Primary spleen tumors have a low-incidence pathology. They present nonspecific manifestations that can make diagnosis difficult, and are normally only found after surgical removal of the organ and subsequent anatomopathological study.
The purpose of this case report is to address the clinical features, diagnosis, treatment, and literature review of a pediatric patient who was diagnosed with littoral cell splenic angioma and investigated at a university pediatric service in southern Brazil. This case report was approved by the ethics committee (approval number 67482223900000120) in 2023.
Ten years old white female patient with diffuse, sporadic, low-intensity abdominal pain for two years was treated at a pediatric outpatient clinic. Three months prior, pain in the left hypochondrium developed, with occasional irradiation of the right hypochondrium. The use of dipyrone had no effect, and the pain interfered with her daily activities associated with inappetence and loss of three kilograms (6.61lb) in one month, however normal bowel movements were reported. She presented with no fever, vomiting, nausea, or pathological background.
On physical examination, only pale skin and a painful abdomen were observed, as deep palpation was performed on the left hypochondrium.
Laboratory tests, total abdominal ultrasound, and abdominal and pelvic computed tomography were performed. Laboratory tests showed no significant changes (erythrocyte sedimentation speed; glycemia; hepatic, renal, pancreatic, and thyroid function tests; ferritin; lipidogram; total immunoglobulin A, M, G, and protein electrophoresis), a hemoglobin of11,6g/% and a hematocrit of 35,4% below expected levels. Total abdominal ultrasound showed a spleen of the usual size, with a nodular hypoechogenic image inside, with well-defined and regular contours, measuring approximately 4.41x3.90x4.41 centimeters (cm), volume 39,65cm3 (
Figura 1 Abdominal ultrasound imaging of splenic littoral cell angioma, measuring approximately 4.41x3.90x4.41cm.
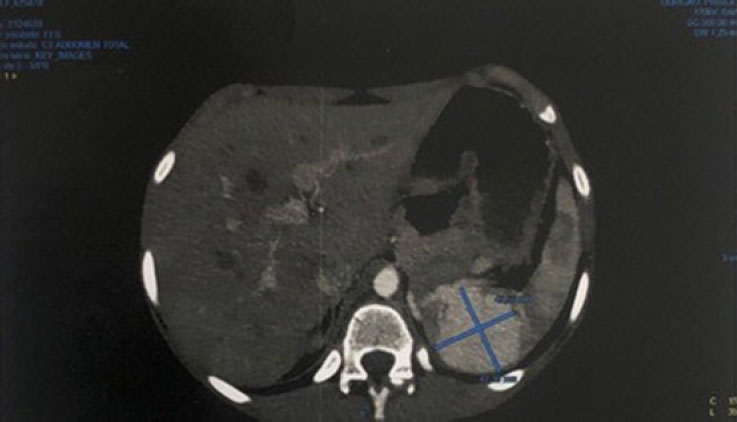
Figura 2 Abdominal computed tomographic imaging of splenic littoral cell angioma measuring 4.5x4.7cm.
The surgery was performed without complications. Starting with a left subcostal incision in the layers, a small spleen with a voluminous hilar circulation was observed. Spleen dislocation and detachment along the splenorenal and splenocolic ligaments were performed, in addition to dissection, identification, and ligation of the splenic artery, splenic vein, and short vessels. The surgical specimen was extracted, followed by a review of hemostasis and closure by layers. The spleen, weighing 90 grams and measuring 10,0x5,0 centimeters with the presence of a well- defined and firm light brown lesion measuring 3,5x3,5x3,0 centimeters, was referred to histopathological study and immunohistochemical examination, which showed, in the histological sections, a spleen containing proliferation of monotonous anastomosing vascular channels that resembled splenic sinuses, lined by high endothelial cells. The channels had irregular lumens and solid areas (
Figure 3A, 3B and 3C A. Findings in the histological section of the sample using hematoxylin eosin. Histological sections of the spleen lesion show proliferation of monotonous anastomosing vascular channel lined by tall endothelial cells; B. Immunohistochemical findings. Positive CD68 observed; C. Immunohistochemical findings. Positive CD31 observed.
Littoral cell angioma is a vascular tumor of unknown etiology that arises from cells that line the venous sinuses of the splenic red pulp.
It is asymptomatic in 55% of cases; however, when symptomatic, it can cause diffuse abdominal pain and fever, splenomegaly, anemia, thrombocytopenia,
The differential diagnoses included hemangioma, hamartoma, lymphoma, and angiosarcoma. Benign tumors of the spleen include hemangiomas and hamartomas. The most common hemangiomas are of vascular origin, and ultrasound imaging reveals homogeneous hypoechoic or hyperechoic lesions. A rare lesion is a hamartoma, and sonography reveals homogeneous lesions withor without a cystic center. The most prevalent malignant neoplasm is lymphoma, and angiosarcoma of vascular origin is rare and is more susceptible to metastasis and rupture.
Histologically, littoral cells are normally found around sinusoids of the red pulp of the spleen. When these cells increase in size, they can become precursors of tumor.
In the case reported by Bedir et al. (2014),
Total splenectomy is the best treatment option due to the possibility of malignant lesions. This approach was used in the case described here. Both open and laparoscopic surgeries are options to be considered, although the laparoscopic approach has a shorter operating time and less blood loss during the procedure. Of the 12 patients reported in the pediatric age group, all were investigated with ultrasound, nine underwent total splenectomy, two underwent partial splenectomy, and one underwent biopsy and active follow-up.
In addition, it is important that the patient be monitored during the postoperative period to evaluate recurrence or metastasis.
In this case report of littoral cell angioma, the only symptom the patient presented with was abdominal pain, and the treatment was surgery. Awareness of this rare diagnostic possibility is important because of the possibility of malignant evolution. It is usually an incidental finding owing to its mostly asymptomatic or nonspecific presentation. Littoral cell angioma is a rare condition in the pediatric age group, the cause of which is still unknown, and its pathogenesis is uncertain.
Therefore, the few cases reported in the literature should be followed for a better understanding of the pathophysiology ofthe disease. In addition, further studies are needed to investigate the prevalence of littoral cell angioma of the spleen in pediatric patients, corroborating early diagnosis and appropriate management to avoid possible progression to malignancy.
SMW Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
AFP Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
NHL Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
RR Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
JB Collection and assembly of data, Conception and design, Final approval of manuscript, Provision of study materials or patient
CR Collection and assembly of data, Final approval of manuscript, Provision of study materials or patient
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Roseira, LFT and Loiola, FC and Guedes, VR. Neoplasias primárias do baço. Rev Patol Tocantins [online]. 2017, vol. 4, p. 21-4.
2. Roldan-Vasquez, E and Roldan-Vasquez, A and Jarrin-Estupiñan, X and Roldan-Crespo, J. Case report: Infrequent littoral cell angioma of the spleen. Int J Surg Case Rep [online]. 2021, vol. 85, p. 106242. https://doi.org/10.1016/j.ijscr.2021.106242 Ver referência
3. Rai, M and Gupta, N. Littoral cell splenic angioma [Internet]. StatPearls, 2021.
4. Liagat, N and Madani, AA and Kausar, N and Almaimani, MOA and Mahomed, A. Littoral cell angioma of the spleen in a child with Cornelia De Lange syndrome. J Pediatr Surg Case Rep [online]. 2021, vol. 69, p. 101868. https://doi.org/10.1016/j.epsc.2021.101868 Ver referência
5. Zeng, QY and Liao, J and Song, Y and Zhang, DQ and Li, H and Wang, J. Multimodality imaging findings of splenic littoral cell angioma: a case description and analysis of literature. Quant Imaging Med Surg [online]. 2023, vol. 13, p. 2740-3. https://doi.org/10.21037/qims-22-897 Ver referência
6. Arcuri, PP and Taglianetti, ST and Vavalà, B and Battaglia, C and Laganà, D and Manti, D. Incidental littoral cell angioma of the spleen: cross-sectional imaging findings and review of the literature. Radiol Case Reports [online]. 2022, vol. 17, p. 3545-50. https://doi.org/10.1016/J.RADCR.2022.06.063 Ver referência
7. Matuszczak, E and Reszec, J and Debek, W and Hermanowicz, A and Chyczewski, L. Is littoral cell angioma of the spleen as rare as previously believed in the pediatric population?. Folia Histochem Cytobiol [online]. 2012, vol. 50, p. 480-5. https://doi.org/10.5603/19761 Ver referência
8. Bedir, R and Sehitoglu, I and Calapoglu, AS and Yurdakul, C. A rare case of splenic littoral cell angioma in a child. J Lab Physicians [online]. 2014, vol. 6, p. 117-20. https://doi.org/10.4103/0974-2727.141511 Ver referência
9. Bouzayan, L and Rachid, J and Mabrouk, MY and Ayoub, M and Abdlali, G and Haloui, A. Littoral cell angioma of spleen: a rare case report. Ann Med Surg [online]. 2022, vol. 79, p. 103904. https://doi.org/10.1016/J.AMSU.2022.103904 Ver referência
10. Pillay, Y and Shokeir, MO. Case report of a littoral cell angioma of the spleen and accessory spleens: a benign vascular tumour. Int J Surg Case Reports [online]. 2017, vol. 40, p. 109-12. https://doi.org/10.1016/j.ijscr.2017.09.017 Ver referência
11. Cai, YQ and Wang, X and Ran, X and Liu, XB and Peng, B. Laparoscopic splenectomy for splenic littoral cell angioma. World J Gastroenterol [online]. 2015, vol. 21, p. 6660-4. https://doi.org/10.3748/WJG.V21.I21.6660 Ver referência
12. Bisceglia, M and Sickel, JZ and Giangaspero, F and Gomes, V and Amini, M and Michal, M. Littoral cell angioma of the spleen: an additional report of four cases with emphasis on the association with visceral organ cancers. Tumor J [online]. 1998, vol. 84, p. 595-9. https://doi.org/10.1177/030089169808400516 Ver referência
13. Moreira, C. Esplenectomias não traumáticas em adultos e crianças: um estudo comparativo [dissertation] [Internet]. Universidade Federal de Santa Catarina (UFSC), 2002.
14. Marques, RG and Petroianu, A. Infecção fulminante pós-esplenectomia. Arq Gastroenterol [online]. 2003, vol. 40, p. 1-8. https://doi.org/10.1590/S0004-28032003000100011 Ver referência


Dados de acesso insuficientes para visualização no mapa.