According to the World Health Organization, colorectal cancer (CRC) is the third most common cancer worldwide. In 2018, approximately 1.8 million people were diagnosed with this tumor type.
CRC originates from the epithelial tissue of the colon, and it may arise either from the right or left the side of the colon, where the splenic flexure is the dividing point. They exhibit differences in blood supply, embryologic development, clinicopathologic characteristics and anatomic features.
Retrospective analyses from two pivotal first-line phase III studies, comparing chemotherapy (CT) (FOLFIRI or FOLFOX) plus cetuximab versus CT plus bevacizumab, reported improved overall survival (OS) in the cetuximab group for left-sided wildtype (wt) RAS mCRC.
Despite those recommendations, little is known whether such international recommendations have influenced clinical practice in Brazil. The Brazilian Gastrointestinal Tumors Group (GTG) is the leading gastrointestinal (GI) cancer society in the country and has the objective of assisting, promoting, developing and encouraging scientific, technological, cultural, educational and social actions aimed essentially at improving the knowledge of GI tumors and related medical sciences. This survey was created by GTG to understand the first line choices of Brazilian oncologists for patients with unresectable mCRC, especially in the emergent context of tumor sidedness and RAS / BRAF V600E status. We also aim at exploring differences in therapeutic choices by oncologists according to gender, years in practice and time dedicated to GI practice.
This was a cross-sectional electronic survey composed of six close-ended questions, which was sent to Brazilian medical oncologists and medical oncology groups by social medias such as email, Facebook and/or Whatsapp. The target survey population was medical oncologists who were members of GTG and those working in leading institutions in Brazil that offer cancer treatments. The contact to invite the participation was conducted by the GTG board of directors. The electronic survey was sent to all potential candidates twice within 30 days. The consent to participate in this study was obtained by the acceptance to complete the questionnaire, which guaranteed that all participants' data would be treated anonymously. Given that this was a survey on treatment practices, the study was not submitted to an ethics committee.
The survey instrument assessed current practices in terms of first-line treatment choices for fit patients with mCRC, including left-sided wt- RAS /wt- BRAF V600E , right-sided wt- RAS /wt- BRAF V600E and any-side mutated RAS, considering that all drugs were available. The instrument also elicited data about years in practice in Medical Oncology, gender and how much of each oncologists' practice was dedicated to GI cancers. Those with at least 50% of their clinical practice dedicated to patients with GI malignancies were considered specialists. The time estimated to complete the survey was between two to four minutes. The study was funded by the GTG.
The online questionnaire was developed using the Survey Monkey platform. Only fully completed questionnaires were included in the analyses. Descriptive statistics were reported for all responses. Subgroup comparisons were analyzed with ?
The survey was completed during a 30-day period (February 20th, 2018 to March 21st, 2018) by 239 medical oncologists who agreed to participate from across the country. Because the survey was not sent to all individual emails, we could not estimate the response rate but for those who responded, the completion rate was 100%.
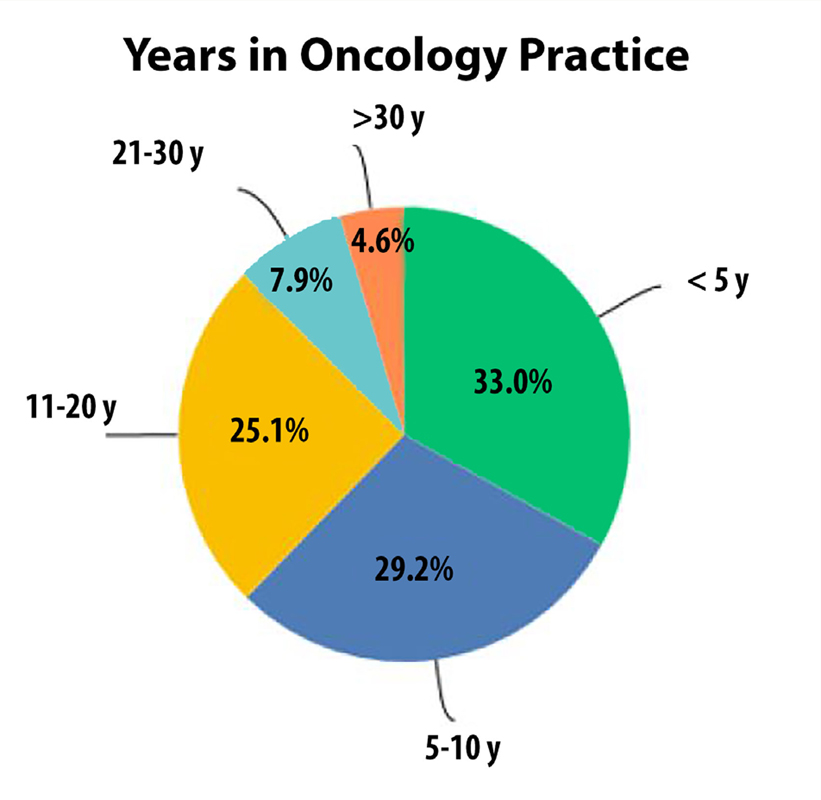
The majority of respondents were male (59%) and were in oncology practice for less than 10 years (62.2%) (
Only 20.9% of the participants were specialists in GI tumors while 30.5% treated GI cancer patients for less than 25% of their practice. In regards to proportion of time dedicated to treat GI cancers, there was neither difference between males and females ( p= 0.872) nor according to years of oncology practice ( p= 0.766).
Figure 1 Distribution of oncologists according to years in oncology practice.
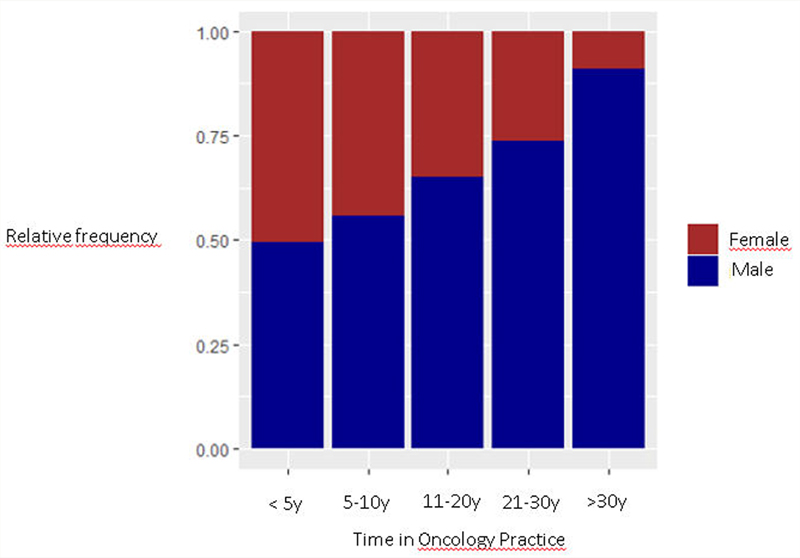
Figure 2 Gender proportion according to time in oncology practice.
For left-sided wt- RAS/ wt- BRAFV600E mCRC, most oncologists (82%) chose first line CT + anti-EGFR therapy, with 53.6% of them preferring FOLFIRI and 46.4% FOLFOX as the CT backbone (
Meanwhile, for right-sided, wt- RAS/ wt- BRAFV600E mCRC, the majority (70.7%) would offer CT + bevacizumab (53.9% of them with FOLFOX, 31.9% with FOLFIRI and 14.5% with FOLFOXIRI) (
In the case of a mutated -RAS mCRC, most oncologists decided for FOLFOX + bevacizumab (51.9%) while 33.3% chose FOLFIRI + bevacizumab and 14.1% FOLFOXIRI + bevacizumab (
There was no statistically difference in treatment choices (CT backbone and monoclonal antibody) for left-sided or right-sided wt- RAS/ wt- BRAFV600E mCRC according to years in oncology practice. However, for patients with mutated- RAS mCRC, oncologists with more than 10 years of practice preferred more FOLFOX + bevacizumab than FOLFIRI or FOLFOXIRI + bevacizumab when compared to younger oncologists ( p= 0.04).
For left-sided, wt- RAS/ wt- BRAFV600E mCRC, there was a statistically significant difference in terms of gender and treatment choices ( p= 0.004). For instance, most female oncologists would choose FOLFOX + anti-EGFR therapy while most male oncologists would prefer FOLFIRI + anti-EGFR. For right-sided wt- RAS/ wt- BRAFV600E or mutated -RAS mCRC, there was no difference in treatment choices according to gender ( p= 0.096 and p= 0.208, respectively).
In terms of time dedicated t o GI practice, a statistically significant difference was seen in the right-sided wt- RAS/ wt- BRAFV600E mCRC group ( p= 0.001). Ninety-four percent of oncologists with more than 50% of their practice dedicated to GI cancers would choose bevacizumab as monoclonal antibody while only 64.6% of the nonGI specialists would prefer bevacizumab. In addition, 18% of the GI specialists would choose FOLFOXIRI + bevacizumab in this scenario whereas only 7.9% of the non-GI specialists would prefer it. For left-sided wt- RAS/ wt BRAFV600E or mutated -RAS mCRC, there was no difference in treatment choices according to time dedicated to treat GI cancers ( p= 0.429 and p= 0.433, respectively).
|
| left-sided wtRAS/wt-BRAF | right-sided wtRAS/wt-BRAF | mtRAS |
|---|---|---|---|
| FOLFIRI + bevacizumab | 10 (4.2%) | 54 (22.6%) | 79 (33.1%) |
| FOLFIRI + cetuximab/panitumumab | 105 (43.9%) | 26 (10.9%) | --------------------- |
| FOLFOX + bevacizumab | 26 (10.9%) | 91 (38.1%) | 123 (51.5%) |
| FOLFOX + cetuximab/panitumumab | 91 (38.1%) | 44 (18.4%) | --------------------- |
| FOLFOXIRI + bevacizumab | 7 (2.9%) | 24 (10.0%) | 35 (14.6%) |
| Did not answer | 0 | 0 | 2 (0.8%) |
| Total | 239 (100%) | 239 (100%) | 239 (100%) |
Tumor sidedness and RAS/BRAF status have modified the treatment landscape of mCRC worldwide in the last years, although the true impact of those changes in third-world countries remains undetermined. Brazil is the 5th largest country and presents accentuated heterogeneity which affects cancer care delivery. This is the first Brazilian survey to try to determine oncologists' first-line treatment decisions for mCRC, according to sidedness and RAS/ BRAF V600E status and considering that all therapeutic choices were available in 2018.
Our study revealed interesting findings. First, it clearly showed a significant increase of women oncologists' proportion over time. While females corresponded to less than 10% of oncologists with more than 30 years of practice, more than half of those with less than 5 years of practice are women. These findings are in parallel with the growing presence of women in Brazilian medicine. The feminization of medicine in Brazil in the past decades has already been described.
Other important finding was the difference in the choice of monoclonal antibody for right-sided wt RAS/ wt- BRAFV600E mCRC according to time dedicated to GI cancers, where 94% of GI specialists chose bevacizumab and only 64.6% of non-GI specialists preferred bevacizumab. Several data have been accumulating over the past years showing better outcomes with bevacizumab + CT in right-sided wt- RAS/ wt- BRAFV600E mCRC, in contrast to anti-EGFR therapy + CT in the left-sided wt- RAS/ wt- BRAFV600E mCRC.
Those answers reveal us that the more specialist an oncologist is in an area, the more in accordance with data he or she will be. The larger proportion of non-GI specialists indicating first-line CT + anti- EGFR for rightsided wt- RAS/ wt- BRAFV600E mCRC may be explained in part by lack of familiarity with current guidelines in GI cancers. While the relationship between surgeon volume and outcomes has long been well established for complex cancer surgeries, the impact of oncologists' experience on outcomes for patients with metastatic tumors is unknown.
Our study has several limitations. First, the questionnaire did not distinguish between academic and community-based physicians, nor did it capture whether responders worked in the public, private or both systems. We have also not captured whether the oncologist worked in outpatient clinics or hospitals, which could influence treatment choices, especially the fear of prescribing FOLFOXIRI where access to granulocyte-colony stimulating factors or hospital admissions is limited. Moreover, the real practice in terms of CT backbone and monoclonal antibodies' choices could not be determined as the questionnaire expected the responders to answer in a scenario where all drugs were available, which is not the case in all areas and medical services in Brazil. In addition, the extent of non-responders was not captured, which may limit the generalizability of our findings.
In conclusion, our survey indicates that tumor sidedness influences the choice of both CT backbone and monoclonal antibody in unresectable wt- RAS mCRC. In addition, oncologists' gender and percentage of time dedicated to treat GI cancers also impact therapeutic choices for mCRC in Brazil. We believe that the first educational task as a group is to ensure that oncologists who see patients with mCRC are practicing in accordance with literature recommendations.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.