After GOG 209, the first line treatment of metastatic endometrial cancer is based on carboplatin plus paclitaxel chemotherapy. As of second line, monotherapy such as doxorubicin or gemcitabine demonstrates low response rates, progression-free survival, and overall survival.(1,2) Recently, this scenario has changed positively following the results of immunotherapy in second-line treatment. After failure to platinum, KEYNOTE-775 study confirmed pembrolizumab plus lenvatinib as the standard of care for patients with microsatellite stable tumors.
Since the 2014 World Health Organization (WHO) classification, carcinosarcomas have been reclassified as uterine carcinomas (previously they were classified as uterine sarcomas). This change considers that carcinosarcomas are metaplastic carcinomas with the presence of sarcomatous metaplasia in their embryonic epithelial origin.
The frequency of MSI-H or dMMR is uncertain in carcinosarcomas, as well as the benefit of immunotherapy for these patients. A recent Korean series published by Noh et al. (2022)
A 60-year-old woman with a history of regular gynecological follow-ups initiated with vaginal bleeding in December 2019. A transvaginal ultrasound was performed in January 2020 and showed an endometrial thickening of 15.5 millimeters. Hysteroscopy was indicated, but due to the COVID-19 pandemic, the patient postponed the exam to October 2020.
The patient underwent hysteroscopy in October 2020, which showed a fragmented fibrous structure exteriorizing in the external cervical orifice. The histopathology demonstrated an endometrial neoplasm composed of well-differentiated endometrioid adenocarcinoma associated with atypical spindle cells with frequent mitotic figures. Immunohistochemistry panel confirmed carcinosarcoma (desmin, EMA
The patient was submitted to surgery with hysterectomy, bilateral salpingo-oophorectomy and pelvic lymphadenectomy in November 2020. The final report confirmed a 4.8×2.4cm lesion affecting from the uterine fundus to the cervical isthmus and infiltrating the entire thickness of the myometrium, presence of lymphovascular invasion, and 3 out of 7 left pelvic lymph nodes and 3 out of 3 right pelvic lymph nodes compromised (clinical stage IIIC1 - pT1bpN1M0). She received six cycles of adjuvant chemotherapy (carboplatin AUC 6 plus paclitaxel 175mg/m2 every three weeks) between December 2020 to March 2021. Subsequently, she received adjuvant external beam radiotherapy (4,500cGy at 180cGy/fraction in 25 fractions between March 2021 to May 2021) and brachytherapy (3 insertions of 800cGy in July 2021).
In May 2022 she developed right iliac fossa pain. The abdominal MRI showed an irregular heterogeneous mass of 3.6×2.7cm in the right pelvic region between psoas muscle and vertebral body of L4 and an enlarged lymph node in the left periaortocaval chain measuring 2.4×1.4cm. The pelvic lesion was in contact with iliac vessels and right ureter leading to moderate ipsilateral hydronephrosis. A double-J stent was inserted, and a somatic and germline genetic panel was performed. The somatic panel was inconclusive due to the quality of the tumor sample. The germline panel had no mutations with clinical significance. The immunohistochemistry for the microsatellite proteins showed loss of MLH1 and PMS2 nuclear staining.
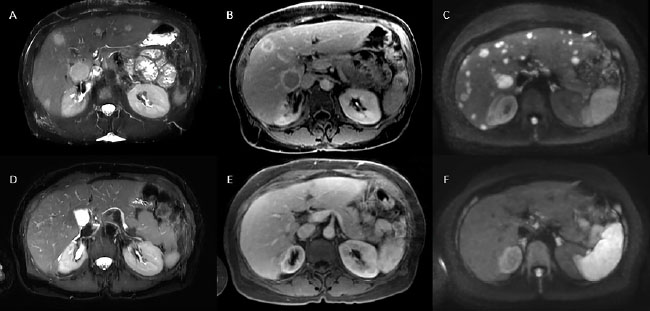
The patient persisted with severe pain in the lower abdomen, needing painkillers on an ongoing basis (morphine 15mg every 4 hours; dipyrone 1,000mg every 6 hours; pregabalin 75mg every 12 hours). New imaging was performed before starting the systemic treatment (May 2022). Chest computed tomography scan (CT) showed no evidence of disease, but abdominal MRI revealed multiple liver lesions (at least 25), the two largest in segments V and VI measuring 2.5cm and 3.0cm respectively; heterogeneous expansive formation located in the right pelvic region measuring 3.8×3.6cm; para-aortic and infrarenal lymphadenopathy measuring 2.7×1.8cm. The patient was started on pembrolizumab 200mg intravenously every 3 weeks as monotherapy. After the third cycle in mid-September 2022, the patient experienced complete pain resolution and discontinued ongoing analgesics (morphine and pregabalin; she continued to use dipyrone if there was mild pain). A new abdominal MRI was performed in October 2022 showing complete disappearance of the multiple hepatic nodular lesions, and partial response in the heterogeneous mass located in the right pelvic region measuring 3.4×2.7cm (prior: 3.8×3.6cm); complete regression was also observed in para-aortic and infrarenal lymphadenopathy (prior: 2.7×1.8cm) (
Figure 1 Liver metastases response at MRI exam. Axial plane images showing multiples liver metastasis in both hepatic lobes (upper images) at T2 fat-sat (A and D), portal-phase post-contrast T1 fat-sat (B and E) and diffusion-weighted images (C and F) with complete response after immunotherapy (bottom images).
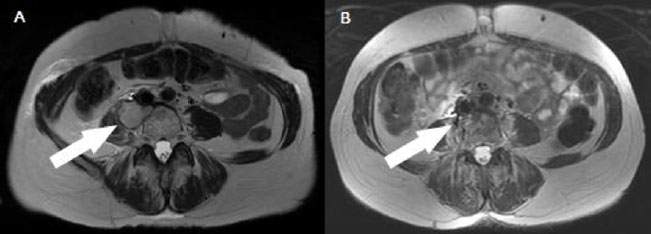
No grade 3 or 4 toxicities were experienced during treatment. She remained asymptomatic and new imaging tests were performed in March 2023, maintaining complete disappearance of the liver lesions and a decrease in the right pelvic mass - partial response by RECIST version 1.1 (
Figure 2 Axial image of MRI exam of October 2022 showing right pelvic mass (narrow A); exam of March 2023 with partial response of the lesion (narrow B).
Uterine carcinosarcoma is a rare tumor accounting for approximately 5% of all uterine carcinomas. It is a biphasic tumor where the sarcomatous component develops from a de-differentiation of the epithelial element.
We describe a woman with carcinosarcoma stage IIIC1 treated with surgery followed by chemotherapy and radiotherapy who had an abdominal recurrence approximately 12 months after the end of the treatment. Following current scientific evidence, this patient should receive first-line palliative chemotherapy with a median overall survival of 10 months.
The Cancer Genome Atlas (TCGA) of uterine carcinosarcoma published in 2017 evaluated genomic, epigenomic, transcriptomic, and proteomic characteristics of this tumor. In addition to classic mutations seen in other uterine carcinomas histologies (TP53, PTEN, PIK3CA, and KRAS), a higher prevalence of the EMT (epithelial-to-mesenchymal transition gene) mutation has been demonstrated. Of the 57 samples evaluated, in only two there was silencing of mismatch repair gene MLH1.
Although carcinosarcomas have not been included in immunotherapy studies for the treatment of metastatic uterine carcinomas, some case reports/case series have been published.
There is a phase 2 study enrolling patients with metastatic uterine carcinosarcoma in patients previously exposed to platinum-based chemotherapy, testing pembrolizumab and lenvatinib regardless of microsatellite instability status.
Written consent was obtained from the patient for publication of this case report. It was conducted following the Declaration of Helsinki ethical principles, and Oncoclínicas Group Ethical Review Board approved it in January 2023 (Reference number 5.862.574).
Diocésio Andrade, Angelica Nogueira, Andreia Cristina de Melo, and Eduardo Paulino were responsible for the conceptualization and supervision of the manuscript. The original manuscript was drafted by Diocésio Andrade and subsequently reviewed and edited by all authors. All authors have contributed to the synthesis of the discussion and have approved the final version.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Collection and assembly of data, Conception and design, Data analysis
DAPA and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
EP Conception and design, Final approval of manuscript, Manuscript writing
IPCB Final approval of manuscript, Manuscript writing
DTW Final approval of manuscript, Manuscript writing
WPA Final approval of manuscript, Manuscript writing
ACM Conception and design, Final approval of manuscript, Manuscript writing
ANR Conception and design, Final approval of manuscript, Manuscript writing
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Miller, DS and Filiaci, VL and Mannel, RS and Cohn, DE and Matsumoto, T and Tewari, KS. Carboplatin and Paclitaxel for Advanced Endometrial Cancer: Final Overall Survival and Adverse Event Analysis of a Phase III Trial (NRG Oncology/GOG0209). J Clin Oncol [online]. 2020, vol. 38, p. 3841-50.
2. Heffernan, K and Nikitas, FS and Shukla, U and Camejo, HS and Knott, C. Previously treated recurrent or advanced endometrial cancer in England: a real-world observational analysis. Gynecol Oncol [online]. 2022, vol. 166, p. 317-25.
3. Makker, V and Colombo, N and Casado-Herráez, A and Santin, AD and Colomba, E and Miller, DS. Lenvatinib plus pembrolizumab for advanced endometrial cancer. N Engl J Med [online]. 2022, vol. 386, p. 437-48.
4. O’Malley, DM and Bariani, GM and Cassier, PA and Marabelle, A and Hansen, AR and Acosta, AJ. Pembrolizumab in patients with microsatellite instability-high advanced endometrial cancer: results from the KEYNOTE-158 Study. J Clin Oncol [online]. 2022, vol. 40, p. 752-61.
5. Oaknin, A and Gilbert, L and Tinker, AV and Brown, J and Mathews, C and Press, J. Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-H) or proficient/stable (MMRp/MSS) endometrial cancer: interim results from GARNET-a phase I, single-arm study. J Immunother Cancer [online]. 2022, vol. 10, p. e003777.
6. Kurman, RJ and Carcangiu, ML and Herrington, CS and Young, RH. Tumours of the uterine corpus. WHO Classification of Tumours of Female Reproductive Organs. International Agency for Research on Cancer (IARC), 2014.
7. Noh, JJ and Kim, MK and Choi, MC and Lee, JW and Park, H and Jung, SG. Frequency of mismatch repair deficiency/high microsatellite instability and its role as a predictive biomarker of response to immune checkpoint inhibitors in gynecologic cancers. Cancer Res Treat [online]. 2022, vol. 54, p. 1200-8.
8. Matsuzaki, S and Klar, M and Matsuzaki, S and Roman, LD and Sood, AK and Matsuo, K. Uterine carcinosarcoma: Contemporary clinical summary, molecular updates, and future research opportunity. Gynecol Oncol [online]. 2021, vol. 160, p. 586-601.
9. Matsuo, K and Ross, MS and Machida, H and Blake, EA and Roman, LD. Trends of uterine carcinosarcoma in the United States. J Gynecol Oncol [online]. 2018, vol. 29, p. e22.
10. Cherniack, AD and Shen, H and Walter, V and Stewart, C and Murray, BA and Bowlby, R. Integrated molecular characterization of uterine carcinosarcoma. Cancer Cell [online]. 2017, vol. 31, p. 411-23.
11. Segura, SE and Nobre, S and Hussein, YR and Abu-Rustum, NR and Weigelt, B and Soslow, RA. DNA mismatch repair-deficient endometrial carcinosarcomas portend distinct clinical, morphologic, and molecular features compared with traditional carcinosarcomas. Am J Surg Pathol [online]. 2020, vol. 44, p. 1573-9.
12. Hunt, JT and Chambers, LM and Yao, M and Joehlin-Price, A and Debernardo, R and Rose, PG. Lenvatinib plus pembrolizumab in patients with advanced or recurrent uterine carcinosarcoma. Gynecol Oncol Rep [online]. 2021, vol. 37, p. 100840.
13. Bhangoo, MS and Boasberg, P and Mehta, P and Elvin, JA and Ali, SM and Wu, W. Tumor mutational burden guides therapy in a treatment refractory POLEmutant uterine carcinosarcoma. Oncologist [online]. 2018, vol. 23, p. 518-23.
14. Zhu, B and Liu, Y and Li, J and Diao, L and Shao, L and Han-Zhang, H. Exceptional response of cryoablation followed by pembrolizumab in a patient with metastatic cervical carcinosarcoma with high tumor mutational burden: a case report. Oncologist [online]. 2020, vol. 25, p. 15-8.
15. NCT05147558 ClinicalTrialsgov Dec 07 [online]. Available from: <>.
Dados de acesso insuficientes para visualização no mapa.