Lung cancer is the leading cause of cancer-related death worldwide. Estimates from the World Health Organization indicate that the disease was responsible for 1.8 million deaths in 2020.
The global distribution of lung cancer reveals that just over half of the incidence and 61.9% of deaths in 2020 occurred in Asia. Regarding countries, China has the highest number of cases (37.0%) and deaths (39.8%), followed by the United States with 10.3% of cases and 7.7% of deaths, then Japan with 6.3% of cases and 4.6% of deaths.
In the state of Sergipe, Brazil, according to INCA estimates for 2022, 240 new cases of lung cancer were expected in 2023. In absolute numbers, it is the fourth most common cancer type in the state, with the exception of non-melanoma skin cancers. This equates to a standardized incidence rate of 11.25 for men and 8.46 for women.
There were two distinct analyses being conducted. First was the complete period, from 1980 to 2022, and second a focused evaluation of the most recent 10 year interval (2013–2022). The rationale for conducting these analyses separately was to achieve both a comprehensive epidemiological overview and a contemporary assessment reflective of current disease patterns.
The current study represents the first robust analysis of lung cancer mortality trends in Sergipe since the inception of systematic record keeping. Importantly, the data underscore the critical need to reduce diagnostic delays, a modifiable factor directly impacting patient survival. Collectively, these evidence-based interventions could substantially reduce the burden of lung cancer morbidity and mortality across Sergipe.
The present study aims to analyze the temporal trend and spatial distribution of lung cancer mortality in Sergipe from 1980 to 2022.
Furthermore, we intend to calculate standardized and age-specific mortality rates for lung cancer by sex and health region; to analyze the spatial distribution of lung cancer mortality for both sexes across municipalities in our state from 1980 to 2022 and from 2013 to 2022; and to correlate the Municipal HDI (M-HDI) and municipal GDP per capita with crude and standardized mortality rates for both sexes.
The present is an observational ecological study with a time series and spatial analysis on lung cancer mortality from 1980 to 2022. The study was conducted in the state of Sergipe, the smallest Brazilian state, covering an area of 21,938 km2, located in the Northeast region of the country. Sergipe is made up of 75 municipalities divided into 7 health regions and has an estimated population of 2.21 million inhabitants.
The study population was composed of unidentified individuals diagnosed with lung cancer and who died due to the disease between 1980 and 2022. Data were chosen from the Brazilian Ministry of Health's Mortality Information System (Sistema de Informações sobre Mortalidade, SIM, in Portuguese), which is an epidemiological surveillance system. Until 1995, the International classification of Diseases, Ninth Revision (ICD-9) was used and, after 1996, the tenth revision (ICD-10). In the current study, according to the ICD-9, the cases of interest were identified as code 162, which refers to malignant tumors of the trachea, bronchi, and lung. From the ICD-10, codes C33 and C34 were used, which refer to neoplasia of the trachea and neoplasia of the bronchi and lungs respectively.
Age standardization was carried out with reference to the estimate of the world population suggested by Segi.
The spatial analysis was carried out using cartographic bases for the state of Sergipe made available by the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística, IBGE, in Portuguese) and the QGIS (QGIS Development Team) software, version 3.10, was used to create thematic maps. It uses the absolute number of deaths and standardized mortality rates.
For spatial statistical analysis, the TerraView (Instituto Nacional de Pesquisas Espaciais) software, version 4.2.2, was used, which is a geographic information system that allows the creation of maps. The Local Empiric Bayes method was used to smooth rates and the Global and Local Moran indices to investigate whether the spatial distribution of rates occurred randomly or standardized.
For the statistical significance analysis, the pseudo-significance test was used with p-values < 0.05. The spatial analyses of both study periods (1980–2022 and 2013–2022) were systematically compared. The evaluation of the most recent decade (2013–2022) particularly reflects current epidemiological patterns.
Official information was collected on municipal data such as GDP per capita and M-HDI. The latter is obtained by the simple arithmetic average of three sub-indices: longevity, education, and income.
The current study was approved by the Research Ethics Committee of Universidade Federal de Sergipe under the protocol number CAAE: 70661923.4.0000.5546.
From 1980 to 2022, lung cancer accounted for 1,815 deaths among women and 2,657 among men in Sergipe. In absolute numbers, the Aracaju health region recorded the highest mortality rate for both genders during this period.
| 1980–2022 | Male | Female | 2013–2022 | Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Health region | AV | CR | SR | AV | CR | SR | AV | CR | SR | AV | CR | SR | ||
| Aracaju | 1,432 | 11.1 | 15.9 | 943 | 6.5 | 7.0 | 470 | 12.0 | 13.3 | 393 | 8.8 | 7.1 | ||
| Estância | 223 | 5.1 | 6.9 | 139 | 3.1 | 3.7 | 92 | 7.7 | 8.2 | 74 | 6.0 | 5.7 | ||
| Itabaiana | 222 | 5.0 | 5.9 | 143 | 3.1 | 3.4 | 113 | 9.2 | 8.9 | 75 | 5.9 | 4.9 | ||
| Lagarto | 214 | 4.6 | 5.2 | 179 | 3.7 | 3.8 | 119 | 9.5 | 8.5 | 99 | 7.5 | 5.9 | ||
| Nossa Senhora da Glória | 122 | 4.1 | 5.3 | 74 | 2.5 | 3.2 | 59 | 6.9 | 7.0 | 36 | 4.2 | 4.0 | ||
| Nossa Senhora do Socorro | 311 | 5.9 | 9.2 | 238 | 4.4 | 6.0 | 143 | 8.7 | 11.0 | 131 | 7.5 | 7.9 | ||
| Propriá | 133 | 4.4 | 5.3 | 99 | 3.2 | 3.3 | 57 | 7.3 | 7.0 | 48 | 6.1 | 5.2 | ||
| Sergipe | 2,657 | 7.1 | 9.3 | 1,815 | 4.6 | 5.1 | 1,053 | 7.3 | 7.0 | 856 | 7.4 | 6.4 | ||
Abbreviations: AV, absolute value; CR, crude rate; S, standardized rate.
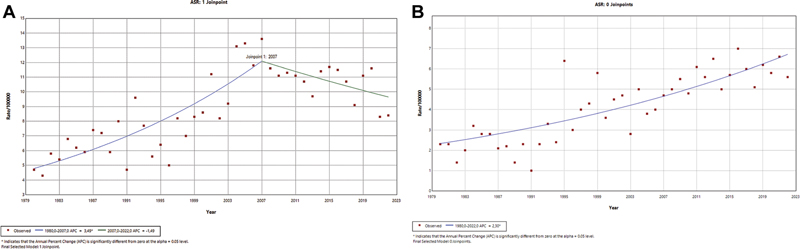
The age-standardized male mortality rate from lung cancer in Sergipe showed an increasing trend in the period from 1980 to 2007 and maintained a stable trend between 2007 and 2022. Despite the falling curve, this trend is still not considered statistically significant. Furthermore, an analysis of the age-standardized female mortality rate from lung cancer in Sergipe revealed an increasing trend throughout the analyzed period (
Fig. 1 Mortality trends due to lung cancer in men (A) and women (B) in Sergipe from 1980 to 2022.
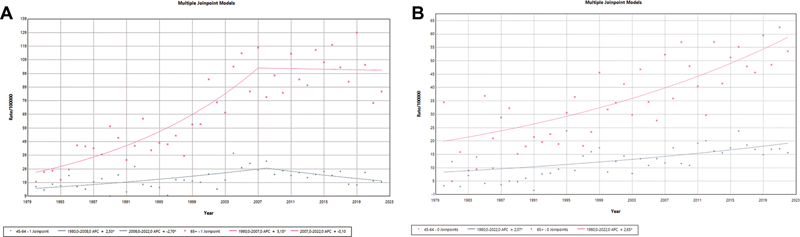
The male analysis by age group showed an increasing trend in mortality in the population aged 45 to 64 years from 1980 to 2008 with a downward trend since then. The population older than 65 years of age showed an increasing trend between 1980 and 2007 and stability since then. The female analysis by age group showed an increasing trend in the period between 1980 and 2022 for those aged between 45 and 64 years and for those older than 65 years of age (
Fig. 2 Mortality trends due to lung cancer in men (A) and women (B) in Sergipe from 1980 to 2022 in the age groups from 45 to 64 years and over 65 years.
The spatial analysis data were divided into two groups: the entire proposed period (1980 to 2022) and the last 10 years (2013 to 2022). Male and female populations were analyzed separately for each study period.
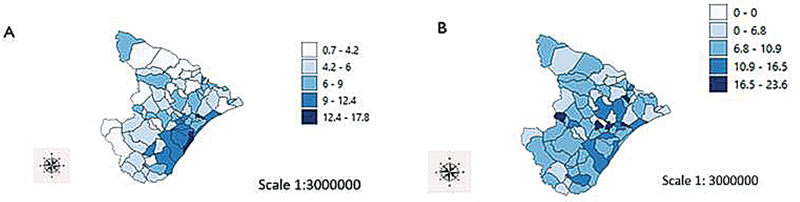
Mortality from lung cancer in men has, in absolute numbers, the highest concentration in the capital city of Aracaju. The age-standardized male mortality rate in the city remains the highest concentration of deaths, highlighting the municipality of Carmópolis also with the highest rates.
The distribution of the age-standardized male mortality rate by municipalities revealed to be statistically significant (p = 0.003), with an index value of 0.284 from 1980 to 2022. From 2013 to 2022, the spatial distribution of the proportion of the number of deaths was similar to the period from 1980 to 2022, however the distribution by municipality did not reveal statistical significance (p = 0.283) (
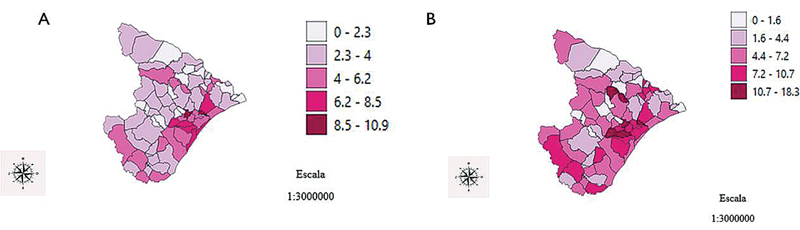
Fig. 3 Spatial distribution of the age-standardized rate of male mortality from lung cancer in Sergipe (A) from 1980 to 2022, and (B) from 2013 to 2022. Source: Original work using cartographic data from the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística, IBGE, in Portuguese). Coordinate Reference System: SIRGAS 2000/UTM Zone 24S.
The Bayesian model, which smoothes differences between municipalities, allows correction between populations and reduces extreme values.
Fig. 4 Distribution of smoothed male mortality rates from lung cancer (A) from 1980 to 2022, and (B) from 2013 to 2022, based on the Bayesian model. Source: Original work using cartographic data from IBGE. Coordinate Reference System: SIRGAS 2000/UTM Zone 24S.
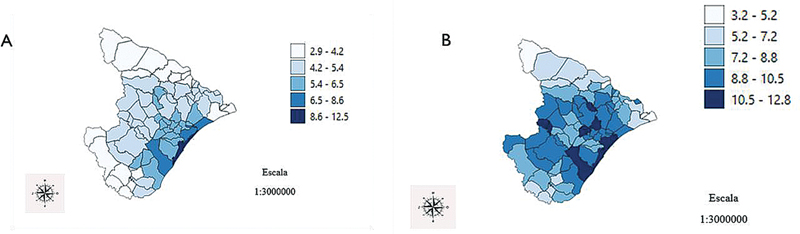
In the spatial analysis of mortality using the age-standardized rate from 1980 to 2022, the municipalities of Carmópolis and Divina Pastora stood out with the highest rates in the female population. The spatial distribution was statistically significant, with p = 0.001 and index value of 0.362. Between 2013 and 2022, as in the previous period, Carmópolis and Divina Pastora maintained high mortality rates. The analysis of standardized mortality rates by municipality revealed a statistically significant distribution, with p = 0.003 and an index value of 0.226 (
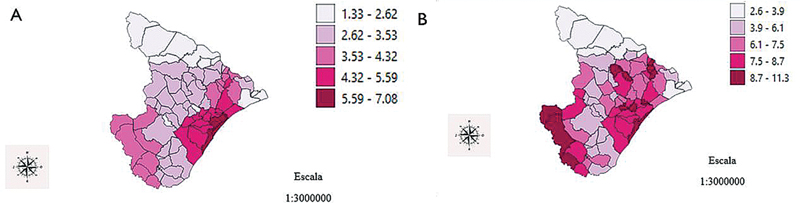
Fig. 5 Spatial analysis of the age-standardized rate of female mortality from lung cancer in Sergipe (A) from 1980 to 2022, and (B) from 2013 to 2022. Source: Original work using cartographic data from IBGE. Coordinate Reference System: SIRGAS 2000/UTM Zone 24S.
From 1980 to 2022, the Bayesian model shows the highest concentrations of mortality in Aracaju, Barra dos Coqueiros, and Santo Amaro das Brotas. This distribution of smoothed rates was statistically significant (p = 0.001), with an index value 0.715. Between 2013 and 2022, the smoothed mortality rates bring interesting changes in the state's distribution with a greater number of municipalities with higher rates. Aracaju and Barra dos Coqueiros, as in the previous period, maintain high rates. The analysis of mortality rates smoothed by the Bayesian estimation model demonstrated a statistically significant distribution (p = 0.001), with an index value of 0.646 (
Fig. 6 Distribution of smoothed female mortality rates from lung cancer (A) from 1980 to 2022, and (B) from 2013 to 2022, based on the Bayesian model. Source: Original work using cartographic data from IBGE. Coordinate Reference System: SIRGAS 2000/UTM Zone 24S.
The correlation analysis of crude male and female mortality rates with the M-HDI demonstrated a statistically significant relationship for females (p = 0.0016).
The correlation analysis of standardized male and female mortality rates with the M-HDI revealed a statistically significant relationship between the variables (p = 0.0000 for the male subjects, and p = 0.0042 for the female subjects).
The analysis of the correlation between the crude mortality rate and the municipality's GDP per capita demonstrated a statistically significant relationship only for females (p = 0.0310).
The analysis of the correlation between the standardized mortality rate and the municipality's GDP per capita revealed a statistically significant relationship only for males (p = 0.0464).
Lung cancer was responsible for 4,472 deaths in Sergipe from 1980 to 2022. The temporal analysis of mortality in the male population showed a rising curve from 1980 to 2007 and a stable trend since then. In the female population, the mortality curve was on the rise throughout the studied period.
In the spatial analysis, we identified pockets of high mortality for both sexes. From 2013 to 2022, the municipalities of Carmópolis and Divina Pastora stood out with the highest mortality rates in both populations. Standardized mortality rates were higher among men compared to women in Sergipe and in all health regions, regardless of period. Global data also demonstrate higher cancer mortality rates in men when compared to the female gender.
The male mortality rate in Sergipe has shown a downward trend since 2007 (APC = 1.49%) but still without statistical significance. The female sector, however, shows a rising curve (APC = 2.3%). In Spain,
In Sergipe, male data showed the peak in mortality in 2007. In Italy, the peak lung cancer mortality rate in women occurred 35 years after the peak mortality rate.
The Aracaju health region, which concentrates the capital and part of the municipalities of the Greater Aracaju metropolitan area, presented the highest standardized mortality rates for both sexes from 1980 to 2022. From 2013 to 2022, the region maintains the highest male mortality rate, although it is surpassed in female mortality by the Nossa Senhora do Socorro health region, which also encompasses part of the municipalities in the metropolitan region. Our data corroborates with the national data of higher concentration of mortality from the disease in metropolitan regions.
The present study found a statistically significant relationship between lung cancer mortality and M-HDI in both sexes. We did not find any correlation data between M-HDI and lung cancer mortality in the literature, although its relationship with HDI is well established. Global data from 2020 showed that more than 90% of cases of the disease and 77% of deaths occurred in countries with a high or very high HDI.
The relationship between GDP per capita and the standardized mortality rate in our population proved to be statistically significant only for males. We did not find data in the literature on this topic. However, previous data has already shown that the Southeast region, which generates around 60% of the country's GDP, has the highest mortality rates from the disease in the country.
The data from the present study in Sergipe did not demonstrate significant changes in lung cancer mortality trends during the coronavirus disease 2019 (COVID-19) pandemic in the years 2020 to 2022. The influence of the COVID-19 pandemic on lung cancer mortality was also investigated in the province of Taranto, Italy, and no significant changes in mortality were found.
The mortality trends for lung cancer among both men and women in Sergipe align with global patterns. The present study demonstrates clusters of mortality from lung cancer in both sexes and provides relevant information for the implementation of future actions for tobacco control and screening in at-risk populations, in addition to helping the organization of the country's health system in targeting public resources and organizing health services. No prior studies from Sergipe are available for comparative analysis, underscoring the novelty of these findings. New studies with joint analysis of incidence and mortality, associated with epidemiological and histological data may provide more relevant information in the future.
As a secular trend analysis, this study must account for the low number of events in the early period (particularly the 1980s), likely due to diagnostic confirmation challenges and inadequate record-keeping. Additionally, the accuracy of mortality data depends heavily on the training and expertise of physicians completing death certificates. In the present study, we identified and excluded cases with incorrectly filled documentation.
Another critical limitation is the difficulty in accessing cancer diagnostics—not only for lung cancer but also for malignancies in general. Routine barriers, such as delays or failures in obtaining histopathological confirmation, directly impact treatment initiation. Consequently, mortality rates in this sample may be underestimated.
The absence of incidence data is a key limitation. The relationship between incidence and mortality rates is crucial for spatial analyses, and future studies should address this gap to improve understanding of the disease's burden to the state. Furthermore, smoking prevalence data would enhance the robustness of these findings.
A major strength of this study is its comprehensive overview of lung cancer mortality in Sergipe, stratified by sex and health region. By dividing the analysis into 2 periods (43-year trends and the most recent decade), we provide both long-term insights and up-to-date mortality patterns, reflecting current realities.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. World Health Organization (WHO). Geneva: WHO; . Available from: . Accessed: May 1, 2024 [online]. Available from: <https://www.who.int/news-room/fact-sheets/detail/lung-cancer>.
2. Ministério da Saúde. Instituto Nacional de Câncer (INCA). Estimativa 2023–Incidência de Câncer no Brasil. , 2022.
3. Bray, F and Laversanne, M and Sung, H. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin [online]. 2024, vol. 74, p. 229-263. https://doi.org/10.3322/caac.21834 Ver referência
4. Li, C and Lei, S and Ding, L. Global burden and trends of lung cancer incidence and mortality. Chin Med J (Engl) [online]. 2023, vol. 136, p. 1583-1590. https://doi.org/10.1097/CM9.0000000000002529 Ver referência
5. Sung, H and Ferlay, J and Siegel, R L. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin [online]. 2021, vol. 71, p. 209-249. https://doi.org/10.3322/caac.21660 Ver referência
6. Lima, M S and Siqueira, H FF and Moura, A R. Temporal trend of cancer mortality in a Brazilian state with a medium Human Development Index (1980-2018). Sci Rep [online]. 2020, vol. 10, p. 21384. https://doi.org/10.1038/s41598-020-78381-4 Ver referência
7. Rio de Janeiro: IBGE; . Available from: . Accessed: May 26, 2024 [online]. Available from: <https://cidades.ibge.gov.br/brasil/pesquisa/37/30255>.
8. Segi, M. Cancer mortality for selected sites in 24 countries. Japan Cancer Society, .
9. National Institutes of Health (NIH). National Cancer Institute. Division of Cancer Control & Population Sciences. Bethesda, MA: National Institutes of Health; . Available from: . Accessed: May 26, 2024 [online]. Available from: <https://surveillance.cancer.gov/help/joinpoint/setting-parameters/method-and-parameters-tab/apc-aapc-tau-confidence-intervals/estimate-average-percent-change-apc-and-confidence-interval>.
10. Ottonelli, J and Silva, J and Marin, S. Desenvolvimento humano no Nordeste: um estudo sobre a influência de indicadores sociais no IDH-M (1991 e 2000). Econ Desenvol (Recife) [online]. 2013, vol. 12, p. 7-35.
11. Shapiro, S S and Wilk, M B. An analysis of variance test for normality (complete samples). Biometrika [online]. 1965, vol. 52, p. 591-611. https://doi.org/10.1093/biomet/52.3-4.591 Ver referência
12. The R Project for Statistical Computing. Vienna: R Foundation for Statistical Computing; [online]. Available from: <https://www.r-project.org/>.
13. Cayuela, L and Gaeta, A M and Lopez-Campos, J L and Reinoso-Arija, R and Cayuela, A. Age-period-cohort effect on lung cancer mortality in Spain, 1982-2021. Lung Cancer [online]. 2023, vol. 178, p. 269-276. https://doi.org/10.1016/j.lungcan.2023.03.004 Ver referência
14. Catelan, D and Biggeri, A and Bucchi, L. Epidemiologic transition of lung cancer mortality in Italy by sex, province of residence and birth cohort (1920-1929 to 1960-1969). Int J Cancer [online]. 2023, vol. 153, p. 1746-1757. https://doi.org/10.1002/ijc.34657 Ver referência
15. Souza, G S and Junger, W L and Silva, G A. Lung cancer mortality trends in different urban settings in Brazil, 2000-2015. Epidemiol Serv Saude [online]. 2019, vol. 28, p. e2018421. https://doi.org/10.5123/S1679-49742019000300003 Ver referência
16. Wunsch Filho, V and Moncau, J E. [Cancer mortality in Brazil 1980-1995: regional patterns and time trends]. Rev Assoc Med Bras [online]. 2002, vol. 48, p. 250-257. https://doi.org/10.1590/s0104-42302002000300040 Ver referência
17. Addabbo, F and Giotta, M and Mincuzzi, A. No Excess of Mortality from Lung Cancer during the COVID-19 Pandemic in an Area at Environmental Risk: Results of an Explorative Analysis. Int J Environ Res Public Health [online]. 2023, vol. 20, p. 5522. https://doi.org/10.3390/ijerph20085522 Ver referência
Dados de acesso insuficientes para visualização no mapa.