Treatment of advanced melanoma has undergone a revolution over the last decade. Immunotherapy with high-dose interleukin-2 (IL-2)(
Considering that the treatment of any patient at a public oncology treatment center is reimbursed by the Ministry of Health (MH) according to the socalled Authorization of Ambulatory Care Procedure (Autorização de Procedimento Ambulatorial - APAC), which is a document where the diagnosis and the proposed treatment regimen are recorded, it is expected that the vast majority of patients with advanced melanoma treated at one of such facilities would receive a treatment which has its financial cost covered based on the APAC.
Each APAC (which is valid for up to three months and forwarded by the oncology treatment center to the MH) has a prespecified corresponding monetary value, dependent on the diagnosis and the line of treatment (first line, second line, etc.), and this value is transferred to the treatment center periodically. Although there are a few exceptions where the MH buys and then distributes the medication (such as is the case with imatinib for chronic myelogenous leukemia or trastuzumab for breast cancer), this does not apply to any melanoma treatments. Therefore, we assumed that evaluating all the APACs related to the diagnosis of advanced melanoma for which the MH reimbursed the oncology treatment centers for, would give an accurate picture of how melanoma is treated at SUS.
To undertake an exploratory analysis of the patients with advanced melanoma and the treatment they received at SUS between the years 2015 and 2017.
We evaluated the data available at DATASUS,(
Different treatments were initially grouped based on the name of the protocol or the names of the medications that were recorded in the APACs. These were then reviewed in order to be correctly assigned to treatment groups related to different levels of effcacy, as described below. We excluded those APACs that recorded ICD C43 but were related to supportive medications (such as bisphosphonates for bone metastasis or pain medications). We then classified all drugs or drug combinations as being inadequate, minimally effective, moderately effective or effective treatments (
| Drug | Drug combinations | |
|---|---|---|
| Effective | Vemurafenib Ipilimumab Pembrolizumab Nivolumab High dose Interleukin | |
| Moderately effective | Platinum + Taxane + DTIC Platinum + vinca alkaloid Platinum + vinca alkaloid + DTIC Platinum + vinca alkaloid + BCNU Platinum + BCNU or CCNU DTIC + vinca alkaloid Platinum + Taxane + IFN Platinum + Vinblastine + DTIC + IFN | |
| Minimally effective | Interferon Dacarbazin (DTIC) Cis or Carboplatin Carmustin (BCNU) Lomustin (CCNU) Temozolomide Tamoxifen Vincristin Taxol or Docetaxel | |
| Inadequate | Etoposide Ifosfamide Gemcitabin 5FU Metotrexate Irinotecan Doxorubicin Cyclophosphamide | Any combination with inadequate drugs |
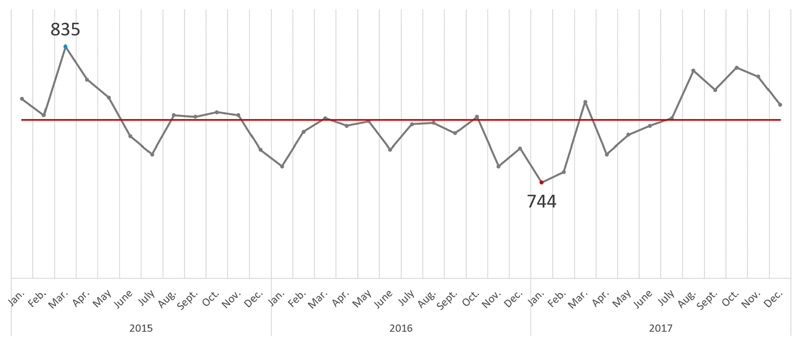
We initially identified 13,187 APACs related to the treatment of melanoma. Of these, we excluded 2,344, which were related to either some systemic treatment for stage III melanoma or supportive medications. We ended up analyzing 10,843 APACs, related to the treatment of metastatic melanoma of 4,338 patients treated between January 2015 and December 2017. The monthly number of patients on treatment varied from 744 to 835 and was relatively stable over these two years (
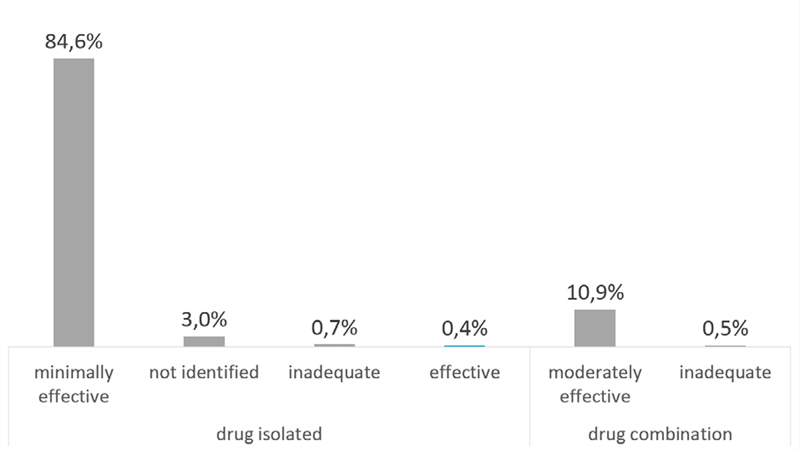
We identified 19 different treatment protocols used as first line, of which 11 consisted of single drug and 8 of drug combinations. Over the two-year period (and excluding those who were already on some treatment in January 2015), 3,097 (88%) and 281 (8%) patients initiated treatment with a minimally effective or moderately effective regimen, respectively (
Figure 1 Patients on treatment.
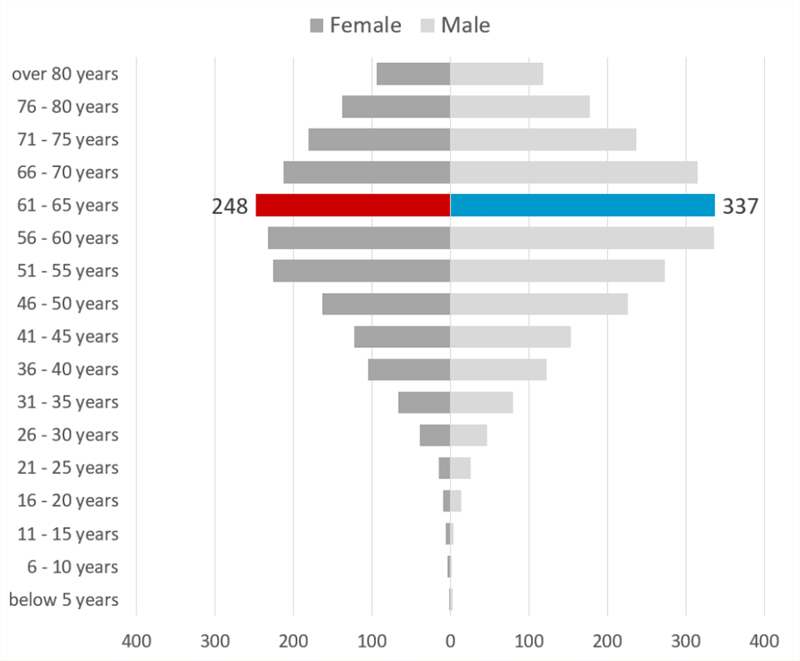
Figure 2 Age distribution.
Figure 3 Distribution of treatments by type and effcacy.
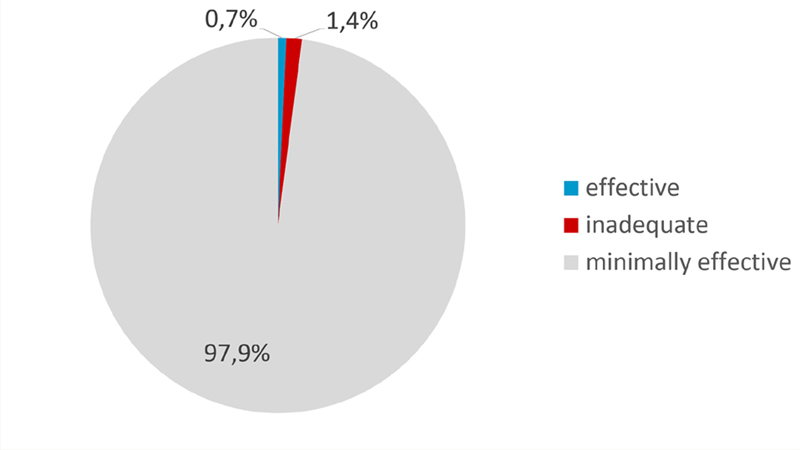
Figure 4 Treatment by efficacy.
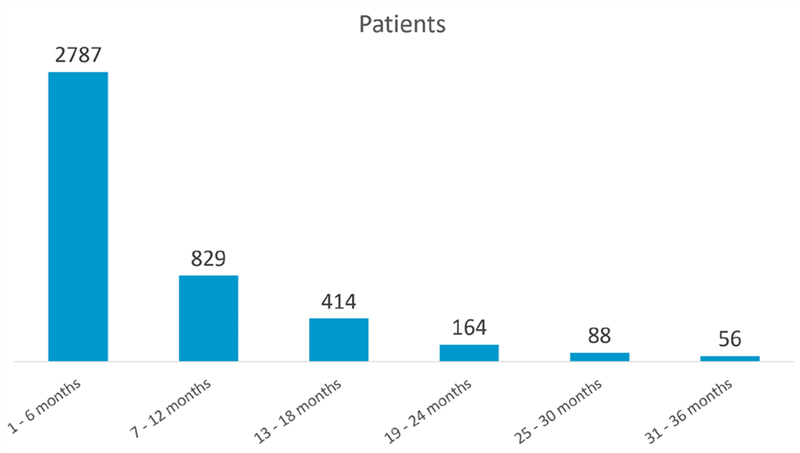
Figure 5 Duration of treatment.
Our investigation allows us to evaluate the different types of treatments prescribed to patients at public oncology treatment centers and reimbursed by the MH in Brazil. It clearly documents a fairly short duration of treatment of less than six months, which is in line with historical duration of ineffective therapies for metastatic melanoma such as dacarbazine. We found a significant difference in length of treatment duration between different states in the country, which will have to be better investigated. Since more than 98% of treatments consist of minimally effective or at best moderately effective therapies, it comes as no surprise that the mean duration of treatment is so short.
We draw attention to the 19 possible first assigned treatment regimens, indicating a lack of standard. Indeed, the Ministry of Health does not impose any guidelines for cancer treatment. Instead, one of its divisions, the so-called Secretaria de Assistência à Saúde - SAS) publishes periodically Directives for Diagnosis and Treatment (Diretrizes de Diagnóstico e Tratamento - DDTs), with a review of the disease and suggestions as to which are recommended treatment options. The last DDT for melanoma was published in 2013 (one year after vemurafenib and the same year ipilimumab were registered in Brazil) and recommended essentially treatment with dacarbazine,(
One criticism to our data consists of the fact that patients may have received other treatments than those recorded in the APACs and submitted to the MH for reimbursement, and therefore would not be identified in our analysis. This would be possible if the specific treatment center had a different source of financing such as the state department of health, philanthropic financing or if the patient filed and won a lawsuit in order to receive modern therapy. Although we acknowledge this possibility, we believe it would only be pertinent to a small minority of patients being treated at SUS, where most treatment centers only administer treatments that are reimbursed by the MH. Regarding the length of 5 months on therapy, this is in line with what used to be reported when dacarbazine or dacarbazine combinations were used.(
Medical oncologists prescribing treatment for advanced melanoma face an ethical dilemma by being forced to prescribe minimally effective therapies in order to preserve financial viability of the treatment center, while the MH dodges responsibility by publishing DDTs that are rarely updated and not a mandatory guideline to begin with. Advanced melanoma constitutes the prime example of cancer where the massive advance in knowledge and new and effective treatment options have widened the gap of life expectancy between those patients treated in the Private Health System versus at the Public Health System.
Currently, based on the monthly reimbursement of the APAC related to systemic therapy for melanoma, the MH spends R$1,080 (approximately U$270) for every month/patient. The average of U$1,600/ patient spent by the MH (as described before) over the course of the whole systemic treatment certainly would not suffice to offer modern treatments. As an example, if a 70kg patient were to be treated in the Public Health System with current pricing of nivolumab (the MH has a mandatory 20% discount off the market price, before any negotiations), it would cost R$28,300/month (approximately U$7,250). If ipilimumab were to be used for four cycles, each cycle would cost R$70,900 (U$18,200). Other checkpoint inhibitors approved for the treatment of advanced melanoma would cost about the same magnitude.
There are precedents in the Brazilian Public Health System where very high discounts have been negotiated in order to offer modern hepatitis C treatment and trastuzumab to patients with HER2positive breast cancer, and most certainly, a model of risk sharing should be negotiated with the pharma industry. The same way physicians have a moral obligation to offer the best possible treatment, pharma industry should undertake a significant effort in order to make life changing medications available worldwide. There is an urgent need for new models of payment based on performance, rather than the traditional price/volume model of negotiation. At a time when the most effective systemic therapies consist of dual checkpoint inhibitors or combined BRAF-MEK inhibition at an enormous cost, we believe a good start would be to offer single-agent checkpoint inhibitor (anti-PD1/ PDL1 inhibitor) or alternatively a BRAF protein kinase inhibitor to those with V/K600E mutation, on a risk sharing model as a pilot for oncology treatments.
Based on the analysis of 4,338 patients with advanced melanoma treated between 2015 and 2017 in the Brazilian Public Health System, we estimate that more than 98% of treatments were minimally effective, and not surprisingly, patients were treated for less than six months overall. The median duration of treatment was expectedly short, and the variety of first line therapies used in one same health system was concerningly high. These are the result of an outdated reimbursement model and the lack of mandatory treatment standard.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.