Sarcoidosis is a systemic inflammatory disease of undefined etiology, in which noncaseating epithelioid granulomas are found in several organs, mainly in the lungs, lymph nodes, liver, eyes and skin, but can also involve the breast tissue. Accordingly, sarcoidosis can mimic breast cancer, making the differential diagnosis very challenging.
The first case of sarcoidosis was reported in 1877 by Jonathan Hutchinson, at the King’s College Hospital in London (United Kingdom). In 1889, Ernest Besnier described the cutaneous hallmarks of chronic sarcoidosis as lupus pernio. Later, Caesar Boeck used the term sarkoid (sarcoid) for the first time when he assumed that these lesions were similar to sarcoma, but benign. Despite its long history, this disease remains enigmatic. Unidentified etiology and the multisystemic nature of the disease have made it more complex. The disease is not influenced by sex, although it is more common in adults of African-American or Scandinavian descent.
Despite the still unknown etiology, it is currently accepted that several antigens can cause sarcoidosis, in addition to a genetic predisposition related to the regulation of the immune response and environmental agents. Various factors, including infection, genetic predisposition, and environmental factors, are involved in the pathology of the disease. Exposures to insecticides, herbicides, bioaerosols, and agricultural employment are also associated with an increased risk.
The highest prevalence of sarcoidosis is found in Sweden (121/100,000 population), while Spain has the lowest rates in the region. In the US, the annual incidence rate is 10.9/100,000 population. In Asian countries, the disease is rarer; the prevalence of the disease in Japan is 1-2 cases/100,000 inhabitants. In Latin America, there are few studies on the prevalence of the disease, and, in Brazil, the incidence is estimated at 10/100,000 inhabitants.
Breast cancer is currently the neoplasm that most affects the female sex, and is configured as the cancer with the highest mortality rate in women on the planet. Breast carcinoma includes a heterogeneous collection of subtypes with histological variations, clinical presentations, treatment responses and diverse outcomes.
The disease is one of the few tumor types in which molecular classification has successfully been used for the design of individualized therapies, leading to significant improvements in disease-specific survival. Based on comprehensive gene expression profiling, breast tumors are classified into at least three major subtypes: luminal, human epidermal growth factor receptor 2 (HER-2) positive, and basal like. Each of these subtypes has different risk factors for incidence, response to treatment, risk of disease progression, and preferential organ sites of metastases.
Breast cancer has the potential for lymph node dissemination, mainly to axillary lymph nodes and/or lymph nodes of the internal mammary chain, in the thoracic region. In addition, all breast cancers have the potential for hematogenous spread to distant organs, such as the lung, liver, bones, and brain. The risk of lymph node and/or hematogenous metastases varies according to the subtype of breast cancer and time of disease progression.
The treatment of breast cancer is defined after staging, that is, defining the stage in which the disease is found. In addition, it is essential to know the subtype of the disease. In general, through the result of the pathology, including immunohistochemistry, it is possible to define the subtype of breast cancer. After staging and defining the tumor characteristics, it is possible to define the best treatment strategies, which may or may not include neoadjuvant chemotherapy, radiotherapy and/or hormone therapy.
Although the diagnosis of sarcoidosis in patients with breast cancer is uncommon, it is suspected that granulomatous disease is underdiagnosed in patients with malignant neoplasms, including breast cancer.
Kochoyan et al. (2016)
Data from Chen et al. (2015)
A similar pathogenesis between the two diseases is suggested by the shared characteristics. Sarcoidosis usually presents in the lungs and is often accompanied by mediastinal or hilar lymphadenopathy. One of the most frequent extrapulmonary manifestations is peripheral lymph node involvement, reportedly found in 8-15% of patients. The possibility of axillary lymph node involvement in sarcoidosis poses a diagnostic challenge in the differentiation of sarcoidosis from suspected breast mass metastasis to the lymphatic system and warrants nodal tissue sampling in all cases. Breast involvement is not common in sarcoidosis, and the diagnostic and physical findings resemble those of breast cancer. Sarcoidosis and breast masses have similar features upon palpation. Imaging is also of little value in differentiating breast involvement in sarcoidosis from breast malignancy.
As a result, this study examined a rare case and others previously present in the literature with the main objective of improving the patient’s evolution and understanding the mechanisms that must be involved in the pathogenesis of the development of sarcoidosis in patients with breast cancer.
The information contained in this work was obtained through a review of the medical record, interview with the patient, photographic record of the diagnostic methods to which the patient was submitted and a review of the literature. The study has no conflict of interest.
CLD, female, 40 years old, hypertensive, teacher, married, mother, born in Minas Gerais (Brazil), maternal aunt with breast cancer at 50 years old and paternal uncle with neck cancer at 50 years old. Denies smoking and social drinking. Menarche at 13 years old.
The patient was diagnosed in early 2020 with right breast cancer, multicentric, localized, luminal B, and clinical stage IIA. She was treated with neoadjuvant chemotherapy from March to July 2020 (AC X 4 followed by taxol X 12 cycles), followed by right mastectomy, with immediate reconstruction, right axillary dissection on 08/29/2020, pathologic stage ypT1ycN1a. It was followed by necrosis of the areolar-papillary complex (APC), requiring reoperation on 09/25/2020.
Due to the time elapsed between the end of the chemotherapy and the surgery, it was decided to carry out new staging tests before the patient proceeded to the sequential treatment, radiotherapy. In October 2020, the patient underwent CT scans of the chest and abdomen, which revealed the presence of numerous thoracic and abdominal lymphadenopathy, suspected of disease progression.
During the period from 11/24/2020 to 12/17/2020, the patient received treatment with ionizing radiation in plastron D and drainages with a dose of 4005cGy in 15 daily fractions, daily IMRT technique, in a 6MV linear accelerator.
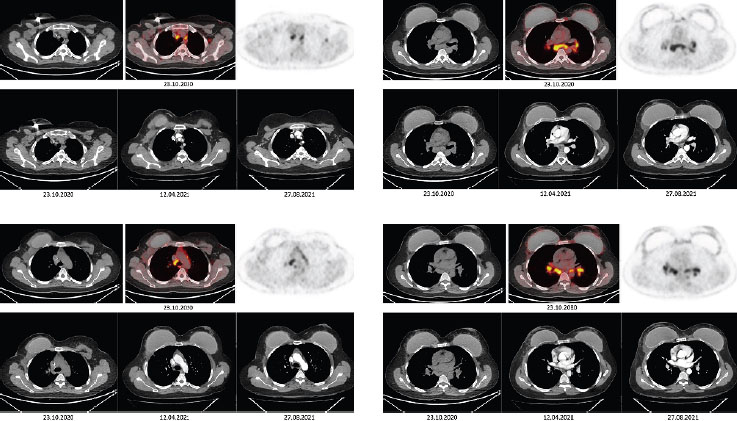
The PET/CT performed in 10/23/2020 (
Figure 1 Computed tomography + PET-SCAN.
Immunohistochemistry performed on 22/27/2020 resulted in: AE/AE3 negative, CD20 and CD3 positive in lymphocytes, CD30 Ki-1 (Ber-H2) positive in rare cells, CD68 (KP1) positive in histiocytes, Ki67 (MIB-1) positive in 10% of cells, BCG negative.
Immunohistochemical panel associated with histological aspects of chronic non-necrotizing granulomatous lymphadenitis with well-formed granulomas and multinucleated histiocytes.
On biopsy, sarcoidosis was diagnosed. The patient remains without recurrence signs, maintaining zoladex and continues to be followed up with pulmonology.
Several case reports and studies conducted over the past 4 decades have described the association between malignancy and sarcoidosis, but no definite causal relationship has been identified.
Some studies have reported that an unidentified antigen processed by activated macrophages instigates an immune response regulated by T-cells and macrophages. These activated cells discharge various mediators, including cytokines, chemokines, and reactive oxygen species that may be involved in the progression of the illness.
Clinically, patients could be asymptomatic like our patient, and diagnosis can be made on chest radiograph, with the most common finding being bilateral hilar lymphadenopathy (85%). Due to the diversity of the clinical picture, the diagnosis of sarcoidosis must be consolidated after excluding other possible diseases, especially those of infectious origin.
Often, however, patients present with respiratory symptoms, weight loss, and fever. Most cases have a self-limiting course, but some patients develop progressive disease or fibrosis. Sarcoidosis has been known to imitate other malignant neoplasms and has been described after treatment of other tumors, including lung cancer, Hodgkin’s disease, testicular cancer, osteosarcoma, melanoma, colorectal cancer, and thyroid cancer. However, there have only been rare case reports of sarcoidosis mimicking breast cancer.
The occurrence of lymphoma after the onset of sarcoidosis is called sarcoidosis- lymphoma syndrome and is more closely related to non-Hodgkin’s lymphoma. The syndrome was first described by Brincker et al. (1986)
Sarcoidosis can occur before, during or after cancer. According to a study by Arish et al. (2017)
In cases of simultaneous sarcoidosis and malignancies, the functions of FDG-PET/CT are further limited because tumor and granulomatous tissue both uptake fluorodeoxyglucose. The maximal standardized uptake value (SUV) in patients with malignancies is significantly higher than in patients with benign diseases. Nevertheless, in patients with granulomatous processes, the maximal SUV is similar to that in patients with malignant diseases. Therefore, FDG-PET/CT scan may only be an additional diagnostic tool used to assess the extent of disease spread without differentiation between malignant and granulomatous disorders; this tool could also create diagnostic difficulties and misunderstandings in patients with such simultaneous comorbidities. Only histological verification could accurately describe the nature of the disease.
A study of Grados et al. (2015)
Sarcoidosis must be considered in the differential diagnosis of patients with a history of malignancy who have developed lymphadenopathy or other lesions on positron emission tomography computerized tomography.
The Schweitzer et al. (2017)
The high rate of sarcoid-like reaction among breast cancer patients in the literature highlights the importance of a thorough clinical investigation when sarcoid-like granulomas are found in the context of known breast cancer to detect the possible presence of sarcoidosis. Furthermore, sarcoid-like reaction in regional lymph nodes can conceal a metastasis and needs to be carefully evaluated.
The study of Lower et al. (2001)
Therefore, although the presence of both sarcoidosis and breast cancer in the same patient is rare, the differentiation between the diseases is justified, being difficult clinically and radiologically. If suspected, the association requires histological study.
In conclusion, this case report alerts to the importance of observing the natural history of breast cancer, capacity for lymphatic dissemination. Furthermore, pay attention to possible differential diagnoses, such as granulomatous diseases. Excisional biopsy remains the most appropriate test for diagnostic confirmation, adequate management, and treatment.
| AGAD | Collection and assembly of data, Conception and design, Data analysis and interpretation, Manuscript writing |
| ACSMF | Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Provision of study materials or patient |
| LDVCPA | Conception and design, Final approval of manuscript, Manuscript writing |
| FDST | Conception and design, Final approval of manuscript |
| WFB | Conception and design, Data analysis and interpretation, Manuscript writing |
| EMP | Data analysis and interpretation, Manuscript writing |
| TGAD | Conception and design, Data analysis and interpretation, Manuscript writing |
| GANS | Data analysis and interpretation, Manuscript writing |
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Jain, R and Yadav, D and Puranik, N and Guleria, R and Jin, JO. Sarcoidosis: causes, diagnosis, clinical features, and treatments. J Clin Med [online]. 2020, vol. 9, p. 1081. https://doi.org/10.3390/jcm9041081 Ver referência
2. Ravaglia, C and Gurioli, C and Casoni, GL and Romagnoli, M and Tomassetti, S and Gurioli, C. Sarcoid-like lesion is a frequent benign cause of lymphadenopathy in neoplastic patients. Eur Respir J [online]. 2013, vol. 41, p. 754-5.
3. Ungprasert, P and Ryu, JH and Matteson, EL. Clinical manifestations, diagnosis, and treatment of sarcoidosis. Mayo Clin Proc Innov Qual Outcomes [online]. 2019, vol. 3, p. 358-75. https://doi.org/10.1016/j.mayocpiqo.2019.04.006 Ver referência
4. Jain, R and Yadav, D and Puranik, N and Guleria, R and Jin, JO. Sarcoidosis: causes, diagnosis, clinical features, and treatments. J Clin Med [online]. 2020, vol. 9, p. 1081. https://doi.org/10.3390/jcm9041081 Ver referência
5. El Jammal, T and Pavic, M and Gerfaud-Valentin, M and Jamilloux, Y and Sève, P. Sarcoidosis and cancer: a complex relationship. Front Med (Lausanne) [online]. 2020, vol. 7, p. 594118. https://doi.org/10.3389/fmed.2020.594118 Ver referência
6. Lemos-Silva, V and Araújo, PB and Lopes, C and Rufino, R and Costa, CH. Características epidemiológicas de pacientes com sarcoidose na cidade do Rio de Janeiro. J Bras Pneumol [online]. 2011, vol. 37, p. 438-45. https://doi.org/10.1590/S1806-37132011000400005 Ver referência
7. Rosmaninho, A and Velho, G and Caetano, M and Selores, M. Breast cancer: 2 case reports. An Bras Dermatol [online]. 2012, vol. 87, p. 123-6.
8. Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA). Controle do câncer de mama: conceito e magnitude [Internet]. INCA, 2022.
9. Poliak, C. Heterogeneity in breast cancer. J Clin Invest [online]. 2011, vol. 121, p. 3786-8. https://doi.org/10.1172/JCI60534 Ver referência
10. Klevesath, MB and Pantel, K and Agbaje, O and Provenzano, E and Wishart, GC and Gough, P. Patterns of metastatic spread in early breast cancer. Breast [online]. 2013, vol. 22, p. 449-54. https://doi.org/10.1016/j.breast.2013.04.017 Ver referência
11. Chen, J and Carter, R and Maoz, D and Tobar, A and Sharon, E and Greif, F. Breast cancer and sarcoidosis: case series and review of the literature. Breast Care (Basel) [online]. 2015, vol. 10, p. 137-40. https://doi.org/10.1159/000381324 Ver referência
12. Kochoyan, T and Akhmedov, M and Shabanov, A and Terekhov, I. Sarcoidosis imitating breast cancer metastasis: a case report and literature review. Cancer Biol Med [online]. 2016, vol. 13, p. 396-8. https://doi.org/10.20892/j.issn.2095-3941.2016.0038 Ver referência
13. Baughman, RP and Teirstein, AS and Judson, MA and Rossman, MD and Yeager, H and Bresnitz, Eda. Case Control Etiologic Study of Sarcoidosis (ACCESS) research group. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med [online]. 2001, vol. 164, p. 1885-9. https://doi.org/10.1164/ajrccm.164.10.2104046 Ver referência
14. Grados, A and Ebbo, M and Bernit, E and Veit, V and Mazodier, K and Jean, R. Sarcoidosis occurring after solid cancer: a nonfortuitous association: report of 12 cases and review of the literature. Medicine (Baltimore) [online]. 2015, vol. 94, p. e928. https://doi.org/10.1097/MD.0000000000000928 Ver referência
15. Arish, N and Kuint, R and Sapir, E and Levy, L and Abutbul, A and Fridlender, Z. Characteristics of sarcoidosis in patients with previous malignancy: causality or coincidence?. Respiration [online]. 2017, vol. 93, p. 247-52. https://doi.org/10.1159/000455877 Ver referência
16. Tolaney, SM and Colson, YL and Gill, RR and Schulte, S and Duggan, MM and Schulman, LN. Sarcoidosis mimicking metastatic breast cancer. Clin Breast Cancer [online]. 2007, vol. 7, p. 804-10. https://doi.org/10.3816/CBC.2007.n.044 Ver referência
17. Brincker, H. The sarcoidosis-lymphoma syndrome. Br J Cancer [online]. 1986, vol. 54, p. 467-73. https://doi.org/10.1038/bjc.1986.199 Ver referência
18. Schweitzer, MD and Salamo, O and Holt, G and Donna, E and Mirsaeidi, M. Sarcoidosis on set after breast cancer, a potential association. Eur J Intern Med [online]. 2017, vol. 44, p. E11-E12. https://doi.org/10.1016/j.ejim.2017.08.006 Ver referência
19. Lower, EE and Hawkins, HH and Baughman, RP. Breast disease in sarcoidosis. Sarcoidosis, vasculitis, and diffuse lung diseases. J WASOG [online]. 2001, vol. 18, p. 301-6.
Dados de acesso insuficientes para visualização no mapa.