The inferior vena cava sarcoma (IVC) represents 2% of all leiomyosarcomas. It is a tumor of mesenchymal origin of poor prognosis, because approximately 50% of patients submitted to curative surgical resection will present recurrence of the disease. Leiomyosarcoma represents 60% of IVC primary malignancy cases of the inferior vena cava, and until the year 2010 there were less than 300 cases reported in medical literature on this pathology. The diagnosis is more common in sexagenarian women and the segment of the inferior vena cava most affected is located between the hepatic veins and the renal veins.[
Surgical R0 resection in monoblock is the only form of curative treatment. The objectives of surgery are complete resection of malignant neoplasia, prevention of locoregional recurrence and venous return preservation. Due to the proximity to abdominal and retroperitoneal structures, enlarged resections may be necessary to obtain free margins. Surgical reconstruction of the vena cava is a controversial subject in the medical literature. Adjuvant treatment with radiotherapy is not related to increased survival in patients with leiomyosarcoma of the inferior vena cava; however, radiotherapy may assist in local disease control.[
We report the case of a 73-year-old female patient with IVC leiomyosarcoma who underwent surgical R0 resection by videolaparoscopy. Reconstruction of the vena cava was not performed due to her low blood flow in the preoperative period and to the good development of collateral vascular systems. No neoadjuvant or adjuvant treatment has been performed.
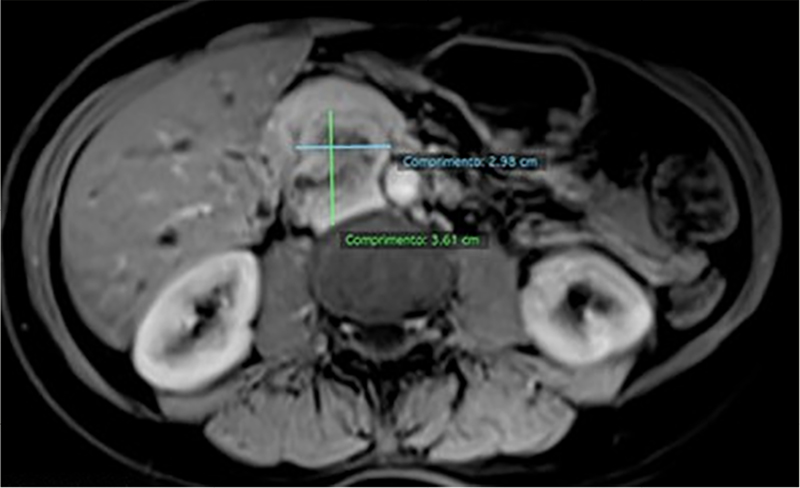
R.M.B, 73-years-old, female, presenting abdominal discomfort, started in August 2015, with chronic and progressive evolution without irradiation and without other associated symptoms. The patient underwent these propaedeutic exams in March of 2016. Magnetic resonance image (MRI) upper abdomen floor showing expansive lesion with lush and heterogeneous enhancement after intravenous contrast located up retroperitoneal previously shifting the head of the pancreas and caudal duodenal arc, and keeping in touch with the right wall of the aorta, without definite signs of invasion of these structures and without a cleavage plane with the inferior vena cava, and may represent its primary lesion (
Figure 1 Para-aortic retroperitoneal lesion in the inferior vena cava topography with heterogeneous impregnation by contrast and restricted diffusibility.
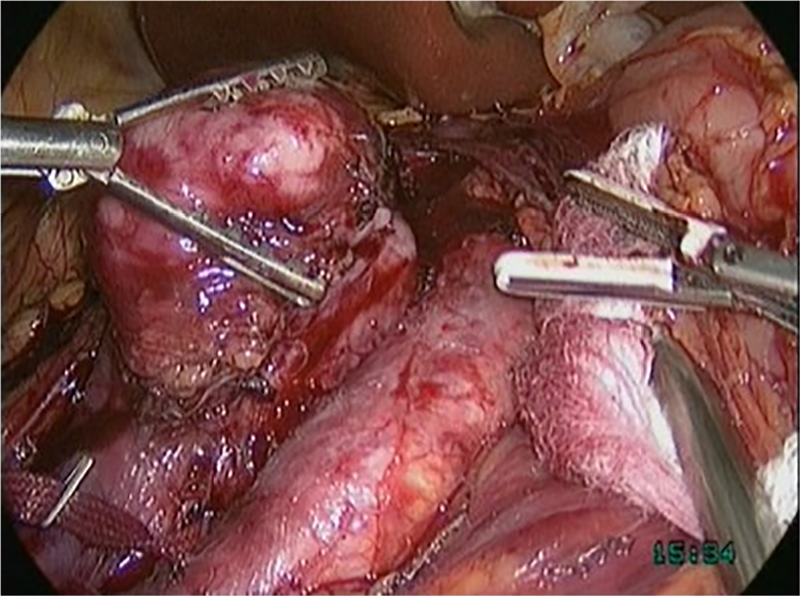
Patient submitted to videolaparoscopic surgery in April 2016 for leiomyosarcoma treatment of the inferior vena cava located below renal veins and above the iliac vein bifurcation (segment I). Six trocars were arranged as follows: umbilical of 10mm, in the right flank of 12mm, in the left iliac fossa of 12mm, in the left flank of 5mm, in the right iliac fossa of 5mm and in epigastric region 5mm port. Dissection (
Figure 2 Dissection: distal and posterior repair of the inferior vena cava.
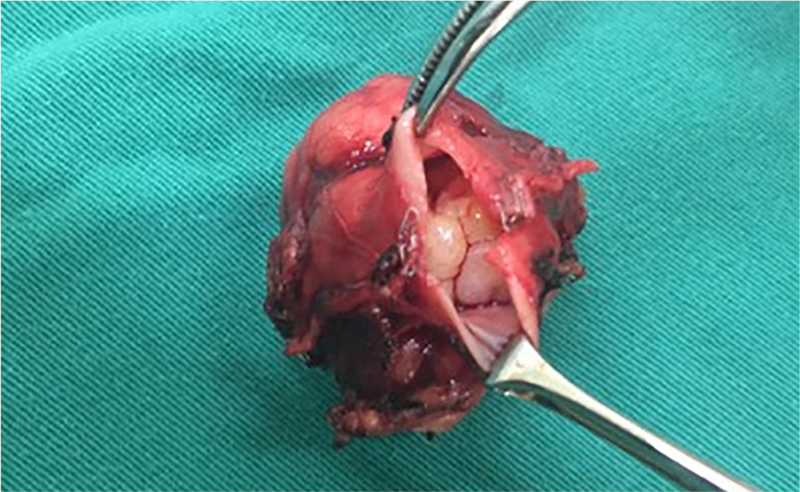
Figure 3 Intraluminal tumour and negative margin.
The surgery time was approximately 2h40min, and there was no intraoperative complication. An oral diet was introduced on the first postoperative day and the patient was discharged on the third postoperative day. Prophylactic heparinization was performed with enoxiparin 1mg/kg once daily for 30 days postoperatively.
Histological and immunohistochemical profile positive for desmin and smooth muscle actin. The diagnosis consistent with grade 1 leiomyosarcoma of 4 centimeters arising from the IVC with endophytic extension. Macro and microscopic negative margins.
After 30 months of follow up, the patient is asymptomatic, with no lower extremity lymphedema or thrombosis and no locoregional disease. She presented liver and lung metastasis, and is currently receiving combined chemotherapy with doxorubicin and olaratumab.
Primary leiomyosarcoma of inferior vena cava is a rare neoplasm and of poor prognosis, which develops from the smooth muscle constituents of the media layer of the blood vessel. It is the most common tumor of the venous system where the inferior vena cava and the most affected vessel. IVC leiomyosarcoma presents classification defined by its location: segment I (lower), below the renal vessels (IVC infrarenal); Segment II (middle): between the origin of renal vessels and the hepatic vein; Segment III (superior): between the origin of the hepatic veins to the right atrium (IVC suprahepatic). The majority of tumors are located in the middle segment (50.8%) and lower segment (44.2%). In our study, the patient presented IVC leiomyosarcoma in segment I.[
In patients with metastasis and in those cases where it will not be possible to perform R0 resection, it must performed neoadjuvant treatment and evaluate the possibility of R0 resection later. For patients submitted to surgical resection the next step is to analyze the margins of the surgical part. In case of free margins, the patient will be monitored and in case of positive margins, should be performed adjuvant treatment.[
Chemotherapy and radiotherapy are not associated with increased patient survival; however, radiotherapy seems to help in local disease control. Reconstruction of the vena cava after resection of the tumor is a very controversial subject since some authors believe that this procedure would increase intraoperative time by increasing the morbidity of the procedure. In addition they believe that the patient is able to tolerate well the ligature of the inferior vena cava.[
After a careful literary survey on this subject (BIREME, Portal CAPES, PubMed and RIMA), we did not find studies that report videolaparoscopy as an access way in surgical resection of this type of tumor. All reports mention the laparotomy.
Just only one paper report a laparoscopic excision of an exophytic tumour without any intraluminal extension and no compromising IVC lumen.[
In our report, the patient underwent total laparoscopic monoblock resection of the inferior vena cava and leiomyosarcoma with free margins, and the surgical time was similar to that of the laparotomy procedure described by other authors. The patient was given oral diet on the first postoperative day and hospital discharge on the third postoperative day, that is, there was a significant reduction in the length of hospital stay, contributing to a reduction in morbidity.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.