Nasopharyngeal carcinoma (NPC) is an uncommon malignant tumor that originates from the epithelial cells lining the surface of the nasopharynx. The prevalence of NPC is typically less than 1 per 100,000 person-years, accounting for approximately 0.25% of all cancers diagnosed worldwide.
Patients often manifest nonspecific symptoms in the early stages of NPC, including headache, dizziness, and unexplained weight loss, which can further delay diagnosis and appropriate intervention.
The treatment of cancer requires a comprehensive strategy that includes radiotherapy (RDT), chemotherapy (CHT), and sometimes surgery. The choice of treatment depends on factors such as the size of the tumor, whether it has spread, and the patient’s overall health.
We present the case of a 61-year-old man who was diagnosed with locally advanced nasopharyngeal squamous cell carcinoma.
A 61 -year-old man, a heavy smoker, presents with symptoms of headache, dizziness, and significant weight loss over a 4-month period. Upon worsening of his symptoms, he sought medical attention in the emergency room where a CT scan of the skull revealed a malignant process in the nasopharynx characterized by infiltration and destruction of surrounding structures including the clivus, second cervical vertebra, and involving the right sphenoid sinus with associated lysis of its posterior wall. In addition, partial obstruction of the ipsilateral intrapetrous canal was noted.
Figure 1 Illustrates frontal and sagittal views from a CT scan, highlighting the tumor-induced destruction of the clivus and the accompanying damage to the bony barrier.
Although neurological examination yielded asymptomatic results, laboratory tests revealed hyponatremia due to pituitary involvement secondary to the syndrome of inappropriate antidiuretic hormone secretion (SIADH). Furthermore, a biopsy subsequently confirmed luminal epidermoid carcinoma with a staging of cT4 cN0 M0, which indicates local tumor spread with no regional lymph node involvement or distant metastases.
Upon diagnosis, the treatment consisted of RDT with 70 Gy applied by LINAC Siemens ONCOR® plan with multilayer collimator and a 3DRT plan (PCRT system) with the aim of targeting the localized tumor spread while minimizing damage to surrounding healthy tissues. The planning target volume (PTV) encompassed the nasopharyngeal region with both ganglion chains receiving a total dose of 50 Gy delivered at a rate of 2 Gy per day.
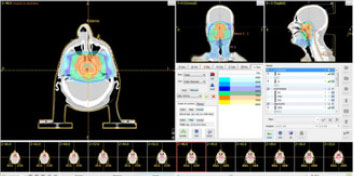
Figure 2 Depicts the CT 3D planning, revealing the destruction of the clivus and the bone barrier caused by the neoplasm.
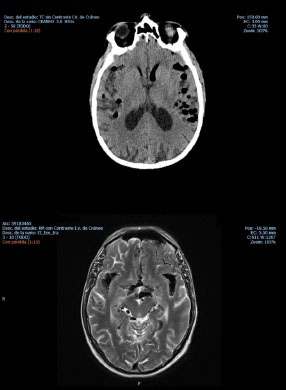
Figure 3 Displays non-contrast computed tomography and magnetic resonance imaging, providing visual evidence of the presence of air bubbles within the brain.
During the first weeks of treatment, the patient experienced fatigue, dysphagia, and mild xerostomia with negligible eyelid drooping. After 6 weeks of treatment, CT scans showed an incomplete regression of the NPC due to the presence of significant residual tumor. He was hospitalized for 4 months with headache, fluctuating level of consciousness, spatial disorientation, drowsiness, left-sided paralysis of the sixth and twelfth cranial nerves, and rhinorrhea suggestive of respiratory infection.
Two weeks later, with no noticeable clinical changes, CT and MRI scans showed a significant improvement in the previously reported tumor remnants; however, scattered bubbles were detected throughout the brain mass. After the tumor disappeared, residual effects persisted as the tumor could still act as a plug obstructing the outflow of cerebrospinal fluid. Subsequently, a fistula formed requiring drainage to the nasopharyngeal area, creating the potential for air bubbles to enter the central nervous system and leading to tension pneumocephalus (TPN).
Direct rhinoscopy revealed persistent cerebrospinal fluid drainage from the fistula, which was identified as the cause of the rhinorrhea. Neurosurgeons and otolaryngologists were consulted regarding a trans-maxillary approach and placement of dural fragments or other materials, but this recommendation was quickly rejected due to insufficient compliance of the irradiated area. The patient died within 2 weeks.
Several environmental factors, including exposure to chemical carcinogens, alcohol consumption, dietary habits, and nitrosamines, as well as genetic predisposition, have been associated with NPC.
NPC typically originates in the fossa of Rosenmüller, located superior and posterior to the torus tubarius, where the mucosal epithelium directly overlies the underlying lymphoid tissue.
In our case, pneumocephalus (PN) emerged as a rare complication, adding a layer of complexity to the clinical presentation of NPC. PN is a neurological emergency characterized by the accumulation of compressed air within the cranial cavity, often associated with accidental decompression, surgical trauma, and impacts involving the face and skull.
Despite significant advances in understanding the pathophysiology of PN, the documentation remains limited, with only six confirmed cases of PN and only four cases of TPN properly documented regarding patients with NPC.
Furthermore, in our case study, we note that osteoradionecrosis (ORN) may have played a significant role in the development of the clivus fistula. Although uncommon, ORN must be considered as a potential contributing factor to TPN associated with NPC. Extensive literature supports the notion of delayed, spontaneous onset of TPN following radiotherapy (RDT). Insights provided by Wu and Lee (1999) and Sumitsawan et al. (2009) shed light on the occurrence of TPN in patients who underwent RDT to the skull base.
In contrast, the mechanism underlying these changes in blood vessels after ionizing radiation exposure is not yet fully understood, leading to nutrient deprivation in the bone marrow and hindering osteoblast production.
In addition, the delayed onset of TPN, observed in our case approximately 5 months after RDT treatment, contrasts with the findings of other studies in which TPN typically manifests approximately 12 months after treatment.
Regardless of the etiology, we are confident that at least two mechanisms can contribute to the formation of TPN. One mechanism, known as “inverted ink bottle,” involves a continuous cerebrospinal fluid (CSF) leak resulting in fluid loss and subsequent intracranial depression.
In our patient, the constellation of symptoms (headache, fluctuating level of consciousness, spatial disorientation, and drowsiness) appears to be pathophysiological linked to decreased intracranial pressure
Alternatively, another theory states that intracranial negative pressure (INP) results from excessive CSF loss due to iatrogenic physiological drainage.
While CT serves as the reference test, in our case report, its combination with MRI represents the optimal approach for diagnosing and monitoring both NPC and complications associated with TPN. Initially, the onset of rhinorrhea was mistakenly attributed to a cold, while the CT scan provided limited information. Abdel and King established CT as the primary modality for staging NPC, providing details on the extent tumor of invasion (T and N), albeit with limitations in imaging intracranial, orbital, and nerve sheath extensions.
Moreover, MRI addresses these limitations, with studies demonstrating its superior efficacy in detecting early-stage NPC due to its accuracy in detecting cervical and retropharyngeal lymph nodes and facilitating patient follow-up due to its ability to differentiate between soft tissue and bone changes.
While previous findings may have provided validation for our treatment decisions, it is imperative to remain cognizant of the critical role that RDT dose plays in preventing ORN-associated complications. This case report serves as a poignant reminder of the delicate balance required in administering RDT, particularly in the context of NPC. By carefully considering the optimal dosage levels and adhering to established protocols, healthcare professionals can reduce the risk of adverse effects such as osteoradionecrosis while ensuring effective tumor control.
In summary, RDT proves to be effective in treating NPC, even when the tumor invades the skull base and may cause complications (e.g., ORN). This suggests that the therapeutic approach used has yielded promising results. However, it is unfortunate that the patient in this clinical case died. This underscores the importance of close monitoring and comprehensive management of complications such as tension pneumocephalus to increase the survival of patients in similar circumstances.
Because of the nature of this report, formal approval by an ethics committee was not required. Informed consent was obtained from all patients for inclusion in the study.
| IMMP | Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing. |
| SEMP | Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing |
| AVM | Collection and assembly of data, Conception and design, Final approval of manuscript, Provision of study materials or patient |
| NKY | Final approval of manuscript |
| MCDC | Collection and assembly of data, Conception and design, Final approval of manuscript |
| CRG | Manuscript writing |
| FRH | Conception and design, Final approval of manuscript, Manuscript writing |
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references found for this article.

Dados de acesso insuficientes para visualização no mapa.