“Tumor-to-tumor metastasis” is a rare phenomenon, described in few reports in the literature, in which a tumor metastasizes and its growth is established in another tumor.
The patient was an 89-year-old male with previous low charge of smoking (less than 10 years-package) and who had been diagnosed in 2005 with adenocarcinoma of the prostate, graded at Gleason 8 (4+4), and underwent radical prostatectomy the same year. In 2009, biochemical and local relapse were detected and he was treated with salvage radiotherapy combined with hormone therapy. In July 2018, biochemical relapse was detected again with PSA level raising from 2.79 to 3.84 plus lung lesions in a castrationresistant scenario and it was started abiraterone acetate as systemic treatment. The68 Ga-PSMA PET-CT imaging was used for restaging, revealing anomalous tracer concentrations in the prostatic space, with an SUV of 2.6; in a left peribronchial mass, with an SUV of 8.0; and in multiple bilateral pulmonary nodules with SUVs ranging from 2.8 to 4.4. (
A biopsy was then performed on one of the nodules in the patient's left lung (
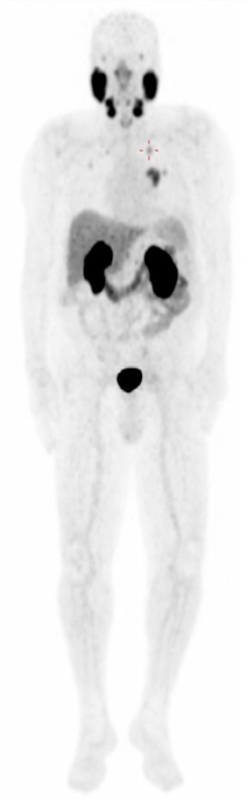
Image 1. Full body image at maximum intensity projection (MIP) from the PET-CT examination, demonstrating areas of abnormal 68Ga-PSMA concentration in the lungs, especially the left lung nodule that was biopsied (cross).
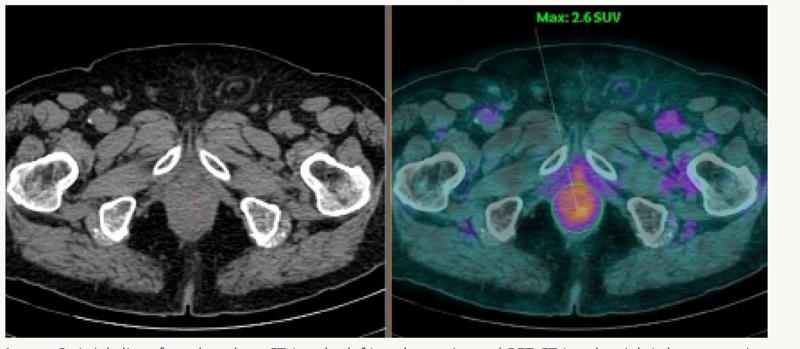
Image 2. Axial slices from low dose CT (on the left) and coregistered PET-CT (on the right) demonstrating 68Ga-PSMA concentrations in the prostate space with an SUV of 2.6.
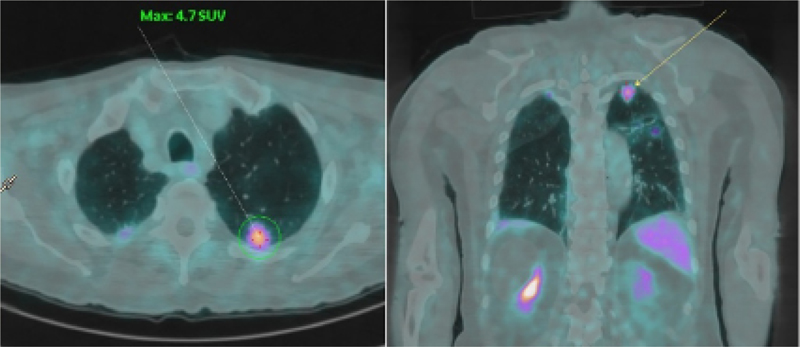
Image 3. Coregistered PET-CT axial slices (on the left) and coronal slices (on the right) demonstrating 68Ga-PSMA concentrations in the left lung nodule (which was later biopsied) with an SUV of 4.7.
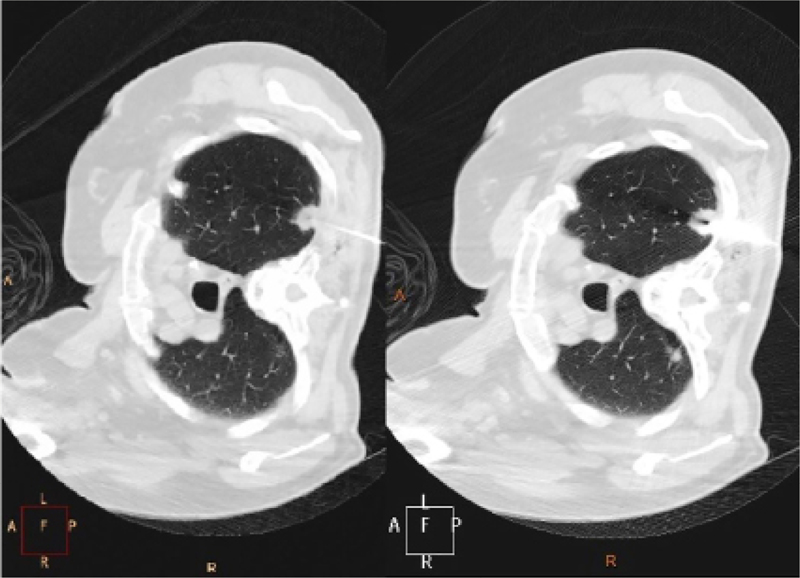
Image 4. Axial computed tomography slices guiding the biopsy of left lung nodule using a large caliber needle with a Coaxial 17 / 18 G system and automatic trigger device.
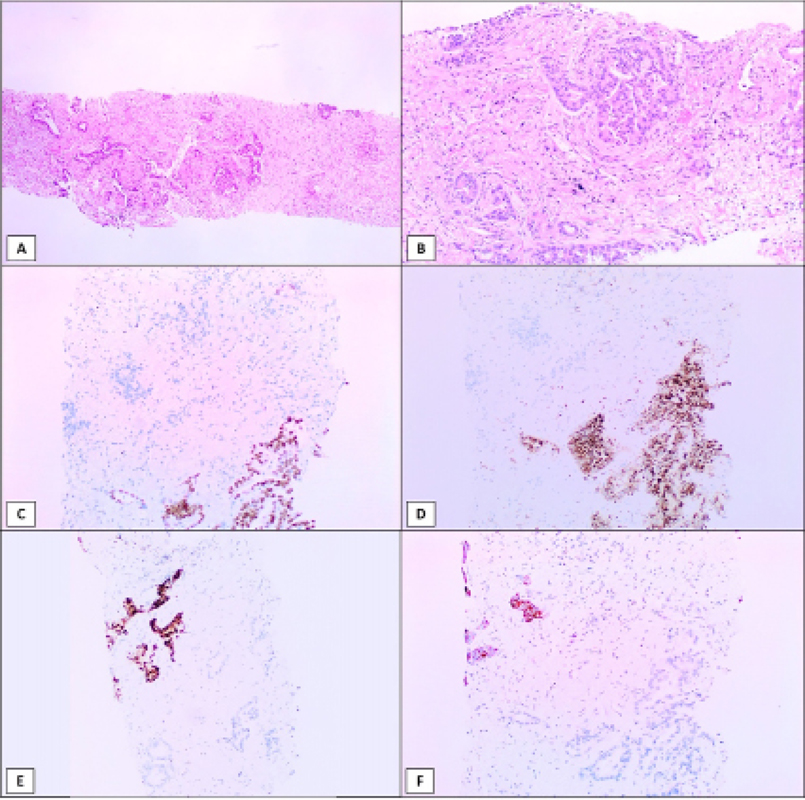
Image 5. A) Biopsy fragments showing an infiltrating adenocarcinoma (H&E, 40x). B) The tumor was composed of acinar and cribriform malignant glands (H&E, 100x). Most of the tumor cells were positive for TTF-1 (C, 100x) and Napsin-A (D, 100x), but a small group of cells were negative for both markers (upper left corner). In contrast, those glands were positive for NKX3.1 (E, 100x) and PSA (F, 100x), mirroring the images from the lung markers and confirming the diagnosis of a metastatic prostatic adenocarcinoma inside a primary lung tumor.
“Tumor-to-tumor metastasis” is a phenomenon that is still considered rare in the literature and, according to Campbell et al., certain criteria must be met for diagnosis: more than one primary tumor; the recipient tumor must be a true benign or malignant neoplasm; metastatic growth must be established in the recipient tumor; and tumors that have metastasized to the lymphatic system are excluded.
Just as there are differences in metastatic potential between different tumors, there are also differences in their capacity to host metastases. According to the literature, clear cell renal cell carcinoma is the most common metastasis recipient tumor, followed by sarcoma, meningioma, and thyroid cancer. Lung carcinoma is the most common donor tumor (40-50% of cases), followed by breast, gastrointestinal tract, prostate, and thyroid carcinomas.
Lung carcinoma as recipient of tumor metastasis, as described in this case, is one of the rarest presentations. The most common donor tumor for this recipient is papillary thyroid carcinoma. In addition to not affording a rich network of blood vessels, they tend to grow rapidly and do not provide a suitable host environment.
Applications for68 Ga-PSMA PET-CT continue to extend beyond prostate cancer. Expression of PSMA has been demonstrated by immunohistochemistry in neovasculature of a range of lung tumors that exhibited affinity with68 Ga-PSMA. However, this analytical method is not yet able to discriminate reliably between pulmonary lesions in patients with prostate cancer. Primary lung tumors have demonstrated similar tracer concentrations to prostatic metastases, creating a diagnostic challenge that, in the majority of cases, still requires histological confirmation.
Ethical Considerations: This case report received approval from the institution's Research Ethics Committee.
Conflict of Interest Statement: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.