Differentiated thyroid carcinoma (DTC) is rare in children, ranging from 0.3-0.5% of all pediatric neoplasms, but remains the most common endocrine malignancy in this age group and represents the third most common pediatric solid tumor.
More recently, rearrangements of other protooncogenes have also been observed in papillary thyroid cancer (PTC) in association with exposure to ionizing radiation, with gene fusions activating the MAPK signaling pathway: the three NTRK genes (NTRK1, NTRK2, and NTRK3) each encode a distinct TRK protein, such as TRKA, TRKB and TRKC, respectively.
Pan-TRK IHC staining using clone EPR17341 (Abcam, Cambridge, MA), a rabbit recombinant monoclonal antibody, can assess the protein expression and has been used in several recent studies with a sensitivity and specificity of around 85-90% and 80%, respectively. Although this method is widely used, its effectiveness is still questionable, and another method is needed to confirm the positive cases. The most used confirmation method is the NGS that has a high sensitivity of virtually 100% in RNA based sequencing.
In order to evaluate the main tests used in clinical practice for NTRK fusion detection in pediatric thyroid cancer, the objective of this study was to investigate pan-TRK IHC sensitivity and specificity in DTC samples from CAYA patients correlated with NGS method. In our study, IHC were chosen for NTRK fusion screening because of it’s low cost, easy execution and availability and NGS was elected as the second method considering the sensitivity of this technique.
We performed a retrospective multicenter crosssectional study with 79 cases of DTC in CAYA patients 21 years or younger diagnosed and treated at four centers: (i) Aristides Maltez Hospital (HAM), Salvador- Brazil; (ii) IT - Instituto Integrado de Endocrinologia e Cirurgia, Salvador, Brazil; (iii) Santa Casa de Misericórdia (SCMFS), Feira de Santana, Brazil; and Lauro Wanderley University Hospital (HULW), João Pessoa, Brazil; between January 2010 and March 2021. Non-consecutive patients were selected (non- probabilistic sampling, for convenience) and their tumor samples, fixed in formalin and preserved in paraffin (FFPE) blocks, resulting from surgical resections of the thyroid performed by the head and neck surgery services of the respective hospitals.
The cases were selected after researching patients who were diagnosed with malignant thyroid neoplasms on anatomopathological examination (code C.73, according to the International Statistical Classification of diseases and Related Health Problems; ICD) and who were registered in a database available in the internal electronic system of the services of pathological anatomy from participating centers with diagnosis of DTC. After the selection of patient, a search was performed for the respective slides stained with hematoxylin- eosin (HE), previously prepared at the time of the anatomopathological diagnosis, as well as the respective paraffin blocks containing tumor tissue. Both blocks and blades were kept in their respective services. On occasions when slides were absent or inadequate for evaluation and identification of the tumor area, new slides were made and stained with HE. To confirm the diagnosis of DTC, the HE slides were subjected to blind-review by two pathologists linked to the institutions participating in the study (M.V.P., R.S.).
Tumor slides were classified according to the World Health Organization’s World Tumor Classification criteria and staged according to the AJCC Cancer Staging Manual, 8th edition.
Tumor tissue was obtained through histological sections of paraffin blocks containing samples of carcinomas stored in the archives of the respective pathology services of the participating institutions. Four sequential 10µm-thick histological sections were performed for each case/block to make new slides, which were superimposed on their corresponding HE slides, with the tumor areas previously marked. The areas of tumor tissue from the new slides were manually dissected with sterile 6 disposable razors (Leica Biosystems, Germany) and transferred to microtubes (1.5ml), previously autoclaved and identified, and stored at room temperature until processing. In cases of multifocality, all tumor foci were selected, but only the most extensive focus was used in the study.
IHC staining for expression of TRK A, B and C was performed with pan-TRK monoclonal antibody (mAb) clone EPR17341 (Abcam, Cambridge, MA). The antibody is reactive to a homologous region of TRK-A, -B, and -C near the C-terminus. IHC was performed using 4µm thick slides of sections of paraffinized tumor tissue from selected tumor blocks with representative material. EPR17341 was used at 6µg/ml, at 1:200 dilution. All assays were performed on a Dako Autostainer Link 48 automated staining platform (Agilent, Santa Clara, CA) using a heatbased antigen retrieval method and high pH buffer (EnVision Flex High pH, Agilent). Testicular tissue, submucosal colonic plexus ganglia, and cortical brain tissue were used as positive control tissues non-neoplastic lymphocytes, hepatocytes, colorectal epithelium, alveolar epithelium, and renal cortex were used as negative external controls. Available cases with NTRK rearrangements, as well as 10 consecutive tumors with no evidence of NTRK fusion, were stained as controls. The slides were evaluated and reviewed by 2 pathologists. Label positivity was defined as any unambiguous cytoplasmic and/or nuclear immunopositivity with clear contrast with the surrounding non-tumor tissue. The percentage of stained cells positivity and staining intensity were documented: (i) Pan-TRK negative: 0% stained cells; and (ii) Pan-TRK positive: 1% stained cells. All 79 IHC pan-TRK tested samples were than analyzed with a RNA-based NGS assay in order to confirm IHC pan- TRK result and elucidate fusion partner.
NGS was performed using the Illumina platform with the Oncomine Focus Assay kit for RNA fusion analysis, capable of evaluating all classes of relevant targets, including point mutations, short insertions, or deletions (indels), copy number variants (CNVs) and gene fusions, adapted for formalin-fixed and paraffin-embedded (FFPE) tissues. Three FFPE slides with a section of 5µm thickness were obtained per tumor sample, sufficient to provide about 10ng of DNA or RNA per reaction. This allowed analysis even on small-sized or inferior-quality tumor samples. Three 5µm FFPE cuts were used to extract DNA of somatic origin with the ReliaPrep™ FFPE RNA Miniprep System, Promega (Madison, WI, USA). Quality was verified with Qubit™ RNA HS Assay Kit assay (LifeTechnologies, USA). cDNA synthesis was performed with 7 Ampliseq™ cDNA Synthesis for Illumina® (USA), according to the manufacturer’s recommendations. Genotyping of target genes ABL1, ALK, AKT3, AXL, BRAF, EGFR, ERBB2, ERG, ETV1, ETV5, ETV4, FGFR1, FGFR2, FGFR3, NTRK1, NTRK2, NTRK3, PDGFRA, PPARG, RAF1, RET, ROS1 and MET were performed by NGS on the iSeq 100 Sequencing System platform, Illumina Inc (USA), mean sequencing depth 300x. Bioinformatics analyzes were conducted on the cloud-based Varstation™ platform with a standardized pipeline exclusively for technology and laboratory, considering the rules of the Association for Molecular Pathology (AMP).
The following variables will be analyzed: age at the time of surgery, sex, tumor size, histological subtype, multifocality, extrathyroidal extension, presence of tumor capsule and capsular invasion, angiolymphatic invasion, perineural invasion, Hashimoto’s thyroiditis (TH), lymph node metastases, cancer staging, recurrence risk stratification, positivity for BRAFV600E mutation. Data processing and data analysis will be performed with the assistance of the Statistical Package for the Social Sciences (SPSS), version 22, using nonparametric tests, according to the categorical variables of the research.
The normal distribution analysis will be evaluated using the Shapiro-Wilk test. Univariate analyzes (χ2 test and Fisher>s exact test) will be performed to assess the associations between clinical and pathological aspects and the presence of NTRK or PTC fusions. The implication between such associations will be based on the p-value <0.05, determined with confidence intervals of 95%.
This work was carried out in accordance with Resolution No. 466/2012 of the National Health Council (CNS). The project was submitted for ethical analysis in the electronic system of Plataforma Brasil, a national and unified database of research involving human beings, and was evaluated and approved by the Ethics and Research Committees in Human of the Health Sciences Institute, Federal University of Bahia (CEP/ICS), HAM, SCFMS and HULW, according to Opinion No.4.319.796(CAAE:34192920.6.0000.5662).
This research was carried out with financial resources from the pharmaceutical company Bayer under contract number BR135321023503P, managed by the intervener FAPEX, case number 23066.020493/2020-97.
The median age at diagnosis observed in the sample studied was 18 years (range: 6-21 years). Thirty patients (38%) were under 18 years and forty- nine (62%) were aged between 18 and 21 years. Relation to gender, the vast majority were female (77%). Clinical-pathological characteristics of the patients are presented in Table 1.
All 79 tumors samples were submitted to pan-TRK IHC for NTRK fusion screening. Most tumor samples 64/79 (81%) were negative. Only 03 (3,8%) cases had positive pan-TRK expression and 12 of 79 (15%) cases had indeterminate staining (Table 2). Among positive cases: 1 case with 1% of staining cells and 2 samples with 10% staining cells. All positive samples demonstrated weak, focal, and nuclear staining (Figure 1).
NGS was performed on the 3 pan-TRK IHC positive cases and on 64 pan-TRK IHC negative samples, including 21 cases with MAPK pathway activation by known mutations (BRAF p.V600E, KRAS/NRAS hotspot). 39/74 (52.7%) had inconclusive results, 10/74 (13.5%) were positive for a rearrangement and 25/74 (33.8%) were classified as wild type.
Only 35 of 79 NGS-RNA sequencing tests were considered valid: 10 samples had positivity for gene fusions. Among the 10 positive cases for gene fusions: 04 were of the NTRK gene; 03 were of the RET gene; 02 were of PAX8::PPARG rearrangement; and 01 of the STRN:ALK gene fusion (Table 3).
| Variables | Total | <18 years | >18 years |
|---|---|---|---|
| 79 (100.0%) | 30 (37,9%) | 49 (62,1%) | |
| Age (years), median | 18 (6-21) | 17 (6-17) | 19 (18-21) |
| Sex, n(%) | |||
| Female | 61 (77,2) | 14 | 47 |
| Male | 18 (22,8) | 8 | 10 |
| Histological subtype, n(%) | |||
| CPTC | 66 (83,5) | 14 | 52 |
| FVPTC | 9 (11,4) | 2 | 7 |
| FTC | 3 (3,8) | 1 | 2 |
| DSPTC | 1 (1,3) | 1 | 0 |
| T staging, n(%) | |||
| T1a | 9 (11,3) | 3 | 6 |
| T1b | 22 (27,8) | 4 | 18 |
| T2 | 22 (27,8) | 5 | 17 |
| T3a | 6 (7,5) | 4 | 2 |
| T3b | 17 (21,5) | 4 | 13 |
| T4 | 3 (3,7) | 0 | 3 |
| N staging, n(%) | |||
| N0 | 38 (48,1) | 12 | 26 |
| N1a | 21 (26,5) | 3 | 18 |
| N1b | 20 (25,3) | 5 | 15 |
| M staging, n(%) | |||
| M1 | 8 (10,2) | 1 | 7 |
| Tumor size(cm), median | 2.2 (0,3-7,5) | 2 (0,5-7,5) | 2,3 (0,3-6,8) |
| Focality, n (%) | |||
| Multifocal | 28 (35,5) | 10 | 18 |
| Extrathyroidal invasion, n(%) | |||
| Positive | 21 (26,5) | 7 | 14 |
| Angiolymphatic invasion, n(%) | |||
| Positive | 7 (8,8) | 2 | 5 |
| ATA risk, n(%) | |||
| low risk | 34 (43) | 8 | 26 |
| intermediate risk | 16 (20,2) | 3 | 13 |
| high risk | 29 (36,7) | 8 | 21 |
Legend: ATA - American Thyroid Association; CPTC - classic papillary thyroid carcinoma; DSPTC- diffuse sclerosing papillary thyroid carcinoma; FTC - follicular thyroid carcinoma; FVPTC - follicular variant papillary thyroid carcinoma
| Age (y) | n (%) | indeterminate | positive | negative |
|---|---|---|---|---|
| 79 (100%) | 12/79 (15%) | 3/79 (3,8%) | 64/79 (81%) | |
| <18 | 28 | 4 | 1 | 23 |
| > 18 | 51 | 8 | 2 | 41 |
| Age | Sex | Histological Subtype | TNM staging | Fusion detected |
|---|---|---|---|---|
| 20 | F | CPTC | T2N1bM1 | ETV::NTRK3 |
| 15 | F | CPTC | T1bN0M0 | ETV6::NTRK3 |
| 13 | F | CPTC | T1aN0M0 | ETV6::NTRK3 |
| 12 | F | CPTC | T3N1bM1 | TPR::NTRK1 |
| 18 | F | FTC | T2N0M0 | PAX8::PPARG |
| 17 | F | CPTC | T2N0M0 | PAX8::PPARG |
| 14 | F | CPTC | T2N1bM0 | CCDC6::RET |
| 11 | F | CPTC | T1bN1bM0 | TRIM24::RET |
| 6 | F | SDPTC | T3bN1bM0 | NCOA4::RET |
| 11 | F | CPTC | T3bN0M0 | STRN::ALK |
Legend: ALK - Anaplastic Lymphoma Kinase; CCD6 - Coiled-Coil Domain Containing 6; CPTC- Classic variant of papillary thyroid carcinoma.; FTC - follicular thyroid carcinoma; SDPTC - Scleroing diffuse variant of papillary thyroid carcinoma; ETV6 - ETS variant transcription factor 6; NCOA4 - nuclear receptor coactivator 4; NTRK1- neurotrophic receptor tyrosine kinase1; NTRK3 - neurotrophic receptor tyrosine kinase 3; PAX8 - Paired box gene 8 - peroxisome proliferator-activated receptor; PPARG - peroxisome proliferator activated receptor gamma; RET- Rearranged during transfection; TPR - translocated promoter region; TRIM24 - Tripartite motif-containing 24; STRN - striatin, calmodulin binding protein.
NTRK gene fusion was detected in 04/35 valid tests (11,4%): (i) 03/35 (8,5%) ETV6::NTRK3 and (ii) 01/35 (2,8%) TPR::NTRK1.
Pan-TRK IHC was negative in all 4 NTRK NGS- positive cases. Pan-TRK IHC and NGS concordance analysis: 25 of 79 NTRK NGS-negative control cases had concordant negative pan-TRK IHC results. Therefore, our rate of false positivity to pan-TRK IHC result was 3/25 (12%) (Table 4).
The overall results for pan-TRK IHC in our cohort of NGS-negative cases was: (i) sensitivity (0%), (ii) specificity (96%), (iii) positive predictive value (94.7%), and (iv) negative predictive value (91%) (Table 5).Table 1. Demographics and Clinicopathological features of differentiated thyroid cancer in children, adolescents, and young adults (n=79).
| IHC positive | IHC negative | |
|---|---|---|
| NGS positive | 0 | 4 |
| NGS negative | 3 | 25 |
| False positive | 0 | 03 /25 (12%) |
| Sensitivity | 0% |
|---|---|
| Specificity | 96% |
| Positive predictive value | 94,7% |
| Negative predictive value | 91% |
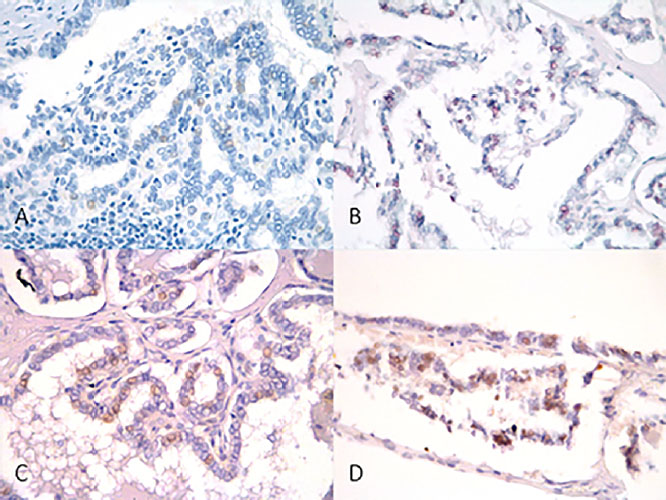
Figure 1. Pan-TRK immunohistochemistry. A. 200x, negative case; B. 200x, weak nuclear staining (1% cells); C and D. 200x, weak nuclear staining (10% cells).
The study aimed to determine the IHC sensitivity and specificity in DTC NTRK gene fusions in CAYA patients. This is the largest cohort of CAYA DTC cases stained with pan-Trk IHC, and it is the first to detail the sensitivity and specificity of pan-TRK IHC regarding the data obtained by targeted RNA-based NGS panel in DTC.
All NTRK positive tumors in our casuistry was papillary histological subtype, most frequent neoplasm found in pediatric population and the most related to NTRK fusions. Despite the majority (62%) were aged between 18 and 21 years, in our study, gene fusions were more detected in young patients (under 18-year-old), with a median of 14 years. This gene fusion greater occurrence in younger age is in accordance with the literature.
Due to the multiple technologies available for the detection of NTRK fusions, one question is whether there is a better method for its evaluation, if we consider cost-effectiveness, given the high cost of performing these diagnostic tests, especially for NGS. Choosing the most appropriate method depends on the type of tumor being studied and the broader strategy for detecting other biomarkers of this neoplasm, as well as the clinical situation.
In the rare case of tumor types with a high frequency of specific and pathognomonic NTRK fusions, investigation with initial IHC is the cheapest, quickest, and most effective way of screening. This is a plausible screening option; however, a second method of investigation, such as RT-PCR, FISH or NGS, is recommended.
Although there are several TRK antibodies available, the EPR 17341 clone has been the most widely used. This antibody detects the C-terminal region of TRK proteins A, B and C, therefore being considered pan-TRK. Overall, pan-TRK IHC is a sensitive technique for identifying NTRK fusions, with a reported overall sensitivity of 85 to 90% and specificity around 80%, but detection of TRKC is less sensitive.
Ideally, positive cases should also be confirmed again by a second technique.
In this study, all 79 tumor samples from this series were submitted to IHC for TRK overexpression. Only 03 (3.7%) tumor samples were pan-TRK positive (3.7%): 1 sample with 1% positive cells and 2 samples with 10% positive cells. In our sample, samples were classified as pan-TRK positive when they had at least 1% of antibody-positive cells. The positive cellularity found was 1% in 1 case and 10% in other 2 cases. All samples positive for IHC showed a nuclear staining pattern with weak intensity in the reaction.
The cutoff point for determining whether a case is positive ranges from 1 to 10%, and there are several patterns of positivity for pan-TRK on IHC. While most NTRK fusions show cytoplasmic labeling, the pattern of labeling in thyroid tissue is variable and depends on the partner where the specific fusion is present and can be nuclear, cytoplasmic, and membranous, or demonstrate a combination of patterns.
However, in our study, none of them was NTRK fusion confirmed, with 1 tumor with negative results and 2 tumors with inconclusive results at NGS, configuring false-positive results. Thus, the frequency of NTRK fusions in the 3 tumor samples from patients with IHC-positive DTC was 0%.
Overall, the sensitivity in detect raised TRK expression by pan-TRK IHC is higher in NTRK1 and NTRK2 fusions, where sensitivity is usually 90%, than in detecting NTRK3. In fact, the ETV6::NTRK3 fusion probably has the lowest detection rate of all fusion proteins, at around 50%.
The specificity is very variable, depending on the type of tumor. While the antibody demonstrates 100% specificity in colon, lung, thyroid, pancreas and biliary tract carcinomas, specificity decreases in breast and salivary gland carcinomas.
Using the same pan-TRK monoclonal antibody (mAb) clone EPR17341 (Abcam, Cambridge, MA), Hechtman et al reported high sensitivity (95.2%) and specificity (100%) of IH in paraffin-embedded samples from several types of cancer (intestinal, brain, lung, secretory carcinoma, melanoma and sarcoma) (16). In agreement, Rudzinski et al. (2018)
DNA-based NGS has about 70% sensitivity for NTRK3 fusion whereas RNA-based NGS has virtually 100% sensitivity, but it is an expensive technology with a long lead time of about two weeks to perform. It is important to keep in mind that the absence of labeling does not exclude the possibility of this diagnosis, as there is a high rate of false-negative results in the detection of the ETV6-NTRK3 fusion, for example.
In the NGS gene fusion panel, the frequency of NTRK fusions was 11.4% (04 cases), with all cases being pan-TRK negative, suggesting a low sensitivity of IHC as a fusion tracking method NTRK. The overall results for pan-TRK IHC in our cohort of NGS-negative cases was: (i) sensitivity (0%), (ii) specificity (96%). However, it is possible that some cases considered false-positive by IHC may be false-negative results by the NGS fusion panel.
Although IHC is a technique capable of detecting increased levels of the TRK protein, and can be a very useful screening technology to reduce costs, in this study, given the presented data, IHC alone has not proven to be a definitive diagnostic methodology to detect NTRK gene fusions in pediatric and young adult DTC in the evaluated population. Even so, due to the great practicality of using IHC, this method should not be excluded as a method of screening NTRK fusions in clinical practice, however it is suggested that the investigation of the NTRK fusion by NGS should be, whenever possible, the preferred technique in tracking this fusion in DTC of children, adolescents and young adults.
It’s possible that the prevalence of NTRK fusions in this present casuistry was underestimated, considering the large number of inconclusive results in NGS. Out of the 79 included samples, only 35 were evaluated (less than half of the initial sample size).
The reasons for this were little availability of tumor sample or degraded tumor material: low-quality, inadequate conservation, small sample, degraded RNA, fixing time and paraffin block age. Additionally, methodological fragility as non-probability sampling may have contributed for NTRK fusion underestimation in our study. Despite that, the obtained sample size can be considered sufficient for the final conclusions considering the ultimate pediatric cohort series in the literature.
Pan-TRK IHC was not a tissue-efficient screen for NTRK fusions in DTC from CAYA patients. In our study, there was absolute disagreement between the IHC and NGS tests for tracking NTRK fusion in DTC. All NTRK fusions were identified only by the NGS method, with a negative result prior to IHC and in no tumor sample positive by IHC there was confirmation of the fusion by NGS. Therefore, the IHC screening test was not able to identify tumors carrying the NTRK fusion in the tumor samples of our study, suggesting a low sensitivity of the IHC as a NTRK fusion screening method.
The frequency of NTRK fusions was 11.4% in this study.
There was disagreement between the IHC and NGS tests for tracking NTRK fusion.
NGS should be the preferred technique in tracking NTRK fusion in DTC from CAYA patients.
This work was carried out in accordance with Resolution No. 466/2012 of the Conselho Nacional de Saúde (CNS). The project underwent ethical review in the electronic system of Plataforma Brasil, a unified national database for research involving human subjects. It was assessed and approved by the Ethics Committees for Research at the Institute of Health Sciences of the Federal University of Bahia (CEP/ICS), Liga Baiana Contra o Câncer (CEP/LBCC/HAM), and Gerência de Ensino e Pesquisa (GEP/HULW), as per Substantiated Opinion No. 5,470,375.
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
This work was financially supported by Bayer, under contract number BR135321023503P, administered by the intermediary Foundation for Research and Extension SupportFunda (FAPEX), project number 200038.
| AJCC | American Joint Committee on Cancer |
| ANVISA | National Agency of Sanitary Monitoring |
| ATA | American Thyroid Association |
| BRAF | V-raf murine sarcoma viral oncogene |
| CEP | Ethics and Research Committees in Human |
| CNS | National Health Council |
| CPTC | Classic variant of papillary thyroid carcinoma |
| DNA | Deoxyribonucleic acid |
| DTC | Differentiated Thyroid Cancer |
| FDA | U.S Food and Drug Administration |
| FFPE | Formalin-fixed paraffin-embedded |
| FTC | Follicular Thyroid Carcinoma |
| HAM | Aristides Maltez Hospital |
| HE | Hematoxilina-eosina |
| HULW | Lauro Wanderley University Hospital |
| International Statistical | |
| ICD | Classification of Diseases and Related Health Problems |
| ICS | Institute of Health Sciences |
| FISH | Fluorescence in situ hybridization |
| IHC | Immunohistochemistry |
| NGS | Next generation sequence |
| NTRK | Neurotrophic receptor tyrosine kinase |
| RT-PCR | Reverse transcription polymerase chain reaction |
| PTC | Papillary thyroid carcinoma |
| RNA | Ribonucleic acid |
| SCMFS | Santa Casa de Misericórdia de Feira de Santana |
| SDPTC | Sclerosing diffuse variant of papillary thyroid carcinoma |
| TNM | Classification of malignant tumors |
| TRK | Tropomyosin receptor kinase |
| UFBA | Federal University of Bahia |
| WT | Wild type |
| ACOTT | Collection and assembly of data, Manuscript writing |
| GJRM | Collection and assembly of data, Data analysis and interpretation, Manuscript writing |
| JLVA | Collection and assembly of data, Data analysis and interpretation, Manuscript writing |
| RRCM | Collection and assembly of data, Manuscript writing |
| TLCO | Collection and assembly of data, Data analysis and interpretation, Manuscript writing |
| FELB | Data analysis and interpretation, Manuscript writing |
| ARP | Provision of study materials or patient, Manuscript writing |
| FH | Data analysis and interpretation, Manuscript writing |
| GCL | Data analysis and interpretation, Manuscript writing |
| LFBR | Provision of study materials or patient, Manuscript writing |
| BSL | Provision of study materials or patient, Manuscript writing |
| HER | Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing |
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Tamam, M and Uyanik, E and Edís, N and Mulazimoglu, M and Ozpacaci, T. Differentiated thyroid carcinoma in children: clinical characteristics and long-term follow-up. World J Nucl Med [online]. 2020, vol. 19, p. 28-35.
2. Prasad, PK and Mahajan, P and Hawkins, DS and Mostoufi-Moab, S and Venkatramani, R. Management of pediatric differentiated thyroid cancer: an overview for the pediatric oncologist. Pediatr Blood Cancer [online]. 2020, vol. 67, p. e28141.
3. Russo, M and Malandrino, P and Moleti, M and Vermiglio, F and D’Angelo, A and RosaLa, G. Differentiated thyroid cancer in children: Heterogeneity of predictive risk factors. Pediatr Blood Cancer [online]. 2018, vol. 65, p. e27226.
4. Vriens, MR and Moses, W and Weng, J and Peng, M and Griffin, A and Bleyer, A. Clinical and molecular features of papillary thyroid cancer in adolescents and young adults. Cancer [online]. 2011, vol. 117, p. 259-67.
5. Beimfohr, C and Klugbauer, S and Demidchik, EP and Lengfelder, E and Rabes, HM. NTRK1 re-arrangement in papillary thyroid carcinomas of children after the Chernobyl reactor accident. Int J Cancer [online]. 1999, vol. 80, p. 842-7.
6. Nakagawara, A. TRK receptor tyrosine kinases: a bridge between cancer and neural development. Cancer Lett [online]. 2001, vol. 169, p. 107-14.
7. Sassolas, G and Hafdi-Nejjari, Z and Ferraro, A and Decaussin-Petrucci, M and Rousset, B and Borson-Chazot, F. Oncogenic alterations in papillary thyroid cancers of young 77 patients. Thyroid [online]. 2012, vol. 22, p. 17-26.
8. Gatalica, Z and Xiu, J and Swensen, J and Vranic, S. Molecular characterization of cancers with NTRK gene fusions. Mod Pathol [online]. 2019, vol. 32, p. 147-53.
9. Prasad, ML and Vyas, M and Horne, MJ and Virk, RK and Morotti, R and Liu, Z. NTRK fusion oncogenes in pediatric papillary thyroid carcinoma in northeast United States. Cancer [online]. 2016, vol. 122, p. 1097-110.
10. Pekova, B and Dvorakova, S and Sykorova, V and Vacinova, G and Vaclavikova, E and Moravcova, J. Somatic genetic alterations in a large cohort of pediatric thyroid nodules. Endocr Connect [online]. 2019, vol. 8, p. 796-805.
11. Pekova, B and Sykorova, V and Mastnikova, K and Vaclavikova, E and Moravcova, J and Vlcek, P. NTRK fusion genes in thyroid carcinomas: clinicopathological characteristics and their impacts on prognosis. Cancers [online]. 2021, vol. 13, p. 1932.
12. Solomon, JP and Benayed, R and Hechtman, JF and Ladanyi, M. Identifying patients with NTRK fusion cancer. Ann Oncol [online]. 2019, vol. 30, p. viii16-viii22.
13. Cui, C and Shu, W and Li, P. Fluorescence in situ hybridization: cell-based genetic diagnostic and research applications. Front Cell Dev Biol [online]. 2016, vol. 4, p. 89.
14. Lee, YC and Chen, JY and Huang, CJ and Chen, HS and Yang, AH and Hang, JF. Detection of NTRK1/3 rearrangements in papillary thyroid carcinoma using immunohistochemistry, fluorescent in situ hybridization, and next-generation sequencing. Endocrine Pathol [online]. 2020, vol. 31, p. 348-58.
15. Albert, CM and Davis, JL and Federman, N and Casanova, M and Laetsch, TW. TRK fusion cancers in children: a clinical review and recommendations for screening. J Clin Oncol [online]. 2019, vol. 37, p. 513-24.
16. Hechtman, JF and Benayed, R and Hyman, DM and Drilon, A and Zehir, A and Frosina, D. Pan-TRK Immunohistochemistry. Is an efficient and reliable screen for the detection of NTRK Fusions. Am J Surg Pathol [online]. 2017, vol. 41, p. 1547-51.
17. Amin, MB and Edge, SB and Greene, FL and Byrd, DR and Brookland, RK and Washington, MK. AJCC cancer staging manual [Internet]. Springer, 2017.
18. Lloyd, RV and Osamura, RY and Klöppel, G and Rosai, J. Cancer IA for R on 2017. Lyon, 2017.
19. Haugen, BR and Alexander, EK and Bible, KC and Doherty, GM and Mandel, SJ and Nikiforov, YE. American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid [online]. 2016, vol. 26, p. 1-133.
20. Marchiò, C and Scaltriti, M and Ladanyi, M and Iafrate, AJ and Bibeau, F and Dietel, M. ESMO recommendations on the standard methods to detect NTRK fusions in daily practice and clinical research. Ann Oncol [online]. 2019, vol. 30, p. 1417-27.
21. Jennings, LJ and Arcila, ME and Corless, C and Kamel-Reid, S and Lubin, IM and Pfeifer, J. Guidelines for validation of nextgeneration sequencing based oncology panels: a joint consensus recommendation of the Association for Molecular Pathology and College of American Pathologists. J Mol Diagn [online]. 2017, vol. 19, p. 341-65.
22. Märkl, B and Hirschbühl, K and Dhillon, C. NTRK-Fusions - a new kid on the block. Pathol Res Pract [online]. 2019, vol. 215, p. 152572.
23. Lassen, U. How I treat NTRK gene fusion-positive cancers. ESMO Open [online]. 2019, vol. 4, p. e000612.
24. Abel, HJ and Duncavage, EJ. Detection of structural DNA variation from next generation sequencing data: a review of informatic approaches. Cancer Genet [online]. 2013, vol. 206, p. 432-40.
25. Brzeziańska, E and Pastuszak-Lewandoska, D and Lewiński, A. Rearrangements of NTRK1 oncogene in papillary thyroid carcinoma. Neuro Endocrinology Letters [online]. 2007, vol. 28, p. 221-9.
26. Grego, A and Miranda, C and Pierotti, MA. Rearrangements of NTRK1 gene in papillary thyroid carcinoma. Mol Cell Endocrinol [online]. 2010, vol. 321, p. 44-9.
27. Sabour, L and Sabour, M and Ghorbian, S. Clinical applications of next-generation sequencing in cancer diagnosis. Pathol Oncol Res [online]. 2017, vol. 23, p. 225-34.
28. Ronsley, R and Rassekh, SR and Shen, Y and Lee, AF and Jantzen, C and Halparin, J. Application of genomics to identify therapeutic targets in recurrent pediatric papillary thyroid carcinoma. Cold Spring Harb Mol Case Stud [online]. 2018, vol. 4, p. a002568.
29. Hsiao, SJ and Zehir, A and Sireci, AN and Aisner, DL. Detection of tumor NTRK gene fusions to identify patients who may benefit from tyrosine kinase (TRK) inhibitor therapy. J Mol Diagn [online]. 2019, vol. 21, p. 553-71.
30. Kummar, S and Lassen, UN. TRK Inhibition: a new tumor-agnostic treatment strategy. Target Oncol [online]. 2018, vol. 13, p. 545-56.
31. Rudzinski, ER and Lockwood, CM and Stohr, BA and Vargas, SO and Sheridan, R and Black, JO. Pan-TRK Immunohistochemistry identifies NTRK rearrangements in pediatric mesenchymal tumors. Am J Surg Pathol [online]. 2018, vol. 42, p. 927-35.
32. Solomon, JP and Linkov, I and Rosado, A and Mullaney, K and Rosen, EY and Frosina, D. NTRK fusion detection across multiple assays and 33,997 cases: diagnostic implications and pitfalls. Mod Pathol [online]. 2020, vol. 33, p. 38-46.
33. Fazeli, S and Dadu, R and Waguespack, SG and Sherman, SI and Busaidy, NL and Hu, MI. MON-491 TRK-fusion thyroid cancer: a clinical overview in a large population at a single cancer center. J Endocr Soc [online]. 2020, vol. 4, p. 491.
Dados de acesso insuficientes para visualização no mapa.