Several novel cancer treatments have received global approval in recent years. However, there are many barriers to rapid access to new drugs, which can occur at various stages of the approval process: during research, at regulatory agencies, in cost-effectiveness and pricing analysis, or during implementation into local practice.
Cancer is a medical condition that is often associated with relatively short survival durations and significantly high mortality rates. In an effort to enable faster access to treatments that may offer meaningful clinical benefits, a variety of intermediate outcomes—such as disease-free survival, event-free survival, progression-free survival, and objective response rates—are being increasingly utilized in both clinical and regulatory decision-making processes. Nevertheless, while these surrogate endpoints can provide useful early indications of treatment efficacy, they can also become subjects of debate, particularly when used in cost-effectiveness evaluations and reimbursement-making decisions.
According to the Global Cancer Observatory (GLOBOCAN), the global cancer burden is expected to rise to 29.9 million cases by 2040, a 49% increase from 2022, with a more significant increase in transitioning countries compared to those already transitioned.
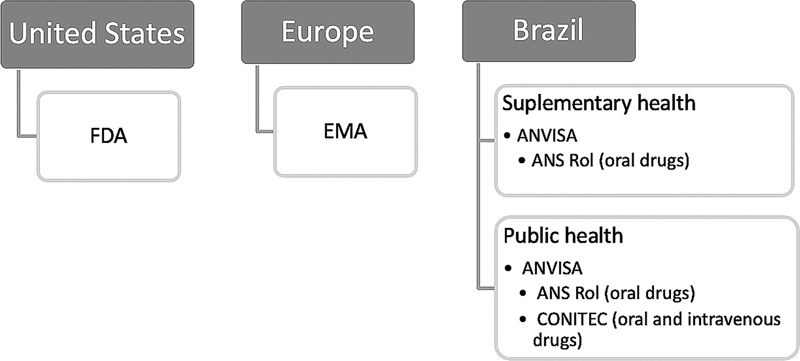
There are national differences in the regulatory processes for new approvals. The United States, through the Food and Drug Administration (FDA), and Europe, via the European Medicines Agency (EMA), are the most important global regulatory bodies.
Across Latin America (LATAM), the processes for granting marketing authorization for new pharmaceutical products differ significantly from one country to another. In certain nations, these processes are characterized by regulatory restrictions and a limited degree of flexibility, which can result in substantial delays or, in some cases, prevent innovative medicines from reaching the market altogether.
In Brazil, the Brazilian Health Regulatory Agency (Agência Nacional de Vigilância Sanitária, ANVISA, in Portuguese) defines the criteria and steps for releasing a new drug to the population.
Given the multitude of regulatory hurdles, administrative complexities, and structural delays inherent in both the public and private healthcare systems in Brazil, the present study advances the hypothesis that Brazilian patients face significantly longer waiting periods to access newly approved oncologic drugs when compared to patients in countries such as the United States and various European nations. Moreover, it is posited that these extended delays in treatment availability may adversely affect the clinical outcomes and overall prognosis of cancer patients in Brazil, potentially widening the gap in survival rates and quality of care between Brazil and higher-income regions.
The primary objective of the current study is to highlight and analyze the disparities in submission and authorization timelines for novel oncological therapies between 2010 and 2021, focusing on Brazil, the United States, and Europe. The study compares the approval timelines of the key regulatory bodies in each region: ANVISA, the FDA, and the EMA. Additionally, the study examines the duration of the review and analysis processes carried out by these agencies, providing insight into the efficiency of their regulatory frameworks and the factors that may influence the speed of approval.
In Brazil, after ANVISA approval, oral drugs require additional review by the ANS for private coverage, and all drugs undergo CONITEC assessment for public incorporation. Considering these steps, a secondary objective of this study was to evaluate oral drug approval timelines in Brazil, including ANS and CONITEC processes. (
Fig. 1 Approval flow in the United States, Europe, and Brazil.
The present study reviewed the regulatory databases of the FDA, EMA, and ANVISA to identify new oncology therapies approved in the United States, Europe, and Brazil from 2010 to 2021, analyzing the timing of regulatory activities. Additionally, it evaluated the time required for incorporation by ANS and CONITEC in Brazil. The submission histories for the FDA and EMA were obtained from public data and verified through their official websites (
This article's structure is based on the study “Cancer Therapy Approval Timings, Review Speed, and Publication of Pivotal Registration Trials in the United States and Europe, 2010-2019,”
The approval times (in days) for oncological therapies were assessed using the Kaplan–Meier (KM) method, presenting results as medians and 95% CIs. The Log-Rank test was used to compare KM curves across regulatory agencies, while Cox regression was applied to estimate hazard ratios (HRs), with a 95%CI. The analyses were performed using R software (R Foundation for Statistical Computing) version 4.4.0, with a significance level set at p < 0.05.
The current study did not require approval from an Ethics Committee, as it does not involve human subjects.
The present study focuses solely on medications submitted for analysis in Brazil between 2010 and 2021, totaling 61 therapies. The analyzed drugs and their indicated diseases are shown in
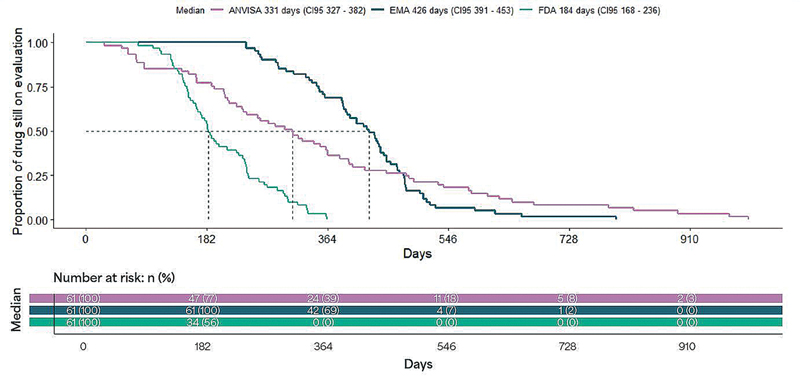
Fig. 2 Kaplan-Meier curves comparing the time until approval from the Brazilian Health Regulatory Agency (Agência Nacional de Vigilância Sanitária, ANVISA, in Portuguese), the European Medicines Agency (EMA), and the Food and Drug Administration (FDA).
| Drug | Initial disease indication |
|---|---|
| Abemaciclib | Breast cancer |
| Abiraterone | Prostate cancer |
| Acalabrutinib | Differing indications |
| Ado-trastuzumab emtansine | Breast cancer |
| Afatinib | NSCLC |
| Alectinib | NSCLC |
| Alpelisib | Breast cancer |
| Apalutamide | Prostate cancer |
| Atezolizumab | Urothelial cancer |
| Avelumab | Merkel cell carcinoma |
| Axitinib | Renal cell carcinoma |
| Brentuximab vedotin | Hodgkin & anaplastic large cell lymphoma |
| Brigatinib | NSCLC |
| Cabazitaxel | Prostate cancer |
| Cabozantinib | Medullary thyroid cancer |
| Carfilzomib | Multiple myeloma |
| Cemiplimab | Squamous cell carcinoma |
| Cobimetinib | Melanoma |
| Crizotinib | NSCLC |
| Dabrafenib | Melanoma |
| Daratumumab | Multiple myeloma |
| Darolutamide | Prostate cancer |
| Decitabine | Myelodysplastic syndrome |
| Dinutuximab | Neuroblastoma |
| Durvalumab | Differing indications |
| Elotuzumab | Multiple myeloma |
| Encorafenib | Melanoma |
| Enzalutamide | Prostate cancer |
| Eribulin | Breast cancer |
| Gilteritinib | Acute Myeloid leukemia |
| Ibrutinib | Mantle cell lymphoma |
| Inotuzumab ozogamicin | Acute lymphocytic leukemia |
| Ipilimumab | Melanoma |
| Ixazomib | Multiple myeloma |
| Larotrectinib | NTRK gene fusion |
| Lenvatinib | Papillary thyroid cancer |
| Lorlatinib | NSCLC |
| Midostarium | Acute Myeloid leukemia |
| Moxetumomab pasudotox | Hairy cell leukemia |
| Neratinib | Breast cancer |
| Niraparib | Ovarian cancer |
| Nivolumab | Melanoma |
| Obinutuzumab | Chronic lymphocytic leukemia |
| Ofatumumab | Chronic lymphocytic leukemia |
| Olaparib | Ovarian cancer |
| Osimertinib | NSCLC |
| Palbociclib | Breast cancer |
| Pazopanib | Renal cell carcinoma |
| Pembrolizumab | Melanoma |
| Pertuzumab | Breast cancer |
| Radium 223 | Prostate cancer |
| Ramucirumab | Gastric cancer |
| Regorafenib | Colorectal cancer |
| Ribociclin | Breast cancer |
| Ruxolitinib | Myelofibrosis |
| Siltuximab | Castleman's disease |
| Trabectedin | Differing indications |
| Trametinib | Melanoma |
| Vemurafenib | Melanoma |
| Venetoclax | Chronic lymphocytic leukemia |
| Ziv-aflibercept | Colorectal cancer |
Abbreviation: NSCLC, non-small-cell lung cancer; NTKR, neurotrophic tyrosine receptor kinase.
| Agencies | Median time in days (95%CI)* | HR (95%CI) | P-value (HR) |
|---|---|---|---|
| ANVISA | 331 (327, 382) | − | − |
| EMA | 426 (391, 453) | 0.90 (0.62; 1.30) | 0.600 |
| FDA | 184 (168, 236) | 5.38 (3.44; 8.40) | < 0.001 |
Abbreviations: ANVISA, Agência Nacional de Vigilância Sanitária (Brazilian Health Regulatory Agency, in English); EMA, European Medicines Agency; FDA, Food and Drug Administration; HR, hazard ratio (estimated by the Cox model).
Notes: *Median time evaluated by Kaplan-Meier method, p < 0.001 in the Log-Rank test for curve comparison.
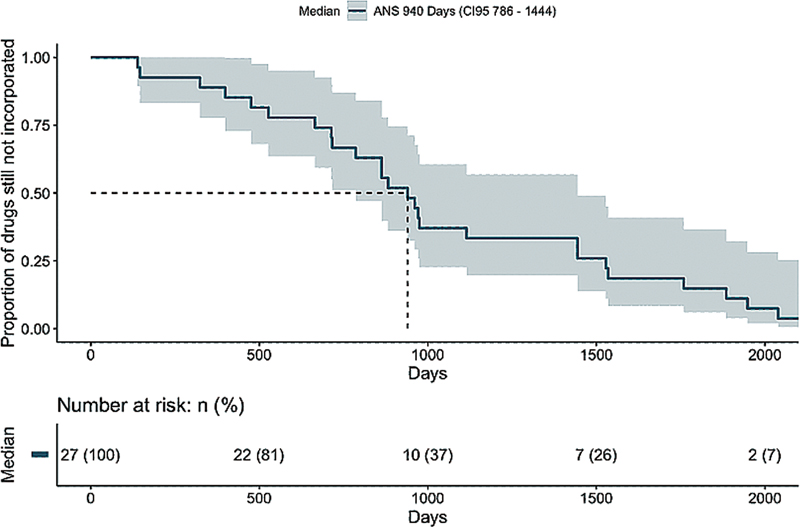
Of the 61 ANVISA-approved therapies, 35 were oral (
Fig. 3 Kaplan–Meier curves of the time until approval from the ANS.
| Drug | Initial disease indication |
|---|---|
| Abemaciclib | Breast cancer |
| Abiraterone | Prostate cancer |
| Acalabrutinib | Differing indications |
| Afatinib | NSCLC |
| Alectinib | NSCLC |
| Alpelisib | Breast cancer |
| Apalutamide | Prostate cancer |
| Axitinib | Renal cell carcinoma |
| Brigatinib | NSCLC |
| Cabozantinib | Medullary thyroid cancer |
| Cobimetinib | Melanoma |
| Crizotinib | NSCLC |
| Dabrafenib | Melanoma |
| Darolutamide | Prostate cancer |
| Encorafenib | Melanoma |
| Enzalutamide | Prostate cancer |
| Gilteritinib | Acute myeloid leukemia |
| Ibrutinib | Mantle cell lymphoma |
| Ixazomib | Multiple myeloma |
| Larotrectinib | NTRK gene fusion |
| Lenvatinib | Papillary thyroid cancer |
| Lorlatinib | NSCLC |
| Midostarium | Acute myeloid leukemia |
| Neratinib | Breast cancer |
| Niraparib | Ovarian cancer |
| Olaparib | Ovarian cancer |
| Osimertinib | NSCLC |
| Palbociclib | Breast cancer |
| Pazopanib | Renal cell carcinoma |
| Regorafenib | Colorectal cancer |
| Ribociclin | Breast cancer |
| Ruxolitinib | Myelofibrosis |
| Trametinib | Melanoma |
| Vemurafenib | Melanoma |
| Venetoclax | Chronic lymphocytic leukemia |
Abbreviations: ANS, Agência Nacional de Saúde (National Supplementary Health Agency, in English); NSCLC, non-small-cell lung cancer; NTKR, neurotrophic tyrosine receptor kinase.
With approximately 10 million cancer-related deaths in 2020, the disease remains one of the leading global causes of mortality.
In the present study, the FDA demonstrated the fastest approval times, being more than 5 times quicker than ANVISA (HR: 5.38; 95%CI: 3.44–8.40). While ANVISA proved faster than the EMA in granting marketing authorization, Brazilian patients face additional delays due to post-ANVISA reviews by ANS and CONITEC. For example, nearly ¼ of oral therapies had not been incorporated into ANS by 2021, and only 3 drugs were approved by CONITEC, reflecting substantial barriers to access within the public system. These findings underscore that, although regulatory performance in Brazil has improved, real-world access remains significantly delayed.
Delays in oncology drug availability have direct consequences on survival and quality of life. Previous studies have shown that longer times to market access are associated with worse clinical outcomes and increased inequities across health systems.
The present study has several limitations. First, the regulatory databases available in FDA, EMA, and ANVISA do not always provide precise and comprehensive submission or approval dates, which may affect accuracy. Second, the study period (2010–2021) encompasses the coronavirus disease 2019 (COVID-19) pandemic, when expedited pathways and emergency authorizations may have artificially shortened approval times for some drugs. Third, all oncologic therapies were aggregated into a single category, despite the heterogeneity between immunotherapies, hormone therapies, tyrosine kinase inhibitors, and antibody-drug conjugates, which likely face different regulatory dynamics. A subgroup analysis by drug class could provide additional insights. Fourth, heterogeneity in submission strategies and requirements across FDA, EMA, and ANVISA (such as dossier completeness, reliance mechanisms, or submission timing) may confound direct comparisons of approval timelines.
Despite these limitations, our findings highlight meaningful disparities in drug approval and access among Brazil, the United States, and Europe. Streamlining post-ANVISA evaluations, especially through ANS and CONITEC, is critical to reducing delays. Efforts to adopt more efficient reliance mechanisms, improve regulatory transparency, and harmonize requirements could help ensure that Brazilian patients gain faster access to life-saving oncologic therapies.
There are notable disparities in the time required for patients to gain access to newly approved oncologic therapies across Brazil, the United States, and Europe. While ANVISA demonstrated faster approval timelines than the EMA, actual patient access in Brazil remains substantially delayed due to additional evaluations by ANS and CONITEC. During the study period, 23% of oral drugs approved by ANVISA were not incorporated by the ANS, and only 3 therapies were approved by CONITEC, underscoring persistent barriers to timely access. Streamlining these post-ANVISA processes and adopting reliance mechanisms, as increasingly applied in other Latin American settings, will be essential to ensure more equitable and timely availability of life-saving cancer treatments in Brazil.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Wilking, N and Bucsics, A and Kandolf Sekulovic, L. Achieving equal and timely access to innovative anticancer drugs in the European Union (EU): summary of a multidisciplinary CECOG-driven roundtable discussion with a focus on Eastern and South-Eastern EU countries. ESMO Open [online]. 2019, vol. 4, p. e000550. https://doi.org/10.1136/esmoopen-2019-000550 Ver referência
2. Barrios, C and Lima Lopes, Gd and Yusof, M M and Rubagumya, F and Rutkowski, P and Sengar, M. Barriers in access to oncology drugs - a global crisis. Nat Rev Clin Oncol [online]. 2023, vol. 20, p. 7-15. https://doi.org/10.1038/s41571-022-00700-7 Ver referência
3. Lythgoe, M P and Desai, A and Gyawali, B. Cancer Therapy Approval Timings, Review Speed, and Publication of Pivotal Registration Trials in the US and Europe, 2010-2019. JAMA Netw Open [online]. 2022, vol. 5, p. e2216183. https://doi.org/10.1001/jamanetworkopen.2022.16183 Ver referência
4. Jenei, K. The Timing of Cancer Drug Approvals in the United States and Europe. JAMA Netw Open [online]. 2022, vol. 5, p. e2216191. https://doi.org/10.1001/jamanetworkopen.2022.16191 Ver referência
5. Nadler, M B and Wilson, B E and Desnoyers, A and Valiente, C M and Saleh, R R and Amir, E. Magnitude of effect and sample size justification in trials supporting anti-cancer drug approval by the US Food and Drug Administration. Sci Rep [online]. 2024, vol. 14, p. 459. https://doi.org/10.1038/s41598-023-50694-0 Ver referência
6. Argotti, U and Leyens, L and Lisbona, C. Comparison of the Latin America Regulation Landscape and International Reference Health Authorities to Hasten Drug Registration and Clinical Research Applications. Ther Innov Regul Sci [online]. 2023, vol. 57, p. 1287-1297. https://doi.org/10.1007/s43441-023-00565-7 Ver referência
7. Barrios, C and Freitas-Junior, R and Martins, S and Bines, J and Estevez-Diz, M DP and Caleffi, M. Challenge of Incorporating New Drugs for Breast Cancer in Brazil: A Proposed Framework for Improving Access to Innovative Therapies. JCO Glob Oncol [online]. 2021, vol. 7, p. 474-485. https://doi.org/10.1200/GO.20.00566 Ver referência
8. GLOBAL CANCER OBSERVATORY. Cancer tomorrow, World Health Organization. Available in: . It is accessed on February 10, 2024 [online]. Available from: <https://gco.iarc.who.int/tomorrow/en/dataviz/isotype?years=2040>.
9. Durán, C E and Cañás, M and Urtasun, M A. Regulatory reliance to approve new medicinal products in Latin American and Caribbean countries. Rev Panam Salud Publica [online]. 2021, vol. 45, p. e10. https://doi.org/10.26633/RPSP.2021.10 Ver referência
10. Huynh-Ba, K and Beumer Sassi, A. ANVISA: an introduction to a new regulatory agency with many challenges. AAPS Open [online]. 2018, vol. 4, p. 9. https://doi.org/10.1186/s41120-018-0029-x Ver referência
11. ANS -National Supplementary Health Agency. Available in: . Accessed in: February 12, 2024 [online]. Available from: <http://www.ans.gov.br>.
12. Published on 12/14/ . Available in: . Accessed on January 15, 2024 [online]. Available from: <https://bvsms.saude.gov.br/bvs/saudelegis/ans/2022/res0555_16_12_2022.html>.
13. gov. br. published 05/25/2022/ updated 11/01/ . Available in: . It was accessed on February 10, 2024 [online]. Available from: <https://www.gov.br/conitec/pt-br/assuntos/a-comissao/legislacao>.
14. BRAZIL. Ministry of Health. Minister's Office. Portaria n° 874, de 16 de maio de . Available in . Accessed on February 2, 2024 [online]. Available from: <https://bvsms.saude.gov.br/bvs/saudelegis/gm/2013/prt0874_16_05_2013.html>.
15. CONITEC - National Commission for the Incorporation of Technologies Available in. . Accessed February 12, 2024 [online]. Available from: <https://www.gov.br/conitec/pt-br>.
16. Ferlay, J and Colombet, M and Soerjomataram, I. Cancer statistics for the year 2020: An overview. Int J Cancer [online]. 2021. https://doi.org/10.1002/ijc.33588 Ver referência
17. Sehdev, S and Gotfrit, J and Elias, M and Stein, B D. Impact of Systemic Delays for Patient Access to Oncology Drugs on Clinical, Economic, and Quality of Life Outcomes in Canada: A Call to Action. Curr Oncol [online]. 2024, vol. 31, p. 1460-1469. https://doi.org/10.3390/curroncol31030110 Ver referência
Dados de acesso insuficientes para visualização no mapa.