Prostate cancer (PCa) is the most prevalent tumor among men except for non- melanoma skin cancers. According to Brazilian National Cancer Institute (INCA), 68,220 new cases of prostate cancer are estimated for 2018 being the second leading cause of cancer deaths in Brazil.(
A portion of patients with early stage disease submitted to locoregional treatment will relapse of the disease and may require systemic treatment. There is another part of the patients presenting with metastatic disease at diagnosis (metastatic “di novo”) and will also need systemic treatment.
During the last decade, the treatment of metastatic prostate cancer has dramatically changed with the approval of seven new agents for patients with metastatic castration-resistant prostate cancer (mCRPC). These new therapeutic options have provided an overall survival (OS) increase from 9-18 months(
Although several agents have resulted in improvement in OS in different scenarios of metastatic disease, head to head comparisons of efficacy and the best sequencing approach are questions that remain unanswered. Despite the advances in the tumor biology understanding, no predictive biomarkers of response are validated to be used in the clinical practice in order to choose the best therapeutic option. Unfortunately, clinical characteristics, such as PSA doubling time, exposure time to primary ADT, extent and location of metastatic disease, performance status (PS) and pathological features have been still used as tools to guide treatment selection.
In this manuscript, we review the latest evidence for treatment of mCSPC and mCRPC discussing the best options in each scenario and, in the absence of approved predictive biomarkers tests, how to choose subsequent treatments.
When metastatic disease is diagnosed, initial treatment of prostate cancer is testosterone suppression at castration levels. It can be done through surgical orchiectomy or drug blockade with GnRH antagonist or GnRH agonist. This stage of disease is called sensitive- castration prostate cancer.(
Despite the suppression of testosterone levels, after an average time of 18 to 24 months, the majority of patients invariably will present progression of disease (elevation of PSA and/or worsening of pre-existing metastatic lesions and/or the appearance of new metastatic lesions).(
The use of peripheral antiandrogens (bicalutamide, nilutamide, flutamide, etc.) associated with LHRH agonists (complete hormonal blockade) can be used for a short period of 2 to 4 weeks to avoid the worsening of symptoms (pain, urinary retention, etc.) that may be caused by a transient increase in testosterone (flare phenomenon).(
Recently three prospective randomized phase 3 studies (
The French trial GETUG-AFU 15 randomized 385 patients with mCSPC to ADT alone or in combination with docetaxel 75mg/m2 every 3 weeks for up to 9 cycles (ADT + D). This study demonstrated a benefit of median OS for the ADT plus docetaxel group but without statistical significance (46.5 vs 60.9 months, HR = 0.90, p = 0.44), independently of the extent of metastatic disease at diagnosis.(
On the other hand, the American trial CHAARTED-ECOG 3805 that randomized 790 patients with mCSPC for ADT alone or ADT + D every 3 weeks for up to 6 cycles, demonstrated better OS (around 13 months) for the ADT + D group (44 vs 57.6 months, HR = 0.61, p < 0.001).
A pre-specified subgroup analysis was performed according to the stage of the disease at the diagnoses. In those defined as high-volume disease (visceral metastasis or = 4 bone lesions with one lesion in the appendicular skeleton) the benefit of OS was even more expressive, approximately 17 months (32.2 vs 49.2 months, HR = 0.60, P < 0.001), but in those defined as low-volume disease there was no statistical benefit of OS.(
In the same context as previous trials, the STAMPEDE trial randomized 2962 patients with high risk localized disease or mCSPC to ADT or ADT + D every 3 weeks for up to 6 cycles and showed an improvement in OS for ADT + D group (71 vs 81 months, HR = 0.78, p = 0.006). In the patients with metastatic disease (61%) the OS benefit was even greater, around 22 months (HR = 0.76).(
A meta-analysis including several trials, including the three trials discussed above, evaluated the role of chemotherapy in men with high-risk localized or mCSPC and demonstrated an improvement in 4 year-survival of 9% (HR = 0.77; p < 0.0001) for ADT + D in those with metastatic disease.(
In, 2017, the Multicentric LATITUDE Trial randomized 1199 patients to abiraterone plus ADT or ADT alone. The patients were required to have at least two of the three following high-risk factors associated with poor prognosis: a Gleason score of 8 or more (on a scale of 2 to 10, with higher scores indicating more aggressive disease), at least three bone lesions and the presence of measurable visceral metastasis. Radiographic progression free survival (HR = 0.47, 95% CI:0.39-0.55, p < 0.001) (rPFS) and OS (56.3 vs 36.5 months, HR = 0.66, p < 0.0001), both primary endpoints, was significantly improved with the addition of abiraterone.(
| Study | N | Follow-up (months) | High-volume disease (%) | Gleason = 8 (%) | Age (years) | Patients who received the planned treatment (%) | Overall Survival (months) | HR and p |
|---|---|---|---|---|---|---|---|---|
| GETUG-AFU 15( | 385 | 84 | 52 | 55 | 64 | 48 | 46.5 (ADT) vs 60,9 (ADT+CHEMO) | 0.9 and 0.44 |
| CHAARTED( | 790 | 29 | 65 | 65 | 63 | 74 | 44 (ADT) vs 57.6 (ADT+CHEMO) | 0.61 and < 0.001 |
| STAMPEDE( | 2962 | 43 | NI | 74 | 65 | 77 | 71 (ADT) vs 81 (ADT+CHEMO) | 0.77 and < 0.0001 |
| LATITUDE( | 1199 | 30 | NI | 100 | 68 | 88 | 34.7 (ADT) vs NR (ADT + ABI) | 0.62 and < 0.001 |
| ARCHES( | 1150 | 14.4 | 62 | 67 | 70 | NI | NR (ADT) vs NR (ADT + ENZA) | 0.81 and 0.3361 |
The STAMPEDE trial had an arm that evaluated the benefit of adding abiraterone to ADT in patients with localized high risk and mCSPC. This strategy compared to ADT alone showed an improvement in OS (HR = 0.63, p < 0.001) and in failure free survival (HR = 0.29, p < 0.001). The OS in the 52% of the metastatic population was even better (HR = 0.61).(
In absence of a head-to-head trial, several comparisons studies, meta-analysis and a directly comparison in the STAMPEDE trial try to answer if abiraterone is better thandocetaxel in mCSPC setting. There is no evidence that one is better than the other in this scenario.(
Recently another new generation anti-androgen, enzalutamide, showed efficacy in mCSPC. ARCHES trial showed that addition of enzalutamide to ADT improves outcomes over ADT alone. Primary endpoint of rPFS favored enzalutamide plus ADT (HR = 0.39, p < 0.0001). All subgroup analysis was statistically in favor of combination, including patients with low and high volume (CHARTEED criteria) and prior docetaxel use or not. OS data are still immature.(
Local treatment was explored in mCSPC in two randomized trials comparing with standard of care (SOC). HORRAD trial compares the addition of radiotherapy to the prostate in patients with bone metastasis CSPC and use of ADT. OS was similar between groups (45 vs 43 months, HR = 0.9, p = 0.4). Patients with less than 5 bone metastasis had the best outcome, but still not statistically significant (HR = 0.68, CI = 0.42-1.1).(
Based on these two trials local treatment in mCSPC patients are not recommended routinely. It must be discussed in a tumor board session and with patients regarding efficacy and toxicities. There are a few trials evaluating the addition of local treatment in patients with mCSPC and new evidences will be available soon.
The choice of treatment should include a discussion with the patient about the potential toxicities associated with abiraterone and docetaxel, as well as the duration, oncologist's experience and access, patient's desire and cost of treatment.
Castration-resistant prostate cancer is defined as an elevation in PSA levels between two consecutive measurements (minimum interval of 3 weeks), with serum testosterone below 50 ng/dl, in the presence of hormonal blockade.(
There are currently seven therapeutic agents, with different mechanisms of action and outcomes for the treatment of mCRPC (
Until 2010, docetaxel (taxane) was the only agent with OS improvement and it was the standard firstline therapy for mCRPC. The phase III study TAX 327 randomized 1006 mCRPC patients to receive Docetaxel 75mg/m2 every 3 weeks for up to 10 cycles versus Docetaxel 30mg/m2 weekly versus Mitoxantrone 12mg/m2 every 3 weeks and showed an improvement of OS for Docetaxel every 3 weeks (19.2 vs 17.8 vs 16.9 months, HR = 0.79, p = 0.004) in all subgroups. (symptomatic vs asymptomatic, presence vs absence of visceral metastases, good KPS vs poor KPS and age < 68 years vs = 69 years), The patients in the docetaxel every 3 weeks group also presented a higher PSA response rate of 50% and improvement in QoL.(
Another option for the use of docetaxel is the schedule every 2 weeks, based on a randomized phase 3 study of 177 patients which compared docetaxel 50mg/m2 every 2 weeks versus docetaxel 75mg/m2 every 3 weeks and demonstrated an increase in time to treatment failure (5.6 vs 4.9 months, p = 0.01), a lower incidence of grade 3 and 4 neutropenia (36 vs 53%) and lower incidence of febrile neutropenia (4 vs 14%) for the use every 2 weeks.(
Cabazitaxel is a new generation taxane developed to overcome resistance to docetaxel. In addition, this drug has the capacity to cross the blood-brain barrier.(
|
| Scenario/Stage | Administration | Corticoid | PSA response | OS |
|---|---|---|---|---|---|
| Docetaxel | CRPC - M1 | IV each 3 weeks | Yes | Yes | 2.9 months( |
| Cabazitaxel | CRPC - M1 After docetaxel | IV each 3 weeks | Yes | Yes | 2.4 months( |
| Abiraterone acetate | CRPC - M1 before or after Docetaxel | Oral Daily | Yes | Yes | Before Docetaxel: 5.2 months( |
| Enzalutamide | CRPC - M0/M1 before or after Docetaxel | Oral Daily | No | Yes | M0: immature( Before Docetaxel: 4.0 months( After Docetaxel: 4.8 months( |
| Sipuleucel-T | CRPC - M1 before or after Docetaxel | IV each 2 weeks | No | No | 4.1 months( |
| Radium-223 | CRPC - M1 before or after Docetaxel | IV each 4 weeks | No | Uninformed | 3.6 months( |
| Apalutamide | CRPC - M0 | Oral Daily | No | Yes | M0 immature( |
| Darolutamide | CPEC - M0 | Oral twice Daily | No | Yes | M0 immature( |
Not available in Brazil.
With a median follow-up of 13.7 months, this study showed an improvement in OS (15.1 vs 12.7 months, HR = 0.70, 95% CI 0.59-0.83, p < 0.0001) and in progression-free survival (PFS) (2.8 vs 1.4 months, HR = 0.74, 95% CI 0.64-0.86, p = 0.0002) for those treated with C+P.(
Due mainly to hematological toxicity, the non-inferiority phase 3 PROSELICA trial evaluated the efficacy of cabazitaxel in a lower dose. In this study, 1200 patients with mCRPC who failed docetaxel were randomized to cabazitaxel 25mg/m2 (C25) every 3 weeks or to cabazitaxel 20mg/m2 (C20) every 3 weeks and no inferiority was demonstrated in OS or PFS at lower dose. In addition, grade 3 and 4 AE (39.5% C20 vs 54.5% C25), grade 4 neutropenia (21.3% C20 vs 48.6% C25) and neutropenic infection (2.2% C20 vs 6.1% C25) were less frequent at the lower dose.(
Therefore, cabazitaxel at a dose of 20mg/m2 every 3 weeks is one of the options for second-line mCPRC (after docetaxel failure) treatment.
Abiraterone acetate is a hormonal agent that inhibits androgen biosynthesis through inactivation of the CYP-17 enzyme, acting in the three sources of androgen production: testis, adrenal gland and intra-tumor. Its activity was demonstrated in mCRPC as first line treatment and as second line (after docetaxel failure).
The phase 3 COU-AA 302 trial randomized 1088 chemotherapy-naïve mCRPC patients, asymptomatic or oligosymptomatic, to abiraterone 1g/day and prednisone 10mg/day or to placebo and prednisone 10mg/ day. A follow-up of 49 months showed improvement of OS (34.7 vs 30.3 months, HR = 0.81, p = 0.003) and rPFS (16.5 vs 8.2 months, HR = 0.52, p < 0.0001) for the abiraterone group. However, 44% of patients in the placebo group received abiraterone later, which may have influenced the magnitude of the results.(
The COU-AA 301 phase 3 trial randomized 1195 mCRPC patients who failed to docetaxel to abiraterone 1g/day and prednisone 10g/day or placebo and prednisone 10mg/day. With a 20 months median follow-up an improvement in OS was demonstrated (15.8 vs 11.2 months, HR = 0.74, p < 0.001) for the abiraterone group. This group had also benefit in all secondary outcomes (time to PSA progression, rPFS, PSA response).(
In general, toxicity of abiraterone is related to the excess of mineralocorticoids, so the concomitant use of prednisone is necessary. Water retention (33%), hypertension (11%) and hypokalemia (18%) are among the most frequent AE. Other AE observed are changes in liver function tests (11%) and miscellaneous cardiac disorders (16%). Despite the toxicity mentioned above, the rate of discontinuation of treatment related to AE was similar to that of the placebo group.(
Thus, abiraterone 1g/day and prednisone 10mg/day is an option for mCRPC either in the first or second line treatment (after docetaxel).
Enzalutamide is a strong AR blocker, thus, it acts directly by blocking the AR, preventing nuclear translocation of the AR and inhibiting the binding of the receptor to the nucleus DNA. Its efficacy in mCRPC was demonstrated in M0 and M1 disease setting, in both chemotherapy-naïve patients and in those who failed to docetaxel. Three important phase 3 trials evaluated enzalutamide in mCRPC setting. Two trials evaluated enzalutamide in metastatic castration-resistant prostate cancer patients (M1CRPC) and one trial included only non-metastatic castration-resistant prostate cancer patients (M0CPRC) with highrisk disease (rapidly rising PSA).
The PREVAIL trial randomized 1717 chemotherapy-naïve mCRPC patients, asymptomatic or oligosymptomatic, to enzalutamide 160mg/day or placebo. With a median follow-up of 22 months it was shown improvement in OS (34.7 vs 30.2 months, HR = 0.71, p < 0.001) and in secondary outcomes (rPFS and reduction of skeletal events) for the enzalutamide group. In addition, there was also a significant improvement in QoL for the enzalutamide group.(
The most common AE related to enzalutamide are fatigue (34%), hot flashes (20%) and diarrhea (21%). In the AFFIRM trial some patients that received enzalutamide presented seizures and, due to this, those with a past of seizures and/or recent brain event were excluded from the PREVAIL trial.(
Thus, enzalutamide 160 mg/day is an option for M0CRPC high-risk disease treatment and for M1CRPC first and second line treatment.
Sipuleucel-T is an autologous vaccine of dendritic cells developed to increase T cell-mediated immune response against prostatic acid phosphatase. Its activity in mCRPC was demonstrated in the phase 3 IMPACT trial. This trial randomized 512 mCRPC patients (asymptomatic or oligosymptomatic, previously treated with docetaxel or not) to sipuleucel-T every 2 weeks for 3 cycles or placebo. With a median follow-up of 34 months it was showed an OS improvement (25.8 vs 21.7 months, HR = 0.78, p = 0.03) for the vaccine group. However, neither improvement in PFS nor in PSA response rate was observed.(
This therapy is well tolerated and, as in other immunotherapies, the most common vaccine-related AE were chills (53%), fatigue (41%), and fever (35%).(
Therefore, sipuleucel-T is an option of for mCRPC, but it is not available outside the USA.
Radium-223 is an a-particle emitter therapeutic agent which has tropism for bone tissue. It is able to achieve bone metastases with high energy in a small radius of action, minimizing toxicity in the bone marrow.
The phase 3 ALSYMPCA trial randomized 921 mCRPC patients previously treated or not with docetaxel, symptomatic and with bone metastases only (no known visceral metastases) to receive radium-223 every 4 weeks up to six cycles or placebo. This trial demonstrated an improvement in OS for those treated with radium-223 as first or second line of treatment (14.9 vs 11.3 months, HR = 0.70, p < 0.001). Treatment was well tolerated and there was no significant difference in grade 3 or 4 toxicity when compared with the control group.(
Thus, radium-223 is another option of treatment - as first or second line (after docetaxel) - for mCRPC with bone metastases.
The systemic treatment of patients who are castrate resistant and have not still developed metastatic disease have been recently studied. In the era of Gallium-68 prostate-specific membrane antigen (PSMA) positron emission tomography (PET), which has a higher sensitivity and specificity in identifying metastatic disease, this scenario in progressively less common in clinical practice.(
The use of enzalutamide was compared to placebo in the PROSPER trial. This trial enrolled 1401 men with a PSA doubling time of =10 months and a serum PSA = 2 ng/mL. Metastasis-free survival (MFS) - the primary endpoint- was longer with enzalutamide (39.6 vs 14.7 months, HR = 0.29, 95% CI: 0.24-0.35, p < 0.001). Time to first use of a new antineoplastic agent and time to PSA progression (39.6 vs 17.7 months, HR = 0.21, 95% CI: 0.17-0.26, p < 0.001 and 37.2 vs 3.9 months, HR = 0.07, 95% CI: 0.05-0.08, p < 0.001, respectively) have also favored the use of enzalutamide.(
Apalutamide is a nonsteroidal antiandrogen agent that binds directly to the ligand- binding domain of the AR and prevents AR translocation, DNA binding, and AR mediated transcription.(
Recently, darolutamide, another antiandrogen, has been tested in the same clinical scenario (ARAMIS study). This double blind, placebo-controlled phase III trial randomized 1,509 patients in a 2:1 ratio. Patients were stratified by PSA doubling time (= 6 months or > 6 months) and use of osteoclast-targeted therapy. Median MFS was 40.4 months with darolutamide vs 18.4 months with placebo (HR 0.41; 95% CI 0.34-0.50; p < 0.0001). In addition, there was a trend favoring darolutamide in terms of OS (Median not reached for either arm, HR 0.71, 95% CI 0.500.99, p = 0.045).(
Advances in treatment of mCRPC and availability of new therapeutic agents are notorious, but many questions related to optimal sequencing or the comparison of efficacy between these new agents remain unanswered. Until then, there are no randomized studies comparing directly the agents of different classes.
Recent data suggest that regardless of the line of treatment and its sequence, patients who are exposed to as many agents as possible have improvement in OS.(
Thus, the search and identification of predictive biomarkers of response would be one of the tools to select the best agent and/or the best time to use it. In this scenario, several studies have evaluated the identification of androgen receptor variants (AR-V) as a possible biomarker. It is known that the presence of AR-V is one of the mechanisms of resistance to castration, since it gives the AR constant activity without requiring stimulation for circulating androgens.
Several variants of the AR have been identified, but the most common and best characterized is variant 7 (AR-V7).(
In another retrospective study, 37 patients with CPRC were treated with taxanes and the presence of AR-V7 in CTC was identified in 46% of them. Unlike the study with enzalutamide and abiraterone, the presence of AR-V7 did not interfere with the rate of PSA response with chemotherapy.(
Despite these results, it is worth mentioning that these are retrospective studies with small number of patients, and it is necessary to await the results of prospective studies in progress that can define AR-V7 as a predictive or only prognostic factor.
A recent prospective study involved 202 patients that received either enzalutamide or abiraterone. The patients were submitted to an analysis of the RNA of CTC to verify quantification of androgen AR and to examine the prognostic value of this data. Patients with high amounts of receptors correlated with the presence of variant 7 (AR-V7). In addition, the number of copies of the AR showed a prognostic value in patients treated with abiraterone or enzalutamide: the higher the number of copies, the lower PFS (laboratory, radiological and clinical) and the lower OS.(
In the absence of randomized studies comparing the agents and the lack of predictive biomarkers, the tools for choosing the first or second line of treatment are the clinical features of each patient. It is important to consider the performance status of the patient, comorbidities and symptoms, clinical-pathological characteristics of the disease as extension of metastatic disease, presence of undifferentiated or small cell components and toxicity profile of each agent. In addition, patient's preference (intravenous or oral), cost and availability of the agents should be taken into account.
Retrospective studies suggest a relationship between the time of exposure to the initial hormone therapy and the activity of the hormonal agents in the castration-resistant setting. In this context, lower exposure (< 16 months vs = 16 months) or the short-lived response (< 12 months vs = 12 months) to the initial hormone therapy is associated with a greater probability of not responding to subsequent treatment with abiraterone or enzalutamide.(
Gleason score is a prognostic factor established in localized disease.(
Undifferentiated tumors or tumors with small cell components are rare, aggressive, more common in young patients, and usually with low PSA regardless of the volume of metastatic disease.(
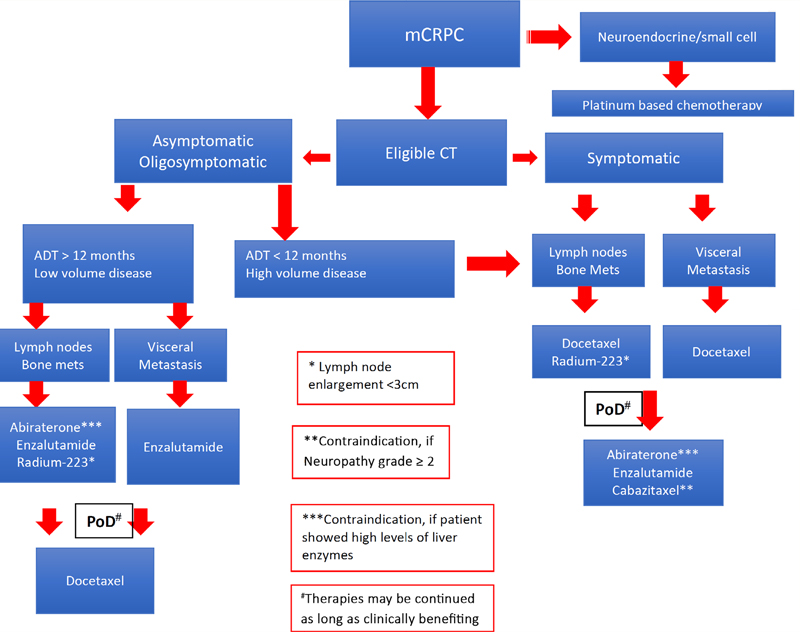
The options for first-line mCRPC treatment available in Brazil, the inclusion criteria, as well as the most common adverse effects are summarized in
Unlike TAX 327 and ALSYMPCA trials, in which 45% and 100% of the patients, respectively, were symptomatic, in PREVAIL and COU-AA 302 trials the symptomatic patients were excluded. Patients with visceral metastasis were excluded of COU-AA 302 and ALSYMPCA trials, but represented 11% of PREVAIL trial patients and 22% of TAX 327 trial patients.(
Recently, a prospective multicenter phase 3b trial of 839 mCRPC patients evaluated Radium-223 in some different scenarios of the ALSYMPCA trial. In this trial, 20% of the patients were asymptomatic and Abiraterone (18%) or Enzalutamide (5%) were allowed to be used associated with Radium-223. Subgroup analysis according to the symptomatology and level of alkaline phosphatase demonstrated a greater OS for asymptomatic patients and for those with alkaline phosphatase levels within normality.(
The improvement of OS in these subgroups raises the question whether this benefit occurs from the early onset of Radium-223 (at the earliest stage of the metastatic disease) or from the more indolent and less aggressive disease.
As previously discussed, due to seizures in some patients that received enzalutamide after prior therapy with docetaxel (AFFIRM trial), those with a historic of seizures or some recent brain event (e.g. stroke) were also excluded from the PREVAIL trial.(
Recent data from patients in a phase 2 trial evaluating the sequence of first-line treatment with abiraterone and enzalutamide in mCRPC showed a worsening of depressive symptoms and an increase of cognitive impairment in those treated with enzalutamide.(
Unlike docetaxel and abiraterone, the use of enzalutamide and radium-223 does not require association with corticosteroids. Some retrospective series suggest that there is no negative impact on the efficacy and safety of abiraterone when used with a lower dose of corticosteroid (prednisone 5 mg/day), as well as the lower incidence of side effects related to prolonged corticoid use.(
|
| Docetaxel (TAX 327)( | Abiraterone (COU-AA 302)( | Enzalutamide (PREVAIL)( | Radium-223 (ALSYMPCA)( |
|---|---|---|---|---|
| Asymptomatic or oligosymptomatic | Yes | Yes | Yes | No |
| Symptomatic | Yes | No | No | Yes |
| Visceral Metastasis | Yes | No | Yes | No |
| = 2 bone metastases | Yes | Yes | Yes | Yes |
| Performance Status | KPS = 60 | ECOG 0/1 | ECOG 0/1 | ECOG 0/2 |
| Seizure | Yes | Yes | No | No |
| Significant cardiac dysfunction | No | No (EF = 50) | No (EF = 45) | No |
| Resistant hypertension | Yes | No | No | No |
| Specific adverse effects | Neutropenia Neuropathy Fatigue Diarrhea | Edema Hypertension Hypokalemia Elevation of hepatic enzymes Cardiac events | Fatigue Hot flashes Hypertension Cardiac events Seizure | Thrombocytopenia Diarrhea |
Recently docetaxel and cabazitaxel were compared in first-line treatment. The FIRSTANA trial randomized 1168 mCRPC patients to receive cabazitaxel 20mg/m2 or cabazitaxel 25mg/m2 or docetaxel 75mg/m2 as first line treatment. Despite the higher response rate with Cabazitaxel 25mg/m2, there was no difference in OS (24.5 vs 25.2 vs 24.3 months, p = 0.99). The AE and the discontinuation rate of the treatments were similar.(
Currently there is another possible setting for the second-line treatment: those patients who received chemohormonal as first-line treatment in the mCSPC setting. There was no standard treatment for those patients.
A retrospective analysis of the GETUG-AFU 15 trial demonstrated a PSA response rate of 13-70% and symptom improvement in 16-33% of patients when exposed to other agents following progression.(
The second line treatment options available in Brazil, some details of each trials and the most common AE associated with these therapies are specified in
To this moment there are no studies comparing these second line therapies or evaluating their use in sequence. Therefore, the data and results of the main phase 3 trials and some retrospective analysis of the action of these drugs when used in sequence should be of great help when choosing the most appropriate treatment.
| GETUG-AFU 15( | CHAARTED( | STAMPEDE( | ||||
|---|---|---|---|---|---|---|
| HT (193) | CT+HT (192) | HT (393) | CT+HT (397) | HT (1184) | CT+HT (592) | |
| Progression | 287 | 238 | 761 | 315 | ||
| Treatment | 42% | 68% | 55% | 88% | 83% |
|
| Docetaxel | 40% | 15% | 51% | 23% | 41% | 14% |
| Cabazitaxel | 1% | 2% | 13% | 26% | 3% | 7% |
| Abiraterone/Enzalutamide | 11% | 12% | 38% | 47% | 23%/9% | 28%/8% |
CT: chemotherapy, HT: hormone therapy.
|
| Cabazitaxel( | Abiraterone( | Enzalutamide( | Radium-223( |
|---|---|---|---|---|
| Symptomatic | Yes | Yes | Yes | Yes |
| Metastasis | Bone: 84% Viscera: 24% | Bone: 89% Lymph node: 44% Liver: 10% | Bone: 92% Lymph node: 55% Lung: 15% Liver: 11% | Bone: 100% |
| Performance Status | ECOG 0/2 | ECOG 0/2 | ECOG 0/2 | ECOG 0/2 |
| Neuropathy Grade = 2 | No | No | No | No |
| Significant cardiac dysfunction | No (EF = 50) | No (EF = 50) | No (EF = 45) | --------- |
| Corticosteroids | Yes | Yes | No | No |
| Control Arm | Mitoxantrone | Placebo + Prednisone | Placebo | Placebo |
| Specific adverse events | Neutropenia Fatigue Diarrhea | Edema Hypertension Hypokalemia AST/ALT rising Cardiac alterations | Fatigue Hot flushes Hypertension Cardiac alterations Seizure | Thrombocytopenia Diarrhea Vomiting |
Considering the control arms of each clinical trial in second line treatment after failure to docetaxel, placebo plus prednisone and placebo alone where used as controls arms in the COU-AA-301 and AFFIRM trials respectively. In the other hand, the TROPIC trial control group received mitoxantrone, a chemotherapy with known palliative action in pain control and PSA response rate, however with no improvement in OS.(
The secondary endpoints of the trials were different. While COU-AA-301 and AFFIRM trials considered disease progression as evidence of tumor progression radiologically, the TROPIC trial defined disease progression as rise in PSA, evidence of tumor progression radiologically or worsening of the pain. Thus, treatment in the TROPIC trial may have been discontinued sooner in comparison to treatment in the COU-AA-301 and AFFIRM trial, therefore resulting in a shorter duration of treatment.
The TROPIC, COU-AA-301 and AFFIRM trial enrolled patients that progressed after treatment with docetaxel. In this context, 63% of the patients enrolled in the TROPIC trial and 45% of the patients in the COU-AA-301 had discontinued the treatment with docetaxel due to progression.(
At the same time that in the COU-AA-301 and AFFIRM trials the OS benefit was seen in patients regardless of age (= 65 vs < 65yrs), in the TROPIC trial there was no difference in OS in patients under 65 yrs. old.(
All secondary endpoints were positive in the three trials. Time to the first skeletal event was longer in the COU-AA-301 and AFFIRM trial, however this endpoint was not evaluated in the TROPIC trial.(
The median duration of treatment was 8 and 8.3 months for the COU-AA-301 and AFFIRM trials, respectively. Patients in the TROPIC trial received a median of six treatment cycles. The cross-over was allowed in the COU-AA-301 and AFFIRM trials and not allowed in the TROPIC trial.(
The toxicity related to each treatment has been discussed previously. It is important to emphasize that, being chemotherapy, the hematological toxicity observed in the TROPIC trial may be a limiting factor for treatment with cabazitaxel. Regarding enzalutamide, as previously discussed, historic of seizures could be a contraindication.(
There is no good level evidence for the best sequence treatment to mCRPC in this setting. Retrospective data suggest lower response rates when abiraterone and enzalutamide are used in sequence, indicating perhaps the existence of a cross-resistance mechanism between them(
Recently, exploring the sequencing of these two agents, a phase 2 trial with 202 M1CRPC patients evaluated abiraterone plus prednisone followed by enzalutamide (arm A) versus enzalutamide followed by abiraterone plus prednisone (arm B), both at PSA progression. The primary endpoints, PSA decline > 50% on second line therapy and time to second PSA progression, were better with arm A sequence (34 vs 4% and 2.7 vs 1.3 months, respectively).(
Although docetaxel was the main second line treatment in patients after disease progression on COUAA-302 (44% of the abiraterone and 58% of the placebo group receive some second line treatment)(
Retrospective data from patients treated with docetaxel after abiraterone demonstrated an OS of 12.5 months, lower than the 19.2 months showed by the TAX 327 trial, which might suggest the hypothesis of some degree of cross-resistance between the agents.(
Given the limitations of these retrospective data, it can also be inferred that docetaxel maintains its activity after previous use of abiraterone.
However, the response or non-response to previous treatment with abiraterone or enzalutamide does not seem to be a predictive factor for response to cabazitaxel.(
Although a considerable number of patients have good clinical conditions to receive some treatment in this setting, there is no standard recommendation. In the absence of randomized clinical trials, some small retrospective series summarized in
|
| N | Response PSA > 50% | OS (mo) | ||
|---|---|---|---|---|---|
| Abiraterone?Docetaxel |
|
|
| ||
| De Bono et al.( | 265 | 47% | NI | ||
| Mezynski et al.( | 35 | 26% | 12.5 | ||
| Schweizer et al.( | 24 | 38% | NI | ||
| Aggarwal et al.( | 23 | 48% | 12.4 | ||
| Azad et al.( | 86 | 35% | 11.4 | ||
| Abiraterone?Enzalutamide |
|
|
| ||
| Azad et al.( | 47 | 25.5% | 8.6 | ||
| Suzman et al.( | 30 | 34% | NI | ||
| Cheng et al.( | 28 | 36% | NI | ||
| Docetaxel?Abiraterone?Enzalutamide |
|
| |||
|---|---|---|---|---|---|
| Authors | N | PSA response | OS | ||
| Schrader et al.( | 35 | 29% | 7.1 | ||
| Bianchini et al.( | 39 | 13% | NI | ||
| Badrising et al.( | 61 | 21% | 7.3 | ||
| Azad et al.( | 68 | 22% | 10.6 | ||
| Docetaxel?Enzalutamide?Abiraterone |
|
| |||
| Authors | N | PSA response | OS | ||
| Loriot et al.( | 38 | 8% | 7.2 | ||
| Noonan et al.( | 30 | 3% | 11.6 | ||
| Docetaxel?Abiraterone or Enzalutamide?Cabazitaxel |
|
| |||
| Authors | N | PSA response | OS | ||
| Pezaro et al.( | 41 | 39% | 15.8 | ||
| Sella et al.( | 24 | 32% | 8.2 | ||
| Wissing et al.( | 69 | 32% | NI | ||
| Al Nakouzi et al.( | 79 | 35% | 10.9 | ||
Given the proven efficacy of immunotherapy in several solid tumors (lung and kidney cancer, melanoma, etc.), this treatment strategy has also been evaluated in mCRPC. Ipilimumab, a humanized anti-CTL-4 monoclonal antibody, was evaluated in two phase 3 trials. In the first trial 799 patients with mCRPC and at least one bone metastasis who had failed to docetaxel were randomized to receive bone-directed radiotherapy followed by either ipilimumab 10mg/kg or placebo every 3 weeks up to four doses. After median follow-up of 9.9 months there was no difference in OS (11.2 vs 10 months, HR = 0.85, 95% CI: 0.72-1.00, p = 0.053).(
Pembrolizumab, a highly selective anti PD-1 humanized monoclonal antibody, demonstrated durable responses in 23 patients with mCRPC whose tumors have PD-L1 expression = 1 percent in a non-randomized phase 1b trial.(
The activity combining immunotherapy was evaluated in a recent phase 2 trial with 78 asymptomatic or minimally symptomatic mCRPC patients who progressed after new generation hormone therapy and not received chemotherapy (cohort 1) or had received chemotherapy (cohort). The combination was nivolumab 1mg/Kg + ipilimumab 3mg/Kg every 3 weeks for 4 doses then nivolumab 480mg every 4 weeks. The primary endpoint ORR was 26 and 10% in cohort 1 e 2, respectively. In both cohorts the ORR was higher in patients with PD-L1 = 1% and DNA damage repair (DDR).(
It has been know that mCRPC can harbor some DNA repair gene mutation like BRCA1 or 2, ATM, CHEK2, NBN and PALB2 that may be associated with more aggressive disease and poorer OS.(
Another phase 2 trial randomized 142 mCRPC patients who have failed to prior chemotherapy to olaparib and abiraterone or abiraterone. With a median follow-up of 15.9 months the rPFS was higher for olaparibe and abiraterone (13.8 vs 8.2 months, HR = 0.65, 95% CI:0.44-0.97, p = 0.034). In contrast, more AE were observed in combination treatment arm.(
Recently the activity combining Pembrolizumab and Olaparib in heavily treated mCRPC was evaluated in one cohort of KEYNOTE-365 phase 1b/2 trial with 40 patients that showed PSA response rate and ORR of 13 and 7%, respectively.(
Currently there are several options for the treatment of metastatic prostate cancer, with different mechanisms of action, toxicities, routes of administration, and costs. Importantly, all approved agents have shown improvement in OS. However, no headto-head comparisons are available. Several efforts have been done in order to answer that question. An international retrospective epidemiologic trial of men with advanced prostate cancer (IRONMAN Trial) is ongoing collecting clinical information about this patients around the world. In addition, biological specimens have been collected to correlate clinical findings with biological characteristics. Hopefully, this registry which will include more than 5.000 patients may help us to answer those open questions.
Advances in the understanding of tumor biology have also influencing in the development of new therapeutic strategies and biomarkers of prognosis or response to available therapies. Unfortunately, no biomarkers have been validated to be used in the clinical practice. Therefore, treatment should be individualized taking into account clinical factors such as age, performance status and comorbidities; disease clinical course PSA doubling time, symptoms or not; and pathological features: Gleason score at diagnosis, neuroendocrine component. Another important factor in the decision making process is the toxicity profile of each agent that may vary according to each agent. In addition, especially in developing countries where resources and access to medications are restricted, cost should be taken in consideration.
In spite of the provocative and promising results with AR-V7, there is still no validation of it as a predictive factor and results from prospective studies are awaited, thus, testing for AR-V7 should not yet be used to guide decisions on treatment.
Considering that all agents are equally effective, practical issues such as availability, access and cost of the agents, besides the preference of patients may be decisive when choosing the agent.
Based on all the prospective and retrospective data already mentioned, the suggestion is that for the majority of PCRC patients, hormonal treatment with abiraterone or enzalutamide should be initially offered, reserving chemotherapy in the case of clinical conditions, for symptomatic patients, with visceral disease, with an undifferentiated component/small cells in the pathology and/or those with progression after a short time of hormonal blockade (signal suggestive of resistance to hormonal therapy).
Retrospective data and post-hoc analyzes suggest that, if the patient has the clinical conditions, chemotherapy is the preferred option after failure to abiraterone or enzalutamide.
New discoveries are accompanied by new possibilities, however, the questions and doubts are increasing. In this manner, we await for the results of the prospective studies in progress evaluating these new agents directly and in earlier stages of the disease, as well as for the evaluation of biomarkers, so that we can understand in which patient and which moment of the disease to better use them.
Flowchart 1.
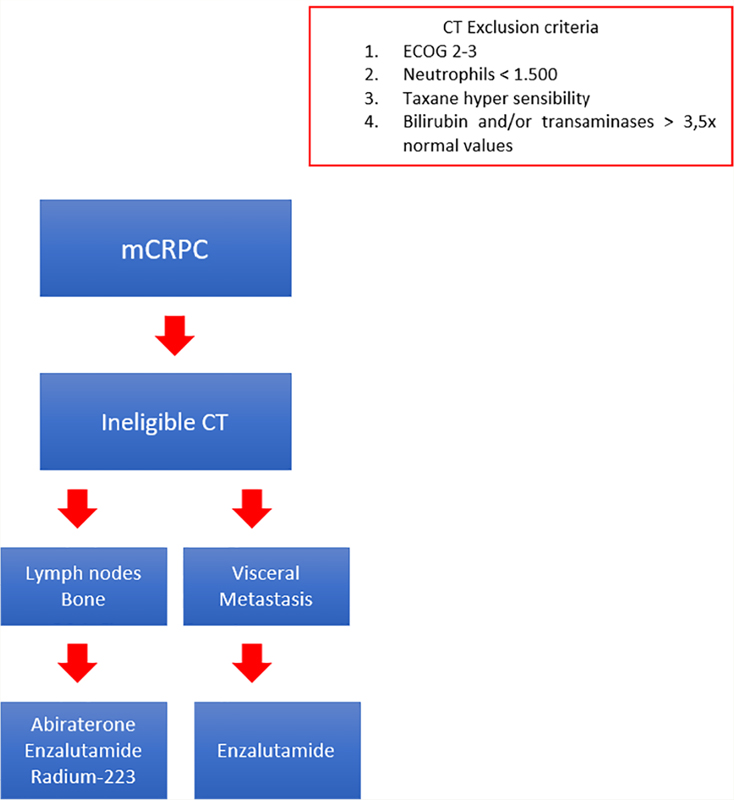
Flowchart 2.
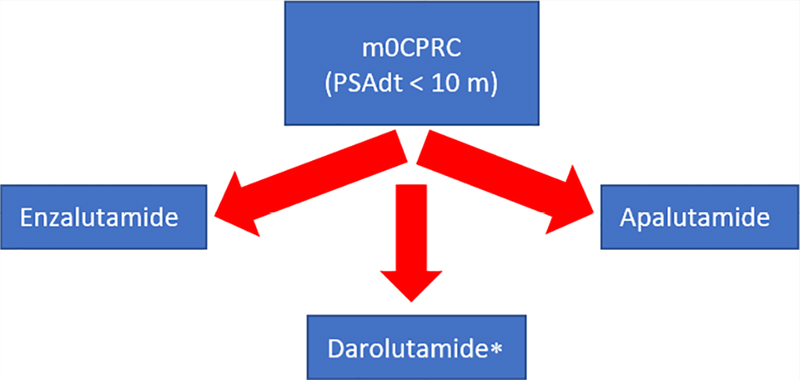
Flowchart 3.
* Not available in Brazil.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.