In Brazil, lung cancer is a public health problem given its high incidence, morbidity and mortality. The estimative of new cases from the Brazilian NCI is 18.740 for men and 12.530 for women in 2018
Clinicopathologic aspects, such as performance status (PS), comorbidities, histopathologic subtypes and oncogenic driver mutations, are crucial information to guide the initial treatment. Epidermal growth factor receptor gene ( EGFR ) and KRAS are the most known activating driver mutations, considered biomarkers predictive of response to tyrosine kinase inhibitors (TKIs), a class of drugs that confers better survival than chemotherapy and less toxicity
Unfortunately, in Brazilian public health, the access to these new technologies is limited by cost, once the reimbursement from the Health Ministry is about half the cost of TKIs treatment for each NSCLC patient
This study aims to analyze frequencies of EGFR and KRAS mutations in a NSCLC population treated at a public comprehensive cancer center in Brazil, and to correlate the tumor genotypes with demographic and clinical-pathologic features. We conducted a retrospective study of all treated patients referred to the Erasto Gäertner Cancer Hospital from January 2004 to December 2017, diagnosed as metastatic or recurrent NSCLC, according to the American Joint Committee on Cancer (AJCC) staging manual, version 7. The Erasto Gäertner Hospital at Curitiba, Paraná State, Brazil, provides cancer care to public health system and is a reference for the Southern Brazilian population. Ethics approval for the study was obtained from the local research ethics board under the inscription number 2320. The primary endpoint was to characterize EGFR and KRAS mutations in metastatic or recurrent NSCLC, suitable for palliative chemotherapy treatment. Secondary endpoints were to correlate EGFR and KRAS mutational status with individual demographic and clinical- pathologic features, and with relevant clinical endpoints (best treatment response and overall survival). The key exclusion criteria were defined with non-treated patients and cases in which formalin-fixed, paraffin-embedded tissue (FFPET) were not available or the genetic material was not viable for analyses.
By a retrospective chart review, we collected the patient's baseline and tumor characteristics, such as age, sex, ethnicity, comorbidities, smoking status, metastasis sites and histological subtypes. Ethnicity was classified as white, black or other. Registered comorbidities were chronic obstructive pulmonary disease (COPD), systemic arterial hypertension (SAH), diabetes, hypothyroidism, and second primary tumor and, for statistical analysis, they were grouped in “absent” (no comorbidity), “one or two” and “three or four” comorbidities subgroups. For smoking status, patients were classified as never smoker, previous or current smoker. The pack-years were calculated by multiplying the number of packs of cigarettes smoked per day by the number of years the person has smoked. Metastatic sites were grouped by prognostic criteria in “lung and/or pleural metastasis only” (excluding other concomitant sites), “visceral” (i.e. liver, adrenal, lymph nodes), “central nervous system (CNS)” (with or without involvement of other sites) and “bones only” (excluding other concomitant sites). The histological diagnosis was based on the 2014 World Health Organization (WHO) classification as adenocarcinoma, squamous cell carcinoma (SCC) and undifferentiated (NOS) carcinomas. The PS was estimated according to the Eastern Cooperative Oncology Group (ECOG) classification. Systemic treatment protocols, including the type of chemotherapy, were collected. Outcomes including overall survival (OS), from the time of diagnosis to death, and progression-free survival (PFS) were recorded. The duration of PFS was defined as the time from diagnosis until the date of objective disease progression or death in the absence of progression, regardless of whether the patient had received another anticancer therapy before progression.
2592 NSCLC patients were referred to our hospital from 2004-2017 and 1398 were at an advanced or recurrent disease. Only 587 were able to perform chemotherapy treatment, and 273 of those have suitable FFPET for DNA extraction and analysis. Tumor samples from primary tumor or metastatic site biopsy or pulmonary surgery resection were collected in FFPET from our Pathology Service arquives and analyzed for mutational status at the laboratory Mantis Diagnósticos Avançados, in Curitiba, Paraná State, Brazil. Reasons for not inclusions were depleted and tiny amount of tumor tissue material, and scarce or low quality DNA extracted from tumor samples interfering with the analysis. Procedures for tumor tissue microdissection and DNA extraction were done according established protocols. In summary, local pathologists defined the area of the tumor sample to be selected by optical microscopy in histological sections (stained by hematoxylineosin), and a number of tissue sections of 5-10 micra corresponding to the blocks were used for DNA extractions with the QIAmp® DNA Mini Kit (Qiagen; California, USA). Quantitative assay for KRAS gene point mutation in codons 12, 13 (exon 2) and 61 (exon 3) was performed with KRAS Pyro ® Kit (QIAGEN). The EGFR Pyro ® Kit (QIAGEN) was used for quantitative assay for EGFR point mutations in codons 719 (exon 18), 768 (exon 20), 790 (exon 20), 856-861 (exon 21) and deletion of exon 19 (del19). The analysis and identification of existing mutations in these codons were performed using the Software PyroMarK ® (QIAGEN Germany).
The quantitative variables were described by average, standard deviation, median, and amplitude. The comparison of two groups defined for the EGFR or KRAS mutation, in respect to the quantitative variables, was made using t-Student test for independent samples or non-parametric MannWhitney test. Categorical variables were analyzed considering Fisher test or Chi-Square test. Survival was described by Kaplan-Meier method and Cox regression model was used to determine mortality predictors. We excluded from the survival analysis the two outlier cases treated with gefitinib. A p-value with less than 0.05 was considered statistically significant. Statistical analyses were performed using the computational program Stata/SE v.14.1. StataCorp LP, USA.
Considering the 587 patients who were able to perform chemotherapy, 273 had viable FFPET for DNA extraction and a n a l y s e s and those were included in this article. The clinical characteristics of adenocarcinoma and SCC cases at baseline are presented in
| Charactcristics | Adeno* n= 162 | SCC* n=92 | Undiffer. NOS* n=19 | Total n=273 | % | |
|---|---|---|---|---|---|---|
| Median age, years |
|
|
| 60 |
|
|
| Min-Max |
|
|
| 30-84 |
|
|
| Ethnicity White | 153 | 84 | 18 | 255 | 93.4 | - |
| Black | 6 | 3 | 0 | 9 | 3.3 |
|
| Other | 3 | 4 | 1 | 8 | 2.9 |
|
| Gcnder Male | 74 | 58 | 12 | 144 | 52.7 | 0.018 |
| Female | 88 | 34 | 7 | 129 | 47.3 |
|
| Comorbidities Absent | 65 | 33 | 8 | 106 | 38.8 | 0.955 |
| One or two | 87 | 52 | 10 | 149 | 54.8 |
|
| Three or four | 10 | 7 | 1 | 18 | 6.6 |
|
| Smoking status Never smoked | 46 | 4 | 3 | 53 | 19.4 | <0.00001 |
| Previous/smoker | 102 | 86 | 13 | 201 | 73.6 |
|
| Unknown | 14 | 2 | 3 | 19 | 7.0 |
|
| Pack years, median |
|
|
| 40 |
|
|
| Min-Max |
|
|
| 0,5 - 224 |
|
|
| Performance status 0 or 1 | 104 | 52 | 10 | 166 | 60.8 | 0.162 |
| 2 | 38 | 31 | 4 | 73 | 26.7 |
|
| 3 or 4 | 9 | 7 | 3 | 19 | 7,0 |
|
| Unknown | 11 | 2 | 2 | 15 | 5.5 |
|
| Metastases sites Lung/Pleural (only) | 46 | 41 | 8 | 95 | 34.8 | 0.004 |
| Visceral | 58 | 34 | 9 | 101 | 37.0 |
|
| CNS | 41 | 6 | 2 | 49 | 17.9 |
|
| Bones (only) | 23 | 10 | 1 | 34 | 12.5 |
|
For one patient with SCC ethnicity is unknown.* Adeno: adenocarcinoma; SCC: undifferentiated carcinomas, NOS.
Chi-square test, p<0.05
In our population, median age was 60. White ethnicity was 93.4%, and male gender was 52.7%. The majority has at least one comorbidity (54.8%), and the most frequent was chronic obstructive pulmonary disease (COPD). Adenocarcinoma was diagnosed in 162 (59.3%), SCC in 92 (33.7%) and undifferentiated carcinomas in 19 (7.0%) patients. Previous or current smoker status was recorded in 201 cases (73.6%). Smoking was more frequent in SCC (93.5%) than adenocarcinoma (63.0%) [p value = 0.0001]. PS was 0 or 1 in 166 (60.8%) cases. CNS metastasis at diagnosis was detected in 49 (17.9%) patients for symptomatic patients based on clinical symptoms or neurological findings, since CNS scanning was not routine in our service. There is an association between gender, smoking status and metastases sites with histological subtypes (p=0.018; p<0.00001; p=0.004, respectively). The most common chemotherapy treatment scheme at first line therapy was a platinum-doublet (95.2%); docetaxel for second line regimen (63.9%); and 2 cases received Gefitinib as second line therapy (2.4%) (
Of the 127 tumors tested for EGFR, 20 resulted positive for any EGFR mutation (15.7%). Among the 121 available samples for KRAS analysis (since six samples were depleted after EGFR analysis), KRAS mutation was detected in 26 (21.5%). In only one tumor sample, concomitance of EGFR (G719A) and KRAS (G12C) mutations could be detected. Compared with wildtype tumors (WT), EGFR mutated tumors did not differ in the median age at diagnosis (60 years for WT vs. 57 years, p=0.513) or in those mutated for KRAS (60 years WT vs. 59.5 years, p=0.343). We also did not found any statistical difference for gender, smoking status, pack- years, histological subtypes (adenocarcinoma or SCC) or metastatic sites between mutated and wild type subgroups for either EGFR or KRAS (
|
| Total | |
|---|---|---|
| Characteristics | n | % |
| First Line Chemotherapy Platinum-doublet | 256 | 95.2 |
| Other | 13 | 4.8 |
| Second Line Chemotherapy Platinum-doublet | 20 | 24.0 |
| Docetaxel | 53 | 63.9 |
| Gefitinib | 2 | 2.4 |
| Others | 8 | 9.7 |
Platinum-doublet were cisplatin or carboplatin and paclitaxel or etoposide or gemcitabine
Others were monotherapy scheme: gemcitabine, vinorelbine, etoposide
|
| EGFR | p -value | KRAS |
| p -value | ||
|---|---|---|---|---|---|---|---|
| Characteristics | mut/wt (%mut/wt) |
| mut/wt (%mut/wt) |
|
| ||
| Gender Male | 10/57 (14.9/85.1) | 0.812 | 13/51 (20.3/79.7) |
| 0.826 | ||
| Female | 10/50(16. 7/83.3) |
| 13/44 (22.8/77.2) |
|
| ||
| Smoking status Never smoked | 6/21 (23.0/78.0) | 0.234 | 8/18 (30.8/69.2) |
| 0.276 | ||
| Previous/smoker | 12/81 (13.0/87.0) |
| 16/68(19.0/81.0) |
|
| ||
| Histology Adenocarcinoma | 12/63 (16.0/84.0) | 0.986 | 16/55 (22.5/77.5) |
| 0.517 | ||
| scc | 6/34(15.0/85.0) |
| 6/31 (16.2/83.8) |
|
| ||
| Others | 2/10(16.7/83.3) |
| 4/9 (30.8/69.2) |
|
| ||
| Metastasis sites Lung/Pleural (only) | 6/33 (15.4/84.6) | 0.229 | 7/32 (17.9/82.1) |
| 0.473 | ||
| Visceral | 7/45 (13.5/86.5) |
| 9/40(18.4/81.6) |
|
| ||
| SNC | 2/19(9.5/90.5) |
| 5/14 (26.3/73.7) |
|
| ||
| Bones (only) | 5/10(33.3/66.7) |
| 5/9 (35.7/64.3) |
|
| ||
Chi-square test, p<0.05. EGFR or KRASmut: mutated; EGFR or KRASwt: wild-type.
Others: undifferentiated carcinomas, NOS.
Among mutated tumors for EGFR or KRAS, the most common metastatic site was visceral (35.0%) in both groups. Others metastatic sites observed in EGFR and KRAS mutated tumors were lung or pleural (30.0% and 27.0%, respectively), bones (25.0% and 19.0%, respectively), and CNS (10.0% and 19.0%, respectively). Although there was an expressive prevalence of CNS metastasis in KRAS mutated tumors compared with EGFR, frequencies did not reach statistical significance for any of those sites in both EGFR and KRAS mutated groups (p=0.838).
In our population, the most frequent position of EGFR mutations was in exon 19 (n=9, 45.0%). Other EGFR mutations were found in exon 21 (n=7, 35.0%), exon 20 (n=3, 15.0%) and exon 18 (n=1, 5.0%). In details, the mutations detected in exon 19 were del E746-A750 (n=5), del L747-P753 (insS) (n=1), del L747- A750 (insP) (n=2), and a complex deletion in-frame c.2237_2251 del15 (p.E746_ T751>A) (n=1). In exon 21, the mutation L858R (n=5) and L861Q (n=2). In exon 20, S768I (n=3); and exon 18, G719A (n=1). For KRAS, the mutations detected on available samples were G12V (n=8, 30.8%), G12C (n=8, 30.8%), G12S (n=6, 23.1%) and G12D (n=4, 15.4%). The distribution of EGFR kinase domain mutations according to clinical and pathological characteristics is described in
|
|
| EGFRmut |
|
|---|---|---|---|
|
| Exon 18/21 | Exon 19 | Exon 20 |
| Gender Male | 3 | 4 | 3 |
| Female | 5 | 5 | 0 |
| Smoking status Never smoked | 5 | 6 | 3 |
| Previous/smoker | 3 | 3 | 0 |
| Histology Adenocarcinoma | 5 | 7 | 0 |
| scc | 3 | 1 | 2 |
| Metastasis sites Lung/Pleural (only) | 2 | 3 | 1 |
| Visceral | 4 | 2 | 1 |
| CNS | 1 | 1 | 0 |
| Bones (only) | 1 | 3 | 1 |
A statistical test could not be applied because of low-frequency cases in exon 20.
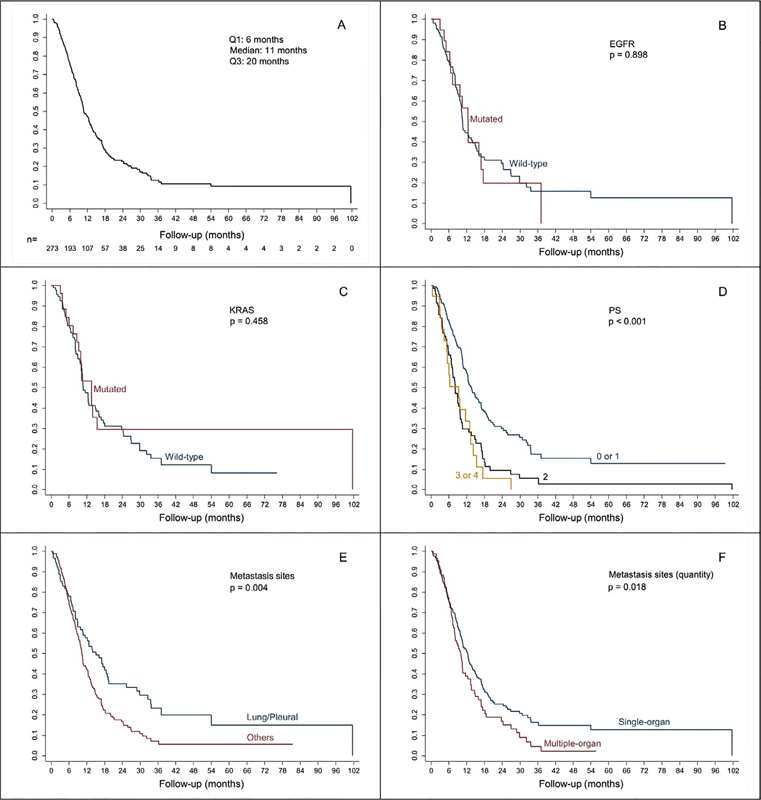
The median overall survival of the entire cohort was 11 months, and no statistical difference in survival was detected between EGFR mutated versus WT (12.4 months vs. 10.6 months; p=0.898), or KRAS mutated versus WT (12.1 months vs. 10.7 months; p=0.458). Some clinical variables significantly interfered with survival: PS 0 or 1 had more favorable prognosis than PS 2 or more (p<0.001); and lung or pleural metastatic sites had better outcomes than visceral, CNS and bones (p=0.004). Neither comorbidities number nor histological subtypes (adenocarcinoma or SCC) influenced overall survival. However, patients that had more than one metastatic site had worst prognosis compared with only one- metastatic site tumors. Kaplan-Meier curves are represented in
Oncogenic drivers identification has redefined how we treat advanced NSCLC. Chemotherapy is no longer a standard therapy if a patient has an actionable driver mutation. Patients with a genotype-directed therapy have a decreased risk of death compared with patients with any oncogenic driver who did not receive genotype-directed therapy (HR, 0.69 [95% CI, 0.53-0.9], p=0.006)
In Brazil, EGFR mutation frequency ranges from 20 to 30%
In the large LCMC study
Ethnicity influences EGFR and KRAS mutation frequency and treatment response. In LCMC
According to LCMC
In LCMC
Figure 1 Overall survival and survival according to EGFR, KRAS and clinicai presentation
Kaplan-Meier survival curves and Cox regression models. A. Overall survival; B. EGFR mutated versus EGFR wild-type; C. KRAS mutated versus KRAS wild-type; D. Performance status 0 and 1 versus PS 2 or more; E. Lung/pleural metastasis sites versus other (visceral, CNS, bones); F. One metastasis site versus two or more metastases sites.
They also found that KRAS mutation was correlated with bone metastasis. Retrospective data show that patients with intrapulmonary metastasis have a higher frequency of KRAS mutation
In this study, the survival was calculated between prognostic variables. Regardless mutational status, one metastasis site versus multiple metastasis sites is considered a known favorable prognostic factor, especially if it is resectable
Another prognostic variable is PS. Initial PS evaluation is crucial for treatment choice and it affects overall survival. In our study, we reviewed only treated patients, and 60.8% of them were PS 0 or 1. This subgroup showed greater survival compared with PS 2, 3 or 4 patients (p<0.001).
Our median survival was 11 months and is similar with others survival data in Brazilian studies
Only in mid-2010, with the encouragement of pharmaceutical companies, molecular testing for advanced NSCLC adenocarcinoma started at our Institution, but public access to TKIs was still limited by costs. Thus, in our study, only two patients with EGFR mutation were treated w i t h Gefitinib, a firstgeneration EGFR TKI, in the second line treatment. These two cases were male patients, smokers, one with L858R mutation (exon 21) and one with E746-A750 mutation (exon 19). Both patients had the study longest survival rates (12.4 months and 37.1 months, respectively). This highlights the great benefit of TKI therapy in survival in NSCLC patients compared to standard chemotherapy
The best responses to TKI targeting EGFR are in individuals with exon 19 deletions
In our study, 45.0% of mutations detected in EGFR happen in exon 19 by distinct small deletions, including complex in-frame deletion p.E746_T751>A, first described here. Point mutations frequencies in exon 18 (G719A, n = 1) and exon 21 (L858R, n=5 e L861Q, n=2) were 40.0%, and 15.0% in exon 20 (all S768I). These findings are in agreement with frequencies in literature
This rare finding may be explained by intratumoral heterogenicity (by mutational events arising separately in at least two distinct clones), or because of two co-mutational events into a unique malignant cellular clone leading to EGFR pathway cooperative activation in both upstream and downstream of the RAS-RAF-MEK-MAPK signalingpathway. Unfortunately, we could not repeat the analysis in this case due insufficient tissue remaining. A recent study including 17.664 lung cancer patients detected 2 to 3 concomitant driver mutations in almost 1% of the cases. The most common co-mutations occurred again with EGFR in this large cohort were PIK3CA (n=28), KRAS (n=24), ALK (n=10), and BRAF (n=5) mutations
Recently in Brazil, government regulatory agency Agencia Nacional de Vigilância Sanitária (ANVISA) approved an oral third-generation irreversible EGFR TKI as front-line treatment for advanced NSCLC with EGFR exon 19 deletions or exon 21 L858R mutation. In the FLAURA study, a phase III randomized trial for advanced NSCLC
Our study has limitations because it was retrospective and we excluded a large number of cases because of scarce or depleted tissue material and because of insufficient quality (fragmentation) of DNA extracted from FFPET. Based on current international guidelines all advanced adenocarcinoma NSCLC should be tested for actionable drug targets ( EGFR, ALK, and ROS1 )
The analytical method sensitivity may also explain differences in EGFR mutational rates in literature. We choose pyrosequencing because of its sensitivity to detect a minimum of 5% mutated alleles. Recently, with the application of next generation sequencing (NGS) and other allele-specific-based assays, i.e. digital droplet polymerase chain reaction (ddPCR), sensitivity of much less than 1% have been feasible, allowing the screening of rare somatic mutated alleles in body fluids (plasma, urine) by liquid biopsy
Despite this fact, pyrosequencing is faster, requires less DNA, and is less complex in terms of assay design and technical setup than others techniques. It can determine not only known EGFR hotspots, including exon 19 deletions and codon 719 substitutions, but also new mutations, like complex in-frame deletion p.E746_T751>A. Ultimately, genetic laboratories must consider analytical sensitivity in their reports, mutational coverage and method limitations when evaluating EGFR mutation assays for adoption into the laboratory workflow. The small volume of viable tumor material for analysis demonstrates the importance of an excellent collection of tissue at the time of biopsy, storage, and the impact in sensitivity that liquid biopsy will bring in the next few years for molecular analysis of tumors.
Because the access of the SUS population to EGFR TKI was limited by cost, only two patients were treated with first generation TKI (Gefitinib). The absence of differences in NSCLC survival between the mutated and non-mutated EGFR groups treated with chemotherapy alone during a pre-TKI era suggests that they have similar biological behaviors, and that EGFR alone was not prognostic. Currently, in our hospital, we perform molecular analyzes (EGFR, ALK, PD-L1) in all patients with advanced NSCLC adenocarcinoma, in association with pharmaceutical companies, access to therapy with Gefitinib after detection of the EGFR mutation is provided by the hospital after negotiating spending with the drug.
We intend to evaluate in the future the impact of introducing EGFR TKI on our population overall survival. Considering that EGFR mutation frequency in our population was 15.7% and that in Brazilian literature mutated cases survival can vary from 30 to 60 months in best series
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.