Cervical cancer is a major cause of cancer morbidity and mortality in women. When compared to developed countries, cervical cancer is a public health problem in developing countries like India, so much so that India alone accounts for one-quarter of the worldwide burden of cervical cancers.
It is well known that screening for cancer reduces mortality through early detection and treatment. However, there are two prerequisites for screening to reduce the rate of death from cancer. First, screening must advance the time of diagnosis of cancers that are destined to cause death. Second, early treatment of these cancers must confer some advantage over treatment at clinical presentation.
The success of the screening for cervical cancer has been largely attributed to the using the Papanicolaou smearing test (Pap-test). Cervical cancer is curable if detected early, and the 5-year survival rate is as high as 92%.
This prospective study was undertaken following permission granted by the Institutional/University ethical committee (KLESKF/IEC/2020/23). Women attending the Gynaecology outpatient department formed the potential study group. Women ≥40 years of age underwent routine screening for cervical cancer as a part of the departmental policy. Following clinical examination all women underwent speculum examination. It was ensured that no local douche, antiseptic cream was used on the day of test. The patient was placed in dorsal lithotomy position and a Cusco’s bivalve speculum was introduced through vagina and cervix was visualized. The longer projection of the Ayre’s spatula was placed in the cervix near squamo-columnar junction and rotated through 360°. The cellular material thus obtained was quickly, but gently smeared on a clean glass slide.
The glass slide was then immediately put into the coplin jar containing 95% ethyl alcohol which acted as a fixative. The prepared smears were then stained according to Papanicolaou’s technique. The cytological interpretation of the smears was made according to the New 2014 Bethesda system.
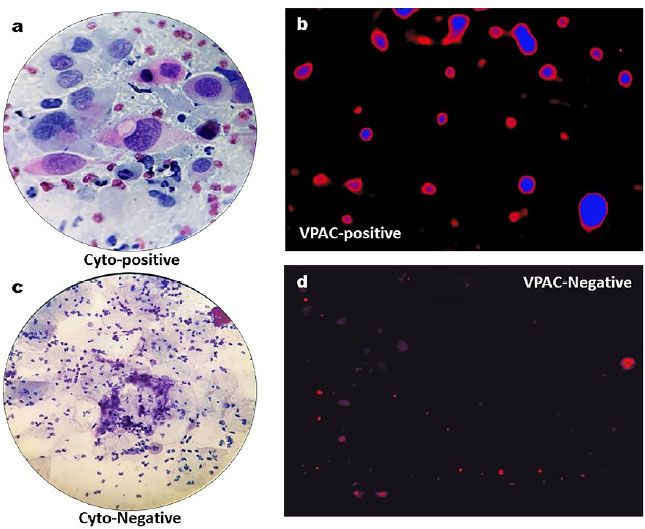
Similarly, another set of prepared smears were used for VPAC receptor detection. The slides were fixed in 97% ethyl alcohol. TP4303 solution (0.5μg) was added to the cells to cover the entire cell area, approximately one cm in diameter. The slide was then kept in dark, at 22°C for approximately 20 minutes and then thoroughly rinsed with deionized water and air dried. On the cells was then added, 20μL of 4,6 dimidino-2-phenylindole, dihydrochloride (DAPI, Fisher Scientific, PA) which strongly binds to A-T rich region of DNA in the cell nucleus. A coverslip was then placed and the slide was observed using a fluorescent microscope. Cells with TP4303 interaction presented themselves with dark orange fluorescence around the nucleus and thereby indicated the presence of VPAC receptor molecules around the cell surface. In the absence of VPAC receptors, only the DAPI bound cell nucleus was seen in dark blue. Normal epithelial cells that may only have minimal or no expression of VPAC therefore do not interact with TP4303 and show only cell nucleus.
Samples for biopsy of the cervix was sent for histopathological examination.
The data was collected and entered into Microsoft Excel-2019 and compared for descriptive statistics, frequency and percentage distribution. The variables were recorded and analysed for statistical significance using IBM SPSS statistics via software Inc., version 22.0.
During the study period September 2020 to November 2021, a total of 114 women attending the Gynaecology outpatient department of our hospital were included in the study. The symptoms of these patients were as shown in (
Figura 1A. Cervical cytology shows pleomorphic keratinized squamous carcinoma and tadpole cells (Pap stain); B. VPAC receptor positive for malignancy; C. Cervical cytology shows normal epithelial cells with inflammation (Pap stain); D. VPAC receptor negative for malignancy.
| No | Symptoms | Total (114) | Ca cervix (25) | Non-malignant (89) | p-value |
|---|---|---|---|---|---|
| 1 | Bleeding per vaginum | 42(36.8%) | 14 (56%) | 28(31.5%) | |
| 2 | Pelvic Pain | 30(26.3%) | 06 (24%) | 24(27%) | |
| 3 | Weight loss | 1 (0.9%) | 01 (4%) | 0 (0%) | 0.015 |
| 4 | Abdominal pain | 41 (36.0%) | 04 (16%) | 37(41.6%) | |
| Total | 114 (100%) | 25 (100%) | 89 (100%) |
| No | SPECULUM FINDINGS | Total (114) | Ca cervix (25) | Non-malignant (89) | p-value |
|---|---|---|---|---|---|
| 1 | White discharge | 23 (20.17%) | 8 (32%) | 15(16.85%) | |
| 2 | Bloody discharge | 37 (32.45%) | 11 (44%) | 26(29.21%) | |
| 3 | Foul smelling discharge | 5 (4.38%) | 2 (8%) | 3(3.37%) | 0.041 |
| 4 | Cervix inflamed | 22 (19.29%) | 2 (8%) | 20(28.09%) | |
| 5 | Ulcers over cervix | 27 (23.68%) | 2 (8%) | 25(28.09%) | |
| Total | 114 (100%) | 25 (100%) | 89 (100%) |
| No | Histopathology | Positive for carcinoma on Pap smear | VPAC receptor positivity |
|---|---|---|---|
| 1 | Positive for cervical cancer (25) | 20 (80%) | 23 (92%) |
| 2 | Negative for cancer (89) | 85 (95.5%) | 87 (97.8%) |
| No | Histopathology | PAP positive for cancer | VPAC receptor positivity |
|---|---|---|---|
| 1 | Positive predictive value | 83.33% | 92% |
| 2 | Negative predictive value | 94.44% | 97.75% |
| 3 | Accuracy | 92.11% | 96.49% |
Cancer of the uterine cervix is the second most common cancer among women world- wide. In India this is the commonest cancer among women and this country has the largest burden of cervical cancer patients in the world. One out of every five women in the world suffering from this disease belongs to India. More than three-fourths of these patients are diagnosed at advanced stages leading to poor prospects of long-term survival and cure.
Better understanding of human diseases at the cellular and molecular levels has paved the way for development of several novel life-sciences technologies. Identification of circulating tumour cells (CTC) in human blood and/or body fluids is one. Currently the CTC-associated liquid biopsy approach has drawn considerable attention and is rapidly getting incorporated into clinical applications.
It has been hypothesized that malignant cells shed in body fluids could be imaged optically, by targeting the VPAC1 receptors with the same peptide labelled with a fluorophore. Trabulsi et al. (2017)
This study shows that VPAC receptor positivity for cancer of cervix is good alternative to PAP staining. The study is highly sensitive with very low false negativity and false positivity rate. The diagnosis is highly reliable similar to Pap staining and can be utilized in an OPD setting. Our study is a preliminary study with a small study population. Our study needs to be validated by multicentric and randomized trials.
RBN Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing.
KV Collection and assembly of data, Final approval of manuscript, Provision of study materials or patient.
MK Collection and assembly of data, Final approval of manuscript, Provision of study materials or patient.
SR Final approval of manuscript, Provision of study materials or patient.
SCG Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient.
MLT Conception and design, Data analysis and interpretation, Final approval of manuscript, Provision of study materials or patient.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Ferlay, J and Soerjomataram, I and Ervik, M and Dikshit, R and Eser, S. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012 v1. International Agency for Research on Cancer, 2013.
2. Institute for Health Metrics and Evaluation (IHME). The challenge ahead: progress in breast and cervical cancer [Internet]. IHME, 2011.
3. Morrison, AS. Screening in chronic disease. Oxford University Press, 1992.
4. Welch, HG and Black, WC. Evaluating randomized trials of screening. J Gen Intern Med [online]. 1997, vol. 12, p. 118-24.
5. Bobdey, S and Sathwara, J and Jain, A and Balasubramaniam, G. Burden of cervical cancer and role of screening in India. Indian J Med Paediatr Oncol [online]. 2016, vol. 37, p. 278-85.
6. Saslow, D and Solomon, D and Lawson, HW and Killackey, M and Kulasingam, SL and Cain, J. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. Am J Clin Pathol [online]. 2012, vol. 137, p. 516-42.
7. Andrae, B and Kemetli, L and Sparen, P and Silfverdal, L and Strander, B and Ryd, W. Screening-preventable cervical cancer risks: evidence from a nationwide audit in Sweden. J Natl Cancer Inst [online]. 2008, vol. 100, p. 622-9.
8. Andrae, B and Andersson, ML and Lambert, PC and Kemetli, L and Silfverdal, L and Strander, B. Screening and cervical cancer cure: Population based cohort study. Br Med J [online]. 2012, vol. 344, p. e900.
9. Guidelines for Cervical Cancer Screening Programme (GCCS). Government of India-World Health Organization Collaborative Programme (2004-2005), 2006.
10. Cristofanilli, M and Hayes, DF and Budd, GT and Ellis, MJ and Stopeck, A and Reuben, JM. Circulating tumor cells: a novel prognostic factor for newly diagnosed metastatic breast cancer. J Clin Oncol [online]. 2005, vol. 23, p. 1420-30.
11. Thakur, ML and Zhang, K and Berger, A and Cavanaugh, B and Kim, S and Channappa, C. VPAC1 receptors for imaging breast cancer: a feasibility study. J Nucl Med [online]. 2013, vol. 54, p. 1019-25.
12. Tripathi, SK and Trabulsi, EJ and Gomella, L and Kim, S and McCue, P and Intenzo, C and Birbe, R. [object Object]. Urology [online]. 2016, vol. 31, p. 29-36.
13. Thakur, ML and Aruva, M and Gariepy, J and Acton, P and Rattan, S and Prasad, S. PETimagingoncogeneoverexpression using 64Cu- VIP analog: comparison with 99mTc-VIP analog. J Nucl Med [online]. 2004, vol. 45, p. 1381-9.
14. Thakur, ML and Devadhas, D and Zhang, K and Pestell, RG and Wang, C and McCue, P. Imaging spontaneous MMTVneu transgenic murine mammary tumors: targeting metabolic activity versus genetic products. J Nucl Med [online]. 2010, vol. 51, p. 106-11.
15. Trabulsi, EJ and Tripathi, SK and Gomella, L and Solomides, C and Wickstrom, E and Thakur, ML. Development of a voided urine assay for detecting prostate cancer non-invasively: a pilot study. BJU Int [online]. 2017, vol. 119, p. 885-95.
16. Nerli, RB and Ghagane, SC and Bidi, SR and Thakur, ML and Gomella, L. Voided urine test to diagnose prostate cancer: preliminary report. Cyto Journal [online]. 2021, vol. 18, p. 26.
17. Reubi, JC and Laderach, U and Waser, B and Gebbers, JO and Robberecht, P and Laissue, JA. Vasoactive intestinal peptide/pituitary adenylate cyclase-activating peptide receptor subtypes in human tumors and their tissues of origin. Cancer Res [online]. 2000, vol. 60, p. 3105-12.
18. The biological significance of PACAP and PACAP receptors in human tumors from cell lines to cancer. Springer-Verlag, 2003.
19. Zia, H and Hida, T and Jakowlew, S and Birrer, M and Gozes, Y and Reubi, JC. Breast cancer growth is inhibited by vasoactive intestinal peptide, (VIP) hybrid, a synthetic VIP receptor antagonist. Cancer Res [online]. 1996, vol. 56, p. 3486-9.
20. Leyton, J and Gozes, Y and Pisegna, J and Coy, D and Purdom, S and Caibang, M and Zia, F. PACAP (6-38) is a PACAP receptor antagonist for breast cancer cells. Breast Cancer Res Treat [online]. 1999, vol. 56, p. 177-86.
Dados de acesso insuficientes para visualização no mapa.