Multiple myeloma (MM) is characterized by monoclonal multiplication and accumulation of malignant plasma cells in the bone marrow, accounting for approximately 10% of all hematologic neoplasms. It remains incurable, and most patients have an overall survival following diagnosis of up to 5 years.
Although testing of new chemotherapy agents has shown good outcomes for duration of disease remission,
Because of different mechanisms that may be involved in the development of drug resistance in MM, the treatment of patients with refractory disease is challenging and needs to be continuously studied.
Treatment options for primary or refractory MM generally include different combinations of drugs with different mechanisms of action, such as corticosteroids, immunomodulatory drugs, and monoclonal antibodies, as well as autologous stem cell transplantation.
CAR-T cells are the patient’s own T cells that were genetically modified to obtain enhanced and specific cytotoxic activity.
The is a systematic review based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria.
The PubMed database (MEDLINE) was used to search for the combination of terms “multiple myeloma” [MeSH Terms] OR “refractory multiple myeloma” [Title/Abstract] AND “CAR T-cell” [Title/Abstract]. The terms should appear in at least one of three search fields, i.e., title, keywords, or abstract. No other filters were added. The search strategy was used in October 2020. All identified records were exported and contained at least information about the authors, year and journal of publication, title, and abstract.
Potentially eligible articles were evaluated using Microsoft Excel®. The articles were initially selected by title and abstract screening. The inclusion criteria were as follows: being an original article based on a randomized clinical trial; investigating primary treatment with CAR-T cells; having refractory MM as an outcome or exposure; and being written in English. The articles selected for full-text screening were located and exported in PDF format,
and the evaluation followed the same criteria previously established. Finally, the selected studies had their references analyzed to identify possible new articles as well as gray literature.
The entire selection process was carried out by the two authors (SS and VS) independently. Articles selected by both authors were included, and those not selected by any author were excluded. The articles included by only one of the authors were analyzed in a meeting, and the judgment for including or excluding them, according to the eligibility criteria, was discussed.
Data were extracted using Microsoft Excel® to identify the studies, including main author, year of publication, place where the study was developed, study phase, CAR-T cell target, number of patients, and others. Data extraction was performed by one author (SS) and analyzed by the other (VS) independently.
A risk-of-bias assessment of included studies improves the reliability of the results of a systematic review
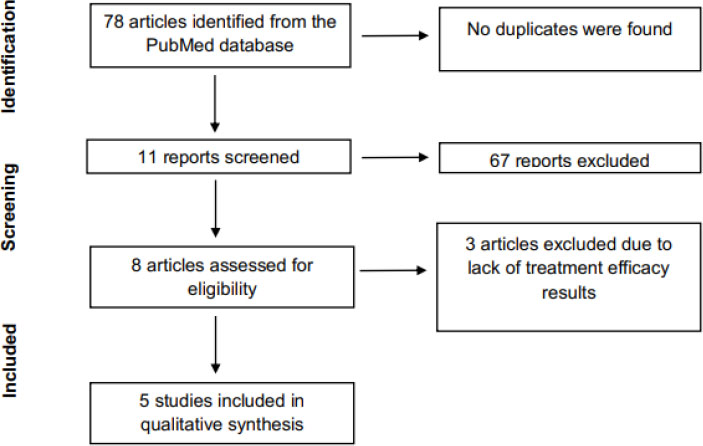
Seventy-eight articles were identified as potentially eligible. An initial evaluation following the established criteria resulted in 11 articles, and eight were selected for full-text screening. Three articles were then excluded because their results did not mention whether the treatment used was effective. Thus, five articles were included in qualitative analysis, as shown in the flow diagram below (
The five included articles were then analyzed. An overview of reviewed studies is shown in
The selected articles were published by research teams in the United States (2 articles) and China (3 articles) between 2018 (2 articles) and 2019 (3 articles), having BCMA as a common target. Three articles refer to open-label, phase I studies, one article refers to a single-arm, phase II study, and one article does not mention the clinical phase but indicates that it refers to a clinical study.
All articles state that patients received previous lines of anti-MM therapy, not responding to them, and two articles inform those patients underwent autologous stem cell transplantation. Also, all study patients received lymphodepletion before CAR-T cell infusion.
| Bias domain | Source of bias | Support for authors’ judgment | Risk of bias |
|---|---|---|---|
| Random sequence generation | Describe the method used to generate the allocation sequence to determine whether the study groups are comparable. | High | |
| Selection | Allocation concealment | Describe the method used to conceal the allocation sequence to determine whether allocations could have been foreseen before or during the intervention. | Unclear |
| Performance | Blinding of participants and personnel | Describe the measures used to blind trial participants and researchers from knowledge of which intervention a participant received. | Low* |
| Detection | Blinding of outcome assessment | Describe the measures used to blind outcome assessment from knowledge of which intervention a participant received. | Low |
| Attrition | Incomplete outcome data | Describe the completeness of outcome data for each main outcome, including exclusions from the analysis, as well as the numbers in each intervention group (compared with total randomized participants) and reasons for attrition or exclusions. | High |
| Reporting | Selective reporting | State how selective outcome reporting was examined and what was found. | High |
| Other | Any other type of bias | State any important concerns about bias not covered in the other domains. | Low |
All participants received the expected treatment.
There were differences in the CAR-T cell infusion protocols used in the studies. Raje et al. (2019),
The dosages used in the studies were also different. Raje et al. (2019)
Despite the use of different doses, anti-BCMA CAR-T cells were detected in the peripheral blood of all patients, persisting for at least 1 month to up to 1 year.
Raje et al. (2019)
Zhao et al. (2018)
Figura 1 PRISMA flow diagram of study selection.
Yan et al. (2019)
Some studies evaluated persistence of CAR-T cells in peripheral blood. Raje et al. (2019)
In all studies
Criteria for Adverse Events, version 4.0.
The CRS was reported by all authors and most of the manifestation was classified in Grade 1 to/or 2 (
| Author/Title | Year | Country | Study phase | study type | CAR-T cell therapy | Target | Number of patients | Lymphodepletion | CAR-T cell dose (cells/kg) | Previous lines of therapy |
|---|---|---|---|---|---|---|---|---|---|---|
| Brudno et al. | 2018 | United States | - | Clinical trial | CAR- BMCA | Anti-BCMA | 16 in this study (24 in total) | Fludarabine + cyclophosphamide | In this study = 9×106 (escalation: 0.3x106, 1×106 3×106, and 9×106) | Median, 9.5 previous therapies |
| Xu et al.[10] Exploratory trial of a biepitopic CAR T- targeting B cell maturation antigen in relapsed/refractory multiple myeloma | 2019 | China | I | Open-label | LCAR- B28M | Two epitopes of BCMA | 17 | Cyclophosphamide (9 patients) Fludarabine + cyclophosphamide (8 patients) | Single dose = 0.70×106 3 infusions (days 0,3, and 6) of a dose of 0.7×106 | 12 received at least three previous protocols of chemotherapy, immunomodulatory drugs, and proteasome inhibitors 8 transplant patients |
| Zhao et al. [7] A phase 1, open-label study of LCAR B38M, a chimeric antigen receptor T cell therapy directed against B cell maturation antigen, in patients with relapsed or refractory multiple Myeloma | 2018 | China | I | Open-label | LCAR- B28M | Two epitopes of BCMA | 57 | Cyclophosphamide | 3 infusions (20%, 30%, and 50% of total dose) Median, 0.5×106 | Proteasome inhibitors (68%) Immunomodulatory drugs (68%) Both (60%) |
| Raje et al.[16] Anti-BCMA CAR-T cell therapy bb2l21 in relapsed or refractory multiple myeloma | 2019 | United States | I | Open-label | bb2121 | Anti-BCMA | 33 | Fludarabine + cyclophosphamide | 50×106, 150×106, 450×106, or 800×106 (escalation) 150×106 to 450×106 (expansion) | Proteasome inhibitors and immunomodulatory drugs in 26 patients (79%) Bortezomib, carfilzomib, lenalidomide, pomalidomide, and daratumumab in 6 patients (18%) |
| Yan et al.[21] A combination of humanised anti-CD19 and anti-BCMA CAR T cells in patients with relapsed or refractory multiple myeloma; a single arm, phase 2 trial | 2019 | China | II | Single-arm | Anti-CDI9 Anti- BCMA | Anti-CDI9 Anti-BCMA | 21 | Fludarabine + cyclophosphamide | Both = 1×106 | Median, 6 previous therapies 3 transplant patients |
| Author/Title | Efficacy | Expansion and persistence | |
|---|---|---|---|
| Brudno et al. (2018) | - Overall response: 81% (1 patient had a marked decrease in MM markers, 13/16 patients had a partial response or better); - Progression-free survival (median, 31 weeks): 6 continued to respond and 10 progressed. - 6 months after infusion, IgG, IgM, and | IgA increased, indicative of plasma cell recovery. - Patients with anti-MM responses had decreased BCMA levels. | - Peak levels between 7 and 14 days in all patients. - CD8+ T cells acquired different phenotypes after infusion. |
| Xu et al. (2019) | - Objective response: 88.2% (13 patients with stringent complete responses and 2 with very good partial responses). - At 1 month: 1 had no obvious response; 15 had a response, of which 13 had a complete response and 2 had a partial response. - Sustained response (11 months after infusion): 7 complete responses + 1 partial response. - Relapse (5 to 11 months after response): 6 patients relapsed after complete response and 1 patient progressed after very good partial response. - Progression-free survival: 82.4% at 6 months and 52.9% at 12 months. | - Durable persistence: up to 9 months. | |
| Zhao et al. (2018) | - Median follow-up: 8 months. - Overall response: 88% (39 patients [68%] had a complete response, 3 [5%] had a very good partial response, and 8 [14%] had a partial response). - MRD: 36 patients were MRD-negative and achieved a complete response. - Progression (median progression-free survival, 15 months): 10 patients (20%) who achieved a partial response then progressed. | - BCMA expression: 26/53 patients (49%) had <40% expression and 27/53 patients (51%) had ≥40% expression. - In 71% of patients, LCAR- B38M was not detectable at 4 months. - Only 5 patients showed persistence up to 10 months. | |
| Raje et al. (2019) | - Objective response: 85% (9% with complete responses and 36% with stringent complete responses). - Dose-dependent effect on the frequency and duration of response. - Very good partial response or better at a dose of 150×106 CAR+ T cells. - Response rate ≥74% among patients who progressed after most recent therapy, those who received daratumumab, or those who had plasmacytomas. - At a dose of 450×106, the same response was obtained in patients with BCMA expression above or below 50%. - Early treatment response: median time to 1st partial response or better was 1 month. - MRD: 18 patients (16 had a partial response or better and 2 had no response). At first assessment: 16 MRD-negative patients at 10−4 nucleated cells, 15 MRD-negative patients at 10−5 nucleated cells, and 3 MRD-negative patients at 10−6 nucleated cells. Of these, 12 had at least two consecutive negative assessments; - Median duration of follow-up: 11.3 months;w - Progression: 17 patients (52%) progressed, including 12 who had a response (6 with complete responses and 6 with MRD-negative responses). | - Variable proportion of CAR+ T cells: 85% CD4 and 13% CD8; - bb2121 was detectable at a dose of 50×106 CAR+ T cells; - Durable persistence: 96% of patients at 1 month, 86% of patients at 3 months, 57% of patients at 6 months, 20% of patients at 12 months. | |
| Yan et al. (2019) | - Overall response: 95% (9 patients [43%] had a stringent complete response, 3 (14%) had a complete response, 5 [24%] had a very good partial response, and 3 [14%] had a partial response). - Median follow-up: 268 days. - Relapse: 17/20 (85%) did not relapse or progress. - Progression-free survival (median, 243 days, partial response or better): 9/21 (43%) maintained a complete response or better for more than 6 months, 4 (19%) maintained a stringent complete response for more than 1 year, and 1 (5%) had no relapse at 602 days. - MRD: 17/21 (81%) were MRD-negative, with 16/17 (94%) remaining MRD-negative 1 month after infusion. | - BCMA expression: detected in 20 patients. - CD19-CAR amplification: peak on day 7 followed by a decrease. - BCMA-CAR amplification: peak between days 7 and 14 followed by a gradual decrease. - Number of plasma cells in bone marrow was associated with peak BCMA-CARs. |
When it was necessary, they used mainly tocilizumab to treat toxicities. Raje et al. (2019)
BCMA was a common target in the reviewed studies. This antigen is expressed on the surface of both normal and malignant plasma cells, and can be found in a soluble form (sBCMA) in circulation.
Brudno et al. (2018)
Although they did not find a correlation between BCMA expression and treatment response, Zhao et al. (2018)
Another common result in the reviewed studies was the absence of MRD in treated patients, especially those who achieved a complete response or very good partial response. Although the definition of MRD negativity depends on the method used,
However, even with high rates of MRD negativity after CAR-T cell therapy, some patients relapsed.
A decrease in response durability in patients who were MRD-negative following CAR- T cell therapy may be related to a number of factors such as level of BCMA expression, absence of BCMA, or loss of BCMA function in MM cells.
| Author/Title | Cytokine release syndrome | Others adverse events |
|---|---|---|
| Brudno et al. (2018) | - Reported only results for dose 9 x 106 CAR+ T cells/kg. - Grade 1: 2 cases; Grade 2: 7 cases; Grade 3: 4 cases; Grade 4: 2 cases. - Use of tocilizumab and glucocorticoids to treat syndrome. | - Hematological: anemia (11/16 - grade 3); lymphopenia (5/16 grade 3; 10/16 grade 4), neutropenia (6/16 grade 3; 8/16 grade 4), platelet count decreased (3/16 grade 3; 7/16 grade 4). - Others Grade 3: hypophosphatemia (11/16); fever (9/16); hypotension (5/16); sinus tachycardia (5/16); hypokalemia (5/16); hyponatremia (4/16); hypoxia (4/16); dyspnea (4/16); AST increase (3/16). |
| Xu et al. (2019) | - Grade 1-2: 10 cases; Grade 3: 6 cases; Grade 5: 1 case. - The grades were associated with the abundance of BCMA. - Increased of IL-6, IL-10 and TNF-α. - Tocilizumab was used to treat 3 cases which complicated. | - All 17 patients had an adverse event. - Fever: Grade 1-2: 8 patients; Grade 3-4: 9 patients. - AST increased in 16 patients and ALT in 7 cases. - Tumor lysis syndrome was observed in 3 patients. - Others: hypotension (5/17); hypoxemia (4/17); prolonged activated partial thromboplastin time (2/17); systemic edema (1/17); renal impairment (1/17). |
| Zhao et al. (2018) | - About 51 patients (90%). - Grade 1-2:47 patients (83%); Grade 3-4: 4 patients (7%). - Median time to onset: 9 days. - Median duration: 9 days. - The syndrome was managed with tocilizumab, vasopressor and supplemental oxygen. - One patient developed Grade 2 cytokine release syndrome with dose 1.8×106 CAR+ T cell/kg, and evolved to ventilator support, dying after reported Grade 5 pulmonary embolism and acute coronary syndrome. | - All 57 patients reported an adverse event. - Most patients (65%) had Grade 3 adverse events. - Neurotoxicity: observed in 1 patient at dose 1.0 × 106 CAR+ T cell/kg, who developed grade 1 aphasia, agitation, and seizure-like activity. - Others: pyrexia (91%); thrombocytopenia (90%); leukopenia (47%); ALT increased (39%); anemia (30%); hypotension (21%); ALT increased (18%); cough (18%); disseminated intravascular coagulation (18%); hypocalcemia (16%); hyponatremia (14%); dyspnea (11%); nausea (11%). |
| Raje et al. (2019) | - Total of 25 patients. - Grade 1 or 2: 23 patients (70%); Grade 3: 2 patients (6%); Grade 4 or higher: none. - Median time to onset: 2 days. - Median duration: 5 days. - Correlated with the dose: > 150×106 CAR+ T cells. - Associated with a higher peak level of serum C-reactive protein and TNF-α. - Tocilizumab and glucocorticoids were used to manage the syndrome. | - All 33 patients had an adverse event. - Hematologic: neutropenia (in 83%); leukopenia (in 58%); anemia (in 45%); thrombocytopenia (in 45%) (all expected because of lymphodepleting chemotherapy). - Neurological: 13 patients had grade 1 or 2 (42%); 1 patient had grade 4 neurologic toxicity after 11 days of infusion. - Infection development: 14 patients (42%); 2 patients had grade 3 (anal abscess and parvovirus infection); no grade 4 occurred. - Gastrointestinal: constipation (27%); nausea (21%); diarrhea (21%), vomiting (18%). - Other: fatigue (42%); headache (30%); hypocalcemia (27%); hypokalemia (24%); hypophosphatemia (21%); peripheral edema (18%); hyperglycemia (18%); hypoalbuminemia (18%); cough (18%); sinus tachycardia (15%); hypotension (15%); hyponatremia (15%). |
| Yan et al. (2019) | - Observed in 19 (90%) of 21 patients. - Grade 1 or 2: 18 patients (86%); Grade 3: 1 patient (5%). - Principal manifestation: Fever - occurred median: 9 days; Median duration: 4 days | - Encephalopathy syndrome: Two (10%) of 21 patients. - Hematological: Grade 3 to 4 Leukopenia in 18 patients (86%); Grade 3 Anemia in 13 patients (62%); Grade 3 to 4 Thrombocytopenia in 13 patients (62%). - All 21 patients had B-cell aplasia. - One patient (5%) had Grade 5 cerebral hemorrhage. - Other: muscle weakness (90%); prolonged activated partial thromboplastin time (38%); hypoxemia (29%); AST increase (29%); ALT increase (19%); nausea (10%); vomiting (10%); myalgias (10%); hypotension (10%). |
Legend: ALT = Alanine aminotransferase; AST = Aspartate aminotransferase; IL-6 = Interleukin 6; IL-10 = Interleukin 10; TNF-α: Tumor necrosis factor-α.
For all reviewed studies, safety of CAR-T cell infusion was analyzed. The common adverse event reported was CRS. To Raje et al. (2019)
Brudno et al. (2018)
Zhao et al. (2018)
During the research, Xu et al. (2019)
Despite all articles reporting adverse events, the reviewed studies also found positive and promising results, including responses to CAR-T cell therapy higher than 80%. Brudno et al. (2018)
Both Xu et al. (2019)
Given the encouraging results of the use of CAR-T cells in anti-MM therapy, all authors suggested that they should be incorporated into treatment options and evaluated in new studies. Xu et al. (2019)
Despite all advances in research into new treatments, MM remains an incurable disease. The use of anti-MM CAR-T cell therapy has shown promising results and must continue to be studied, even if some patients still relapse or progress after treatment. Most types of CAR-T cell therapy discussed in this review are able to maintain undetectable MRD levels and increase progression-free survival time, resulting in an improved quality of life for patients.
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
SS Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
VS Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Rajkumar, SV. Multiple myeloma: 2018 update on diagnosis, risk-stratification and management. Am J Hematol [online]. 2019, vol. 93, p. 981-1114.
2. Ria, R and Vacca, A. Bone marrow stromal cells-induced drug resistance in multiple myeloma. Int J Mol Sci [online]. 2020, vol. 21, p. 613.
3. Tang, F and Lu, Y and Ge, Y and Shang, J and Zhu, X. Infusion of chimeric antigen receptor T-cells against dual targets of CD19 and B cell maturation antigen for the treatment of refractory Multiple Myeloma. J Int Med Res [online]. 2020, vol. 48, p. 1-7.
4. Rajkumar, SV and Kumar, S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc [online]. 2016, vol. 91, p. 101-19.
5. Pinto, V and Bergantim, R and Caires, HR and Seca, H and Guimarães, J and Vasconcelos, MH. Multiple myeloma: available therapies and causes of drug resistance. Cancers [online]. 2020, vol. 12, p. 407.
6. Roshal, M. Minimal residual disease detection by flow cytometry in multiple myeloma: why and how?. Semin Hematol [online]. 2018, vol. 55, p. 4-12.
7. Zhao, WH and Liu, J and Wang, BY and Chen, YX and Cao, XM and Yang, Y. A phase 1, open-label study of LCAR-B38M, a chimeric antigen receptor T cell therapy directed against B cell maturation antigen, in patients with relapsed or refractory multiple myeloma. J Hematol Oncol [online]. 2018, vol. 11, p. 141.
8. Lee, J and Kim, SH. Treatment of relapsed and refractory multiple myeloma. Blood Res [online]. 2020, vol. 55, p. S43-S53.
9. Chim, CS and Kumar, SK and Orlowski, RZ and Richardson, PG and Gertz, MA and Giralt, S. Management of relapsed and refractory Multiple Myeloma: novel agents, antibodies, immunotherapies and beyond. Leukemia [online]. 2018, vol. 32, p. 252-62.
10. Xu, J and Chen, LJ and Yang, SS and Sun, Y and Wu, W and Liu, YF. Exploratory trial of a biepitopic CAR T-targeting B cell maturation antigen on relapsed/refractory multiple myeloma. PNAS license [online]. 2019, vol. 116, p. 9543-51.
11. Maples, KT and Joseph, NS and Harvey, RD. Current developments in the combination therapy of relapsed/refractory multiple myeloma. Expert Rev Anticancer Ther [online]. 2020, vol. 20, p. 1021-35.
12. Dempsey, JL and Johns, A and Rosko, AE and Lazarus, HM. The pharmacologic management of multiple myeloma in older adults. Expert Opin Pharmacother [online]. 2019, vol. 20, p. 887-902.
13. Petty, AJ and Heyman, B and Yang, Y. Chimeric antigen receptor cell therapy: overcoming obstacle to battle cancer. Cancers [online]. 2020, vol. 12, p. 842.
14. Zhang, Q and Ping, J and Huang, Z and Zhang, X and Zhou, J and Wang, G. CAR T-cell therapy in cancer: tribulations and road ahead. J Immunol Res [online]. 2020, vol. 2020, p. 1924379.
15. Huang, H and Wu, HW and Hu, YX. Current advances in chimeric antigen receptor T-cell therapy for refractory/relapsed multiple myeloma. J Zhejiang Univ Sci B [online]. 2020, vol. 21, p. 29-41.
16. Raje, N and Berdeja, J and Lin, Y and Siegel, D and Jagannath, S and Madduri, D. Anti-BCMA CAR T-cell therapy bb2121 in relapsed or refractory multiple myeloma. N Engl J Med [online]. 2019, vol. 380, p. 1726-37.
17. Brudno, JN and Maric, I and Hartman, SD and Rose, JJ and Wang, M and Lam, N. T cells genetically modified to express an anti B cell maturation antigen chimeric antigen receptor causes remissions of poor prognosis relapsed Multiple Myeloma. J Clin Oncol [online]. 2018, vol. 36, p. 2267-79.
18. The PRISMA Group. Preferred reporting items for systemic review and meta-analyses: the PRISMA statement. PLoS Med [online]. 2009, vol. 6, p. e1000097.
19. Barbosa, TF and Lira, AB and Neto, OBO and Santos, LL and Santos, IO and Barbosa, LT. Tutorial para execução de revisões sistemáticas e metanálises com estudos de intervenção em anestesia. Rev Bras Anestesiol [online]. 2018, vol. 69, p. 299-306.
20. Higgins, JP and Altman, DG and Gotzsche, PC and Jüni, P and Moher, D and Oxman, AD. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ [online]. 2011, vol. 343, p. d5928.
21. Yan, Z and Cao, J and Cheng, H and Qiao, J and Zhang, H and Wang, Y. A combination of humanized anti-CD19 and anti-BCMA CAR T cells in patients with relapsed or refractory multiple myeloma: a single-arm, phase 2 trial. Lancet Haematol [online]. 2019, vol. 6, p. E521-E9.
22. Version 4.0 [internet]. U.S. Department of Health and Human Service, 2009.
23. Lee, DW and Gardner, R and Porter, DL and Louis, CU and Ahmed, N and Jensen, M. Current concepts in the diagnosis and management of cytokine release syndrome. Blood [online]. 2014, vol. 124, p. 188-95.
24. Neelapu, SS and Tummala, S and Kebriaei, P and Wierda, W and Gutierrez, C and Locke, FL. Chimeric antigen receptor T-cell therapy – assessment and management of toxicities. Nat Rev Clin Oncol [online]. 2018, vol. 15, p. 47-62.
25. Cho, SF and Anderson, KC and Tai, YT. Targeting B cell maturation antigen (BCMA) in multiple myeloma: potential uses of BCMA-based immunotherapy. Front Immunol [online]. 2018, vol. 9, p. 1821.
26. Cohen, AD and Garfall, AL and Stadmauer, EA and Melenhorst, JJ and Lacey, SF and Lancaster, E. B cell maturation antigenspecific CAR T cells are clinically active in multiple myeloma. J Clin Invest [online]. 2019, vol. 129, p. 2210-21.
27. Caraccio, C and Krishna, S and Philips, DJ and Schürch, CM. Bispecific antibodies for multiple myeloma: a review of targets, drugs, clinical trials and future directions. Front Immunol [online]. 2020, vol. 11, p. 501.
28. Cho, SF and Lin, L and Xing, L and Li, Y and Yu, T and Anderson, KC. BMCA-targeting therapy: driving a new era of immunotherapy of multiple mieloma. Cancers (Basel) [online]. 2020, vol. 12, p. 1473.
29. Shah, N and Aiello, J and Avigan, DE and Berdeja, JG and Borrello, IM and Chari, A. The Society for Immunotherapy of cancer consensus statement on immunotherapy for the treatment of multiple myeloma. J Immunother Cancer [online]. 2020, vol. 8, p. e000734.
30. Radhakrishnan, S and Luetkens, T and Scherer, SD and Davis, P and Mause, ERV and Olson, ML. CD229 CAR T-cell eliminate multiple myeloma and tumor propagating cells without fratricide. Nat Commun [online]. 2020, vol. 11, p. 798.
Dados de acesso insuficientes para visualização no mapa.