterectomy of approximately 40cm was performed, involving the small segments and lymph nodes attached to the tumor mass, followed by an extended right ileocolectomy in oncology with subsequent lateral-lateral ileoanastomosis.
The anatomopathological result of the surgical specimen showed, on macroscopy, an ulcerative tumor lesion in the ceco-colon mucosa, measuring 7.6x7.0cm, infiltrating the muscularis wall and ileocecal valve.
Microscopy of the specimen showed extensive proliferation of lymphoid cells, of medium and large cells, with oval nuclei, irregular chromatin, and evident nucleoli, arranged in sheets, with foci of necrosis, infiltrating to the subserosa, suggestive of lymphoma, in addition to the presence of lymph nodes reactive hyperplastic.
To establish the differential diagnosis, immunohistochemistry was performed on the analyzed pieces, demonstrating positivity for CK7 and CK POLL (see
| Antibody Panel Studies |
|---|
| Expression by Antibody |
| CD20 (-) CD3 (-) CD5 (-) BCL2 (-) BCL6 (-) CD30 (-) MUM-1 (-) CD23 (-) CD10 (-) CHROMOGRANIN A (-) SYNAPTOPHYSIN (-) CD56 (-) DESMOSINE (-) CD1A (-) TDT (-) CD34 (-) CD117 (-) CD138 (-) MYOGENIN |
| (-), VIMENTINA (-) CD45 (-) PAX-5 (-) OCT 3/4 (-) DOG-1 (-) S100 (-) HMB-45 (-) CD68 (-) CD43 (-) MYELOPEROXIDASE(-) CK20 (-) TTF-1 (-) CDX2 (-) PSA (-) CK5/6 (-) CALRETENINA (-) MLH1 (-) PMS2 (-) |
| KI-67 (+) 95%, CYCLIN D1 (+) in few cells, C-MYC (+) in few cells, CD99 (+) in few cells, CK POOL (+) diffused, CK7 (+) focal MSH2 (+) MSH6 (+) |
Subsequently, the patient was referred to clinical oncology for adjuvant evaluation, opting for clinical observation every three months.
MCC is a rare subtype of colorectal carcinoma first described in 1999 by Jessurun et al.
The lack of glandular differentiation can be misinterpreted as a poorly differentiated or undifferentiated adenocarcinoma, among other unusual patterns that may be present and lead it to be characterized as lymphoma, neuroendocrine tumor, or metastasis, and its real incidence may be underestimated.[4] According to a retrospective study carried out by Scott et al. (2021)
MCC of the colon has a predilection for the right side of the colon in 70 to 100%, more precisely in the proximal portion (74%), affecting female patients with an average age of 69.3 years, typically associated with abdominal pain and change in bowel habits.
The treatment of MCC of the colon is very similar to colon adenocarcinoma, with the surgical approach as the gold standard. Adjuvant chemotherapy is not usually applied, since patients with IMS do not usually respond to fluoropyrimidines.
According to a recent edition of the WHO Classification of Gastrointestinal Tumors, medullary carcinomas present an aberrant phenotype, with loss of CDX2 and CK20
Despite these defined characteristics, diagnosis can be challenging. Additional studies reported more detailed characterization to improve the diagnostic algorithm. Winn et al.
In conclusion, the case reports the presence of a rare colon cancer in the population. Due to the limited knowledge about this disease and the few cases reported in the literature, the clinical findings may be inconclusive, and the diagnosis difficult. Thus, further studies are needed to elucidate the management and molecular analysis of this type of cancer.
| MWMCS | Collection and assembly of data, Conception and design, Manuscript writing |
| Collection and assembly of data, | |
| JWFG | Conception and design, Final approval of manuscript, Provision of study materials or patient |
| EVA | Data analysis and interpretation, Provision of study materials or patient |
| ISC | Collection and assembly of data, Conception and design, Final approval of manuscript, Manuscript writing, Provision of study materials or patient |
| GSF | Collection and assembly of data, Data analysis and interpretation, Manuscript writing |
| MMN | Collection and assembly of data, Conception and design, Data analysis and interpretation, Manuscript writing |
| LSP | Final approval of manuscript, Provision of study materials or patient |
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references found for this article.
Dados de acesso insuficientes para visualização no mapa.