Neuroblastoma (NB) is an embryonic cancer arising from neural crest stem cell and are seen in the adrenal medulla and anywhere along the peripheral sympathetic nervous system. It is almost exclusively a pediatric neoplasm and more than 90% of patients are diagnosed under ten years of age.(
It is characterized by a striking heterogeneity of histology and genetic aberrations resulting in a broad spectrum of clinical behavior, which can range from spontaneous regression to aggressive disease with metastatic dissemination leading to death despite intensive therapy. Usually, adult patients have a poorer outcome compared to children.(
The diagnosis of adult-onset neuroblastoma is challenging because of its rarity. The most common presentation of neuroblastoma is a painless abdominal mass. Other signs and symptoms can be related to mass effect from the primary tumor, or as a result of metastatic disease, or paraneoplastic syndromes.(
NB in adults is divided into three categories: L1 - localized tumor, not involved victal structures, without imaging difined risk factors and confined a one body compartment. L2 - locorregional tumor with one or more imaging risk factors. M - metastic disease.(
Multimodal treatments are used, including surgery, chemotherapy, and radiotherapy. There are no well-established treatment guidelines for adults with neuroblastoma. In general, the treatment principle is decided by the risk assessment system.(
In patients with localized disease and low risk, surgery is the primary treatment modality, without the need for adjuvant chemotherapy and/or radiotherapy.(
There are only a few case reports about neuroblastoma in adult in the literature. Here, we present a rare case of anterior mediastinal neuroblastoma in a female adult associated with SIADH, which was treated by means of neoadjuvant chemotherapy, surgery and radiotherapy.
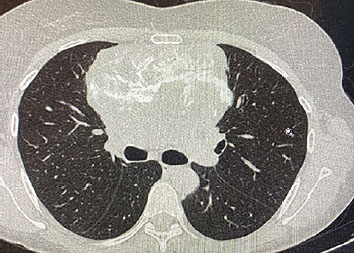
A 52-year-old female patient, hypertensive, without other relevant comorbidities, a mother with rectal cancer as the only cancer family history, began investigating respiratory tract infection in April 2020 during the pandemic COVID-19. Chest X-ray showed mediastinal enlargement and computed tomography (CT) of the chest performed in sequence showed a large expansive formation of the anterior mediastinum (12.0 x 6.0cm), involving the large vessels of the mediastinum and reducing the amplitude of the superior vena cava (
Figura 1 Anterior mediastinal mass on chest tomography (mediastinal window).
Figura 2 Anterior mediastinal mass on chest tomography (pulmonary window).
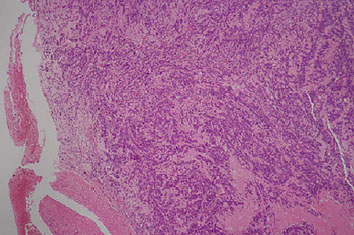
The patient was evaluated by thoracic surgery, which considered the tumor unresectable and performed diagnostic incisional biopsy on 10/16/2020. Pathological anatomy revealed small cell neoplasia in fibrillar matrix with histopathological picture suggestive of neurogenic neoplasia (
Figura 3 Neuroblastoma microscopy in smallest increase (HE): small cell neoplasm in fibrillar matrix with probable neurogenic origin.
| IMMUMOH1STOCHEMICAL MARKERS | RESULTS |
|---|---|
| AE1/AE3 | Negative |
| CK5/6 | Negative |
| CK4 | Negative |
| Ki67 | 20% |
| CD56 | Positive |
| Cromogranina | Positive |
| Sinaptofisina | Positive |
| Enolase | Positive |
| S100 | Positive |
| CD99 | Negative |
The staging was perfomed with abdominal tomography and bone scintigraphy, which did not show lesions suggestive of metastasis.
It was chosen to perform neoadjuvant chemotherapy, with subsequent radiological reassessment, in order to possible future surgical resection. The patient underwent a polychemotherapy regimen (doxorubicin, cisplatin, cyclophosphamide, and vincrinstine) for 6 cycles from December 2020 to April 2021, with excellent tolerance.
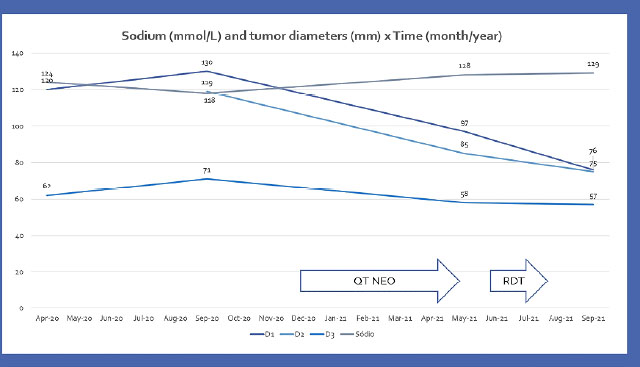
Radiological oncological restaging showed a partial response, with reduction of the dimensions of the mediastinal mass to 9.7 x 8.5 x 5.8cm. However, after the reassessment of thoracic surgery, it was still considered an unresectable neoplasm due to the invasion of large mediastinal vessels. Hyponatremia improved during neoadjuvant chemotherapy, corroborating the hypothesis of paraneoplastic SIADH (Na: 118 -> 125 -> 128 -> 129).
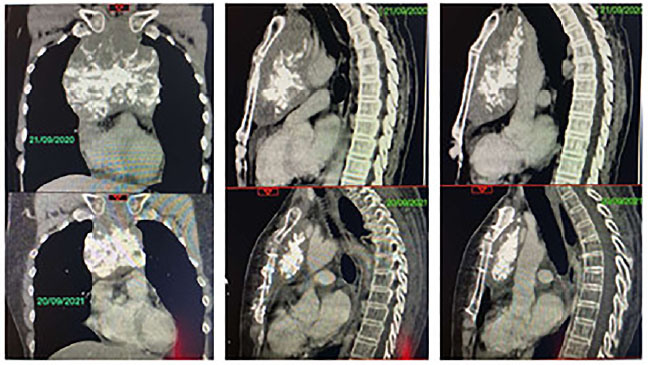
Opted for neoadjuvant radiotherapy, still in order to achieve resectability. He received radiotherapy from June to July 2021, with a total dose of 36Gy divided into 20 fractions. Chest tomography after 2 months of the end of radiotherapy, in September 2021, showed tumor reduction to 7.6 x 7.5 x 5.7 cm (
Figura 4 Comparison of tomographies before (above in 2020 year) and after (below in 2021 year) neoadjuvant treatment.
The patient was reevaluated again by thoracic surgery, which considered resection possible. She underwent thoracic surgery in March 2022. The anatomopathological of the surgery confirmed neuroblastoma, with the effect of previous neoadjuvant treatment in 80% of the sample evaluated (only 20% of residual disease), without neoplasia in pericardium liquid.
Unfortunately, the patient died due to postoperative complications (refractory hypotension/septic shock) in April 2022.
Initially, the pathology was compatible with neoplasm of small cells in the fibrillar matrix of neurogenic origin. Immunohistochemistry was essential to confirm thymic neuroblastoma and rule out other differential diagnoses such as small cell carcinoma and thymoma/thymic carcinoma.
Oncological staging in this patient, was performed with CT scans and conventional bone scintigraphy.
The intention of chemotherapy and subsequently radiotherapy with make the tumor resectable (neoadjuvant treatments). The chemotherapy protocol of choice was the ADOC regimen of the University of Turin for thymomas,(
The patient in question demonstrated a good response to neoadjuvant treatment both chemotherapy and radiotherapy, evidenced by the partial response in radiological restaging examinations, and by the treatment effect (80%) in pathological anatomy of surgery. High dose chemotherapy and surgery can achieve minimal disease state in >50% of newly diagnosed older NB patients.(
This case report brings together, several particularities, that are rare: NB of anterior mediastinum/thymus, NB in adult, SIHAD associated with NB. For these three particularities together, the literature review is scarce and is limited to case reports.(
The improvement in hyponatremia that occurred during neoadjuvant treatment corroborates the possibility of a paraneoplastic syndrome (SIADH) (
Therapeutic strategies remain uncertain due to the scarcity of scientific studies of this neoplasm in this specific population, related to its rarity. Extrapolation of NB therapeutic strategies in children, with adaptation for the adult age group, aiming to improve tolerance, remains the main option in this context.
Figura 5 Sodium and tumor diameters throughout neoadjuvant treatment.
CSS Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
CMBP Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
JSF Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
PRFA Provision of study materials or patient
LCR Provision of study materials or patient
JMN Provision of study materials or patient
LOPS Collection and assembly of data
CMSB Collection and assembly of data
MOES Collection and assembly of data
LCP Collection and assembly of data
MSR Collection and assembly of data
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Rogowitz, E and Babiker, HM and Kanaan, M and Millius, RA and Ringenberg, QS and Bishop, M. Neuroblastoma of the elderly, an oncologist’s nightmare: case presentation, literature review and SEER database analysis. Exp Hematol Oncol [online]. 2014, vol. 3, p. 20.
2. Podda, MG and Luksch, R and Polastri, D and Gandola, L and Piva, L and Collini, P. Neuroblastoma in patients over 12 years old: a 20-year experience at Instituto Nazionale Tumori of Milan. Tumori [online]. 2010, vol. 96, p. 684-9.
3. Ministério da Saúde (BR). Tipos de câncer - câncer infantojuvenil [Internet]. Ministério da Saúde/INCA, 2023.
4. Esiashivili, N and Goodman, M and Ward, K and Marcus, RB and Johnstone, PAS. Neuroblastoma in adults: incidence and survival analysis based on SEER data. Pediatr Blood Cancer [online]. 2007, vol. 48, p. 41-6.
5. Yanik, F and Karamustafaoglu, A and Yoruk, Y. A rare mediastinal occurrence of neuroblastoma in an adult: case report. São Paulo Med J [online]. 2019, vol. 137, p. 104-6.
6. Duan, K and Dickson, BC and Marrano, P and Thorner, PS and Chung, CT. Adult-onset neuroblastoma: report of seven cases with molecular genetic characterization. Genes Chromosomes Cancer [online]. 2020, vol. 59, p. 240-8.
7. Tolbert, VP and Matthay, KK. Neuroblastoma: clinical and biological approach to risk stratification and treatment. Cell Tissue Res [online]. 2018, vol. 372, p. 195-209.
8. Newman, E and Abdessalam, S and Aldrink, JH and Austin, M and Heaton, TE and Bruny, J. Update on neuroblastoma. J Pediatr Surg [online]. 2019, vol. 54, p. 383-9.
9. Brisse, H and McCarville, MB and Granata, C and Krug, KB and Wootton-Gorges, SL and Kanegawa, K. Guidelines for imaging and staging of neuroblastic tumors: consensus report from the International Neuroblastoma Risk Group Project. Radiology [online]. 2011, vol. 261, p. 243-57.
10. Vik, TA and Pfluger, T and Kadota, R and Castel, V and Tulchinsky, M and Farto, JCA. (123)I-mIBG scintigraphy in patients with known or suspected neuroblastoma: Results from a prospective multicenter trial. Pediatr Blood Cancer [online]. 2009, vol. 52, p. 784-90.
11. Taggart, D and Han, MM and Quach, A and Groshen, S and Ye, W and Villablanca, JG. Comparison of iodine-123 metaiodobenzylguanidine (MIBG) scan and 18FFluorodeoxyglucose positron emission tomography to evaluate response after iodine-131 MIBG therapy for relapsed neuroblastoma. J Clin Oncol [online]. 2009, vol. 27, p. 5343-9.
12. Monclair, T and Brodeur, GM and Ambros, PF and Brisse, HJ and Cecchetto, G and Holmes, K. The International Neuroblastoma Risk Group (INRG) staging system: an INRG Task Force report. J Clin Oncol [online]. 2009, vol. 27, p. 298-303.
13. Shimada, H and Ambros, IM and Dehner, LP and Hata, J and Joshi, VV and Roald, B. The International Neuroblastoma Pathology Classification (the Shimada system). Cancer [online]. 1999, vol. 86, p. 364-72.
14. Nakagawara, A and Li, Y and Izumi, H and Muramori, K and Inada, H and Nishi, M. Neuroblastoma. Jpn J Clin Oncol [online]. 2018, vol. 48, p. 214-41.
15. Tan, B and Li, JF and Li, WS and Yang, RL. Primary thoracic neuroblastoma in an adult. A rare case report. Medicine (Baltimore) [online]. 2019, vol. 98, p. e16564.
16. Perez, CA and Matthay, KK and Atkinson, JB and Seeger, RC and Shimada, H and Haase, GM. Biologic variables in the outcome of stages I and II neuroblastoma treated with surgery as primary therapy: a children’s cancer group study. J Clin Oncol [online]. 2000, vol. 18, p. 18-26.
17. Bernardi, B and Mosseri, V and Rubie, H and Castel, V and Foot, A and Ladenstein, R. Treatment of localised resectable neuroblastoma. Results of the LNESG1 study by the SIOP Europe Neuroblastoma Group. Br J Cancer [online]. 2008, vol. 99, p. 1027-33.
18. Matthay, K and Perez, C and Seeger, RC and Brodeur, GM and Shimada, H and Atkinson, JB. Successful treatment of stage III neuroblastoma based on prospective biologic staging: a Children’s Cancer Group study. J Clin Oncol [online]. 1998, vol. 16, p. 1256-64.
19. Haas-Kogan, D and Swift, PS and Selch, M and Haase, GM and Seeger, RC and Gerbing, RB. Impact of radiotherapy for high-risk neuroblastoma: a Children’s Cancer Group study. Int J Radiat Oncol Biol Phys [online]. 2003, vol. 56, p. 28-39.
20. Matthay, K and Reynolds, CP and Seeger, RC and Shimada, H and Adkins, ES and Haas-Kogan, D. Long-term results for children with high-risk neuroblastoma treated on a randomized trial of myeloablative therapy followed by 13-cis-retinoic acid: a children’s oncology group study. J Clin Oncol [online]. 2009, vol. 27, p. 1007-21.
21. Kushner, BH and Kramer, K and LaQuaglia, MP and Modak, S and Cheung, NKV. Neuroblastoma in adolescents and adults: the Memorial Sloan-Kettering experience. Med Pediatr Oncol [online]. 2003, vol. 41, p. 508-15.
22. Shusterman, S and London, WB and Gillies, SD and Hank, JA and Voss, SD and Seeger, RC. Antitumor activity of hu14.18-IL2 in patients with relapsed/refractory neuroblastoma: a Children’s Oncology Group (COG) phase II study. J Clin Oncol [online]. 2010, vol. 28, p. 4969-75.
23. Berruti, A and Borasio, P and Gerbino, A and Gorzegno, G and Moschini, T and Tampellini, M. Primary chemotherapy with adriamycin, cisplatin, vincristine and cyclophosphamide in locally advanced thymomas: a single institution experience. Br J Cancer [online]. 1999, vol. 81, p. 841-5.
24. Argani, P and Erlandson, RA and Rosai, J. Thymic neuroblastoma in adults: report of three cases with special emphasis on its association with the syndrome of inappropriate secretion of antidiuretic hormone. Am J Clin Pathol [online]. 1997, vol. 108, p. 537-43.
25. Ueda, Y and Omasa, M and Taki, T and Okabe, R and Cho, H and Shoji, T. Thymic neuroblastoma within a thymic cyst in an adult. Case Rep Oncol [online]. 2012, vol. 5, p. 459-63.
26. Pellegrino, M and Gianotti, L and Cassibba, S and Brizio, R and Terzi, A and Borretta, G. Neuroblastoma in the Elderly and SIADH: case report and review of the literature. Case Rep Med [online]. 2012, vol. 2012, p. 952645.

Dados de acesso insuficientes para visualização no mapa.