Pancreatic cancer represents the seventh leading cause of cancer mortality in the world, and the second leading cause of cancer death in the United States
Due to the low survival associated with this neoplasia, different research has directed efforts to identify predictive markers that help to optimize the treatment. Among them, the carbohydrate antigen 19-9 (CA19-9), the performance index evaluated by the ECOG (Eastern Cooperative Oncology Group), age, local therapies, and the status of chronic inflammation represented by the neutrophil/lymphocyte (NLR) and platelet/lymphocyte (PLR) ratio
These last two have been particularly studied due to the advance in the knowledge of immunology in cancer. The NLR is calculated from the absolute values of neutrophils and lymphocytes obtained through the blood count. Many studies indicate that a low NLR (usually less than four or five) is associated with better survival in patients with metastatic pancreatic cancer
Finally, has been studied if local therapy can improve survival in patients with locally advanced pancreatic cancer. A series of cases from a retrospective study by the Johns Hopkins group, for example, showed that patients with locally advanced pancreatic cancer who underwent radiation therapy, at some point in their treatment, had a median overall survival of 13.7 months and 61% disease control in one year
The present study evaluated the clinical and epidemiological characteristics and the factors that influenced the survival of patients with metastatic and unresectable locally advanced pancreatic adenocarcinoma, treated in a private reference hospital for the treatment of cancer in the Brazilian state of Pernambuco.
Ours is a longitudinal analytical study with a retrospective and prospective part.
Patients with histological diagnosis of locally advanced or metastatic pancreatic adenocarcinoma who received chemotherapy treatment were selected from the medical archives of the Real Instituto de Oncologia of Hospital Português. The period of diagnosis and treatment was between January 2012 and December 2018, with a minimum of 12 months of follow-up. All patients ongoing active therapy or best supportive care between July 2019 to December 2019 was included in the analyses and represents the prospective part of the study, if they were alive and have completed 12 months of follow-up until December 2019.
Clinical oncology service of the Real Hospital Português and data collected from electronic medical records from July 2019 to December 2019.
Adult patients (> 18 years old)
Histological diagnosis of pancreatic adenocarcinoma Stage III or IV
Patients who underwent at least one chemotherapy treatment session
Medical data on treatment and clinical follow-up available in medical records Minimum of 12-month follow-up period
Patients without the complete data required for the study
Loss of continued service follow-up
Another active tumor (except non-melanoma skin cancer)
To characterize the studied sample, the relative (percentage) and absolute (N) frequencies of the classes of each qualitative variable were calculated. For quantitative variables, averages and medians were used to summarize the information, and standard, minimum and maximum deviations to indicate data variability. The level of significance assumed is 5%. Statistical analyzes were performed using SPSS - Statistical Package for Social Sciences, version 21.0 (IBM, Armonk, NY).
For survival analysis, death was considered an event of interest. Initially, we calculated the survival probabilities for the total number of patients using the Kaplan-Meier method. Such a method allows the survival curve to be constructed with estimates of the probabilities of survival as a function of the followup time. Thus, it is possible to know the chance that a patient will survive “so many” months after the diagnosis. These estimates are independent of the patient's condition; that is, information about other measures of the patient is not being considered here. To assess the influence of these variables, such as Clinical Staging, ECOG, NLR and PLR, Kaplan-Meier curves were constructed for the categories of each qualitative variable. In this type of analysis, a significance test is performed for each variable that indicates whether the variable in question influences the patient's survival. To compare the curves, we used the Log-Rank test. The results (graphs and test results) are shown below.
The research was approved by the Human Research Ethics Committee of Pernambuco's Real Hospital Português de Beneficência. Opinion Number: 3.705.999.
Forty-three medical records of patients diagnosed with locally advanced or metastatic pancreatic adenocarcinoma were identified in the oncology department. Eight patients were treated in another center and therefore excluded due to loss of followup. Finally, thirty-five patients met all inclusion and exclusion criteria. Most patients were diagnosed between 2016 and 2018 (n=31). The average age was 68 years old, and greater than 70% of patients were older than 65 years of age. Other clinical, demographic and laboratory characteristics are shown in
| Clinical Demographics Characteristics | N (%) |
|---|---|
| Age (years) Mean | 68.9; SD ±10.3 |
| Median | 68 |
| Range | 44 - 85 |
| Age (years) < 65 | 10 (28.6) |
| = 65 | 25 (71.4) |
| Gender Male | 23 (65.7) |
| Female | 12 (34.3) |
| ECOG 0 and 1 | 23 (65.7) |
| 2 and 3 | 12 (34.3) |
| Clinical Staging Locally advanced | 11 (31.4) |
| Metastatic | 24 (68.6) |
| NLR < 4 | 21 (61.8) |
| = 4 | 13 (38.2) |
| Unknown | 1 |
| PLR < 150 | 14 (41.2) |
| = 150 | 20 (58.8) |
| Unknown | 1 |
| CA 19.9 < 250 | 16(48.5) |
| = 250 | 17 (51.5) |
| Unknown | 1 |
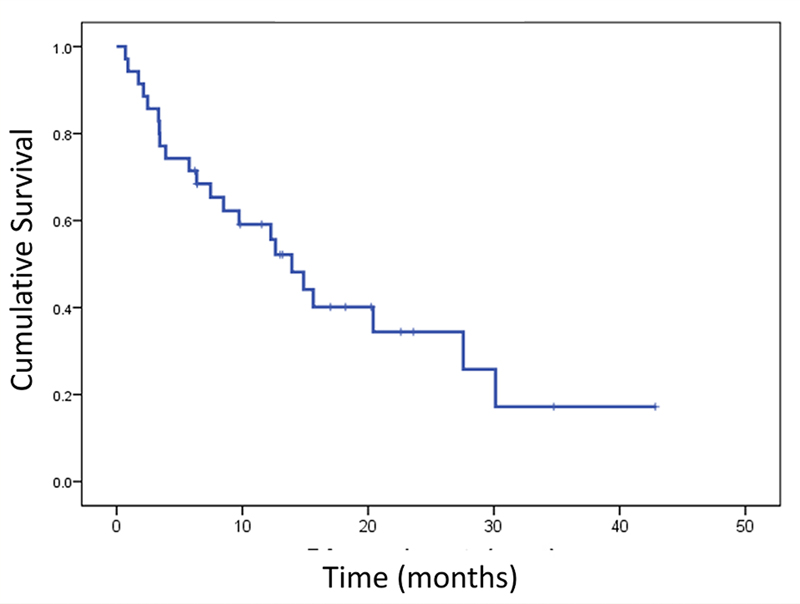
The median survival for our entire cohort was 13.39 months, as shown in
Figure 1 Median Survival of the entire cohort (n=35 patients; Median survival 13.93 months [95% CI; 9.96 - 17.90])
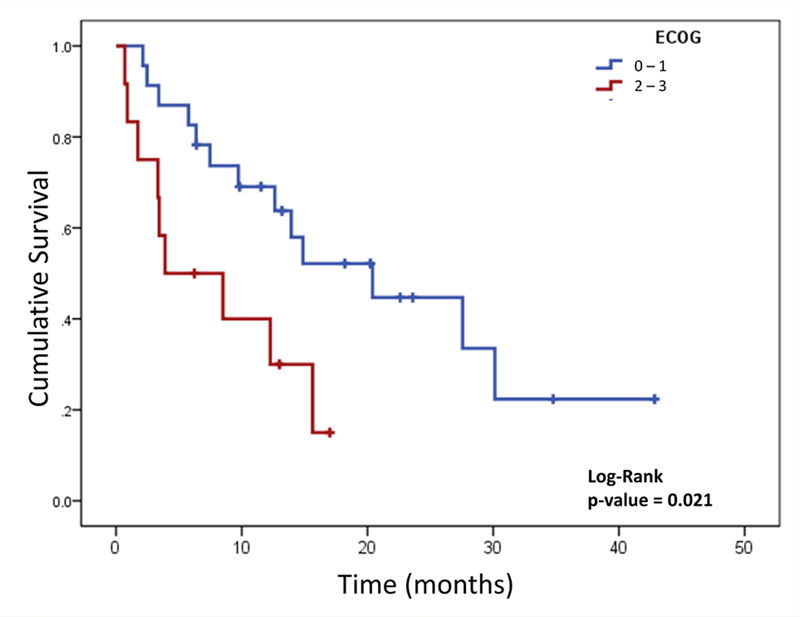
Figure 2 Median survival according to ECOG performance status. ECOG 0 and 1: 13 deaths, median survival 20.4 months (95% CI, 9.05 - 31.74); ECOG 2 and 3: 9 deaths, median survival 3.9 months (95% CI,1.00 - 11.72).
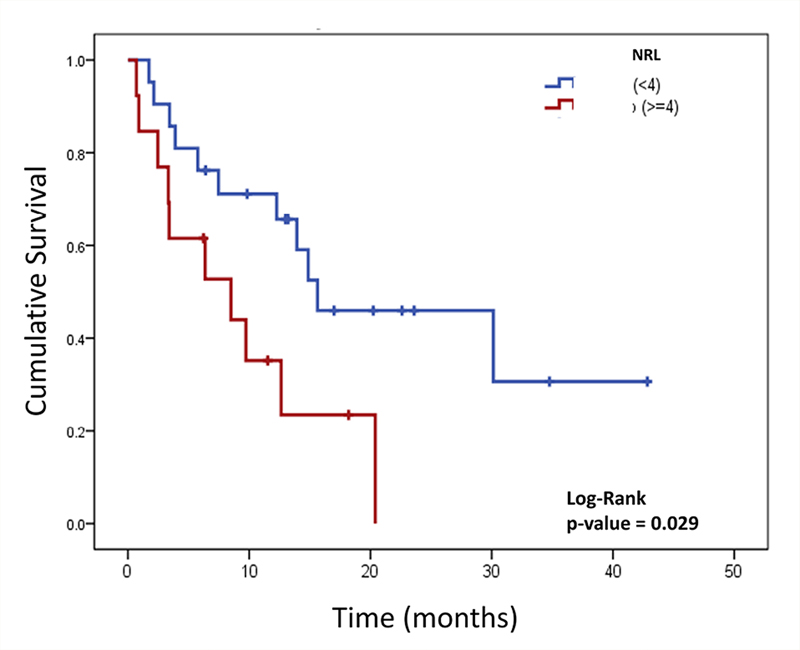
Figure 3 Median survival according to Neutrophil/lymphocyte ratio (NLR). NLR < 4 : 11 deaths, median survival 15.63 months (95% CI, 2.17 - 29.10); NLR > ou = 4: 10 deaths, median survival 8,5 months (95%, CI 0.39 - 16.61).
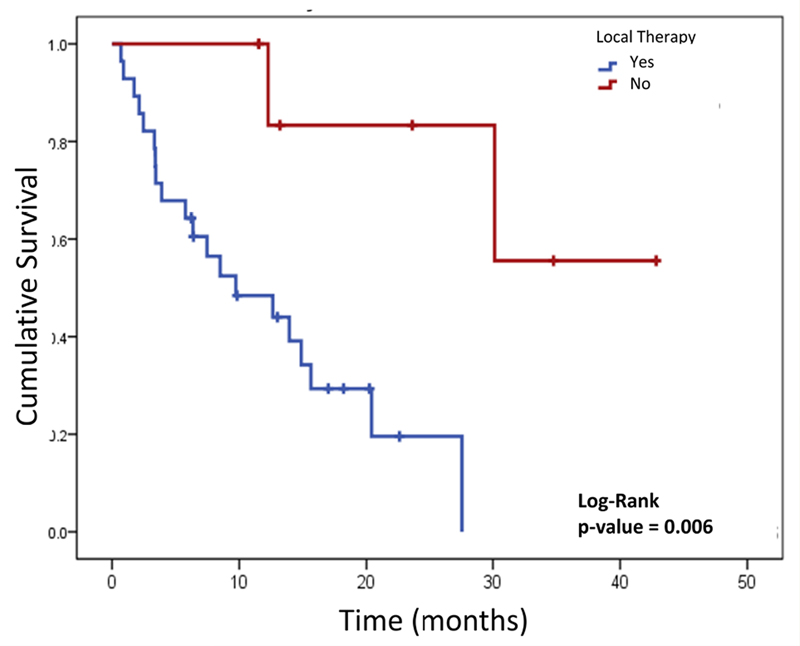
Figure 4 Median survival according to local therapy use during treatment. Local therapy group: 2 deaths, median survival 23.68 months (95% IC, 11.23 - 35.17); Non local therapy group: 20 deaths, median survival 9.73 months (95% IC, 1.85 - 17.61). Local therapy used was radiation therapy or radiofrequency ablation (4 patients with metastatic disease and 3 patients with locally advanced disease).
| Variable | N | Median survival (months) | Deaths | 95% IC | p-value |
|---|---|---|---|---|---|
| Age (years) <65 | 10 | 14.87 | 05 | 5.58 - 24.15 | 0.270 |
| =65 | 25 | 13.93 | 17 | 6.25 - 21.61 |
|
| Clinical Staging Locally Advanced | 11 | 13.93 | 7 | 7.88 - 19.99 | 0.653 |
| Metastatic | 24 | 14.87 | 15 | 6.29 - 23.44 |
|
| ECOG 0 - 1 | 23 | 20.4 | 13 | 9.05 - 31.74 | 0.021 |
| 2 - 3 | 12 | 3.9 | 9 | 1.00 - 11.72 |
|
| NLR < 4 | 21 | 15.63 | 11 | 2.17 - 29.10 | 0.029 |
| = 4 | 13 | 8.5 | 10 | 0.39 - 16.61 |
|
| PLR < 150 | 14 | 20.4 | 8 | 2.42 - 38.38 | 0.436 |
| = 150 | 20 | 12.27 | 13 | 6.87 - 17.67 |
|
| CA 19-9 < 250 | 16 | 15.01 | 7 | 9.22 - 18.77 | 0.519 |
| = 250 | 17 | 13.93 | 13 | 5.91 - 21.96 |
|
| Local therapy Yes | 07 | 23.68 | 2 | 11.23 - 35.17 | 0.006 |
| No | 28 | 9.73 | 20 | 1.85 - 17.1 |
|
ECOG (Eastern Cooperative Oncology Group. ECOG 0, n =1; ECOG 1, n =22; ECOG 2, n =11; ECOG 3, n =1); NLR (neutrophil / lymphocyte ratio, n=34); PLR (platelet / lymphocyte ratio, n=34); CA 19-9 (carbohydrate antigen 19-9, n=33);
Local therapy (n=7 [4 patients with locally advanced disease and 3 patients with metastatic disease) ; radiotherapy, n=6; radioablation, n=1); for survival analysis, the Kaplan-Meier model was used and comparisons were assessed using the Log-Rank test. The p value was considered statistical when p <0.05.
Of the 35 treated patients, 11 had locally advanced disease, and 24 had metastatic disease at diagnosis. In locally advanced disease, FOLFIRINOX was the first line of treatment in nine patients (81%). Twenty-eight patients (24 with initial metastatic disease and 4 with locally advanced disease who developed metastases) received first- line therapy. FOLFIRINOX (18 patients, 64.3%), Gemcitabine plus nab-paclitaxel (5 patients, 18%), and gemcitabine monotherapy (4 patients, 14%) were the most widely used chemotherapy regimens. The median survival for first-line patients who received FOLFIRINOX was 12 months (n=27), and those who received gemcitabine + nab- paclitaxel was 13 months (n=5). Seventeen patients (70.8%) with metastatic disease received a second line of chemotherapy treatment. Gemcitabine plus nab-paclitaxel and gemcitabine alone were used as second-line in 41% and 29% of the patients, respectively.
Between ECOG 2 patients (n=11) the first line therapy was gemcitabine alone (n=5), FOLFIRINOX (n=4), and gemcitabine plus nab-paclitaxel (n=2), only three patients received a second line with was gemcitabine plus nab-paclitaxel (n=1), FOLFOX (n=1) and fluorouracil plus leucovorin (n=1). ECOG 3 patient (n=1) received FOLFIRINOX as first line followed by gemcitabine as monotherapy.
The present study observed a median overall survival of 13.93 months in patients with unresectable and metastatic locally advanced pancreatic adenocarcinoma-results superior to those found in the two main studies in this group of patients. Those studies observed a higher overall survival for FOLFIRINOX (11.1 months) and the combination gemcitabine plus nab-paclitaxel (8.5 months) in the first line of treatment when compared with gemcitabine alone
The ability to predict poor survival for patients with a disease as severe as pancreatic cancer is essential in the initial management before treatment to select patients most likely to receive polychemotherapy such as FOLFIRINOX and gemcitabine plus nab-paclitaxel. For that, possible factors associated with worse survival were evaluated, such as age, disease stage, ECOG, NLR, PLR, CA 19-9, and the use of local therapy.
The median age observed was 68 years old, above that reported in the PRODIGE and MPACT studies, which were 61 and 62 years old, respectively
Our sample did not show any difference in overall survival when comparing the locally advanced and metastatic clinical stages (13.9 months x 14.8 months; p=0.653). However, despite data in the literature pointing to better survival in locally advanced disease
About one-third of our population had ECOG 2 (n=11, 31.4%), which is different from that observed in clinical studies, where the majority of patients are recruited with better performance. Therefore, more real-life studies are essential to assess the impact of treatments on clinical practice. In the MPACT study 8% of the patients included had ECOG 2 and this group of patients had a worse survival when compared with those with better ECOG
Another prognostic factor that has been widely studied is the inflammatory factor. The search for markers of systemic inflammation measured by pretreatment NLR and PLR is a prognostic factor in several studies, which point to a worse survival outcome in patients with elevated NLR and PLR
The CA 19-9 marker is also studied as a prognostic factor for pancreatic cancer, with contradictory results and variable cut-off points. In some studies, a high value before treatment predicts advanced disease, unresectability, recurrence, and worse overall survival
With regard to local therapy, some studies indicate better survival in patients with advanced disease who receive local treatment (radiotherapy or radioablation) at some point in their treatment
As limitations for the present study, we can mention the retrospective and single- centered design and the small number of participants. On the other hand, our study presents information from our daily clinical practice with survival data similar to those observed in phase III clinical studies.
In conclusion, good clinical condition (ECOG 0 or 1), low NLR, and local therapy are associated with better survival in univariate analysis, suggesting their clinical usefulness and applicability in the treatment of locally advanced or metastatic pancreatic cancer.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.