Spontaneous retroperitoneal hemorrhage (SPH) is a rare clinical entity that can occasionally be life-threatening. It poses a dilemma in diagnosis and management due to its varied clinical presentation. The common causes of non-traumatic causes of perirenal hemorrhage include renal cell carcinoma (RCC), renal angiomyolipoma (AML) vascular diseases, blood dyscrasia, and infections
Herein, we present a clinical case of a patient with spontaneous perirenal hematoma with unclear etiology, who was treated with drainage of the hematoma; subsequently, he was diagnosed to have a renal mass at 6-month follow-up.
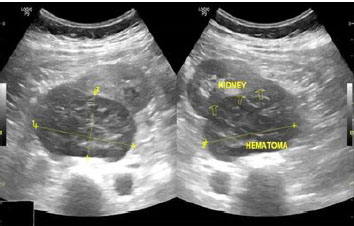
A 51-year-old male patient presented to outpatient department with complaints of right flank pain, since one day, which was sudden in onset, colicky, moderate in intensity and non-radiating in nature. Pain was constant over the last 6 hours and was associated with one episode of vomiting. There was no history of trauma, any bleeding tendency, hematuria, or stone disease. He did not have any previous history of a medical disorder, and presently, was not on any medication. He was a nonsmoker. On examination, his vitals were stable. Abdominal examination showed mild tenderness in the right flank. Bowel sounds were present; the abdomen was soft with no palpable mass. Ultrasonography of the abdomen was done which was suggestive of 106mm x 61mm x 71mm right perirenal heterogenous soft tissue lesion standing order hematoma (
Figura 1 Ultrasound pictures showing the right kidney with perirenal hematoma (106mm x 61mm x 71mm).
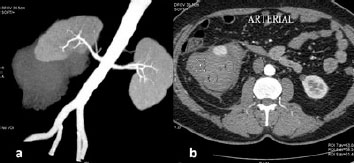
Contrast-enhanced computed tomography scan (CT scan) abdomen and pelvis was done which was suggestive of 15.2 x 10.6x 6.8cm right perinephric collection standing order hematoma (30-35HU [Hounsfield unit]) extending into the right pelvis. The post-contrast study does not show significant enhancement in the collection (
Figura 2 A. Computed tomography (CT) scan reconstructed image of right kidney with perirenal hematoma; B. Cross section CT image during arterial phase showing non-enhancing perirenal hematoma with no other obvious abnormality in the kidney.
The patient was followed up after one month and an ultrasound was done which showed minimal perinephric collection and the patient was asymptomatic. Thus, patient was advised to follow up after 6 months.
At 6 months follow-up, the patient was asymptomatic, on screening ultrasound, there was a suspicious lesion at the lower pole of the right kidney, so a plan was made to do a CT scan. CT scan was suggestive of a well-defined, iso to hypo-dense lesion seen at the posteromedial aspect of the mid and lower poles of the right kidney (Avg-36HU). It measured 7.5 x 6.2 x 6.1cm. The lesion showed an exophytic component with post-contrast enhancement (85HU) in some parts of the lesion (
Figura 3 CT Scan image showing heterogeneously enhancing lesion in the right kidney measuring 74.5mm x 61.6mm x 61mm. A. Image showing transverse section; B. Image showing coronal section.
Trucut biopsy was taken from the lesion, histopathology was suggestive of fibro-adipocytic tissue with one tiny bit of renal tissue and malignant changes were not detected.
In view of the CT scan findings and inconclusive biopsy report, it was decided for surgical removal of the renal lesion. In view of the history of perirenal hematoma and previous intervention, the patient was taken up for right open partial nephrectomy.
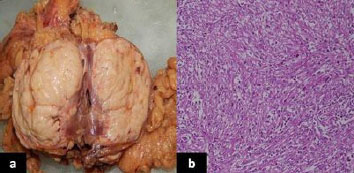
Postoperatively the patient recovered well. Histopathological examination of the surgical specimen revealed papillary renal cell carcinoma (type II), nuclear grade ″4, which was 7.4cm in largest dimension, and the lesion was assigned pathologic staging of pT2a Nx (
Figura 4 A. Cut section of the partial nephrectomy specimen; B. Low power microscopic image showing papillary fronds suggestive of papillary renal cell carcinoma.
In the present era, RCCs are more commonly discovered as incidentalomas on radiological imaging done for other abdominal ailments. This is due to the advancement and invention of newer imaging techniques. The usual presentation of RCC as flank pain, abdominal mass, and total hematuria are less commonly seen now a days. Dougal et al. (1975) discovered 78 documented cases of SPH since 1975, out of which 58% of cases were due to tumors, and the rest were due to benign causes. Similar findings were reported by Cinman et al. (1985) in 27 additional cases of SPH.
In 1956, Carl Reinhold August Wunderlich described spontaneous hemorrhage of the kidney with seepage of blood into the perinephric spaces.
In a meta-analysis by Zhang et al. (2002), it was seen that more than 60% of cases of SPH were due to neoplasms.
The treatment of Wunderlich syndrome ranges from conservative management to immediate exploratory surgery. This depends upon the presentation of the patient and the choice of the operating surgeon. Few urologists are inclined towards early surgery in cases of SPH.
CT scan remains one of the best modalities to diagnose retroperitoneal hemorrhage and RCCs but there is a huge concern regarding the efficiency of CT to diagnose renal tumors when there is bleeding around and in the kidney. As reported by Kendall et al. (1988), an initial CT scan showed no signs of malignancy in about 60% of the patients with SPH. This observation was also seen in our present case and is also supported by a case report by Aldughiman et al., in 2020.
If there is a case of SPH, it can be dealt with either by immediate radical nephrectomy as proposed by Kendall et al. (1988), if the opposite kidney is normal or the nephrectomy to be done in patients with non-fatty lesions except hematomas and rest patients to be followed up with imaging.
As a rule, if the etiology cannot be determined at the primary examination, we should perform a follow-up CT scan at 3-month intervals so that the hematoma can resolve and we can clinch a definitive diagnosis. Malignant renal masses diagnosed on CT scan can be managed by radical nephrectomy or partial nephrectomy. Whereas a benign renal bleed demands an angioembolization. Moreover, if these cases are diagnosed with a renal malignancy in the future, this will affect the staging and prognosis.
For patients having contrast allergy or renal sufficiency, magnetic resonance imaging (MRI) can be used for follow-up. Hashimoto et al. (2007) reported a case in their series who had a renal hemorrhage and the imaging both before and after the drainage of the hematoma showed no malignancy. The patient presented with hematuria after 1 year and was diagnosed with RCC in the same kidney.
Initially, it was advised to perform radical nephrectomy in all patients with spontaneous renal hemorrhage after excluding benign causes.
CARE reporting guidelines were used to prepare this manuscript.
Patients with spontaneous perirenal hemorrhage with unexplained causes should be followed up regularly with imaging in the form of CT scans so that an impending renal tumor can be identified at the earliest. In case of undiagnosed etiology at first presentation, imaging in the form of CT scan/MRI should be done early in follow-up at least at 2-3 months to clinch a definitive diagnosis.
AG Collection and assembly of data, Conception and design, Manuscript writing
AGS Final approval of manuscript, Provision of study materials or patient
RBS Final approval of manuscript
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Polkey, HJ and Vynalek, WJ. Spontaneous non-traumatic perirenal and renal hematomas. An experimental and clinical study. Arch Surg [online]. 1933, vol. 26, p. 196-202.
2. Dougal, WS and Kursh, ED and Persky, L. Spontaneous rupture of the kidney with perirenal hematoma. J Urol [online]. 1975, vol. 114, p. 181-4.
3. Cinman, AC and Farrer, J and Kaufman, JJ. Spontaneous perinephric hemorrhage in a 65-year-old man. J Urol [online]. 1985, vol. 133, p. 829-32.
4. Rousseau, T and Peyret, C and Zerbib, M and Thiounn, N and Flam, T and Debre, B. Circumstances of the detection of kidney cancer. Current part of accidental discoveries. J Urol [online]. 1994, vol. 100, p. 189-95.
5. Agha, RA and Borrelli, MR and Farwana, R and Koshy, K and Fowler, A. For the SCARE Group, The SCARE 2018 statement: updating consensus Surgical Case REport (SCARE) guidelines. Int J Surg [online]. 2018, vol. 60, p. 132-6.
6. Wunderlich, CRA. Handbuch der pathologie und therapie. Ebner & Seubert, 1856.
7. Daskalopoulos, G and Karyotis, I and Heretis, I and Anezinis, P and Mavromanolakis, E and Delakas, D. Spontaneous perirenal hemorrhage: a 10-year experience at our institution. Int Urol Nephrol [online]. 2004, vol. 36, p. 15-9.
8. Katabathina, VS and Katre, R and Prasad, SR and Surabhi, VR and Shanbhogue, AK and Sunnapwar, A. Wunderlich syndrome: cross-sectional imaging review. J Comput Assist Tomogr [online]. 2011, vol. 35, p. 425-33. https://doi.org/10.1097/RCT.0b013e3182203c5e Ver referência
9. Zhang, JQ and Fielding, JR and Zou, KH. Etiology of spontaneous perirenal hemorrhage: a meta-analysis. J Urol [online]. 2002, vol. 167, p. 1593-6.
10. Hao, LW and Lin, CM and Tsai, SH. Spontaneous hemorrhagic angiomyolipoma present with massive hematuria leading to urgent nephrectomy. Am J Emerg Med [online]. 2008, vol. 26, p. 249.
11. Pummer, K and Lammer, J and Wandschneider, G and Primus, G. Renal cell carcinoma presenting as spontaneous retroperitoneal hemorrhage. Int Urol Nephrol [online]. 1990, vol. 22, p. 307-11.
12. Sebastia, MC and Perez-Molina, MO and Alvarez-Castells, A and Quiroga, S and Pallisa, E. CT evaluation of underlying cause in spontaneous subcapsular and perirenal hemorrhage. Eur Radiol [online]. 1997, vol. 7, p. 686-90.
13. Kendall, AR and Senay, BA and Coll, ME. Spontaneous subcapsular renal hematoma: diagnosis and management. J Urol [online]. 1988, vol. 139, p. 246-50.
14. Aldughiman, AW and Alsunbul, A and Al-Gadheeb, A and Almuaiqel, M and Alzahrani, A and Alzahrani, T. Does spontaneous renal hemorrhage mandate close surveillance for impending renal cell carcinoma? A case report and literature review. Int J Surg Case Rep [online]. 2020, vol. 73, p. 44-7.
15. Hashimoto, T and Yamamoto, S and Togo, Y and Ueda, Y and Higuchi, Y and Maruyama, T. Spontaneous rupture of renal cell carcinoma: a case report. Hinyokika Kiyo [online]. 2007, vol. 53, p. 49-52.
16. Gagnier, JJ and Kienle, G and Altman, DG and Moher, D and Sox, H and Riley, D. The CARE guidelines: consensus-based clinical case reporting guideline development. [online]. 2012, vol. 2, p. 38-43.

Dados de acesso insuficientes para visualização no mapa.