Neuroendocrine tumors (NETs) are uncommon neoplasms. However, their incidence have been increasing over the past decades, with nowadays 5-7 cases per 100,000.
The rationale for treatment with TAE and TACE is based on the fact that liver metastases from NETs are hypervascular and derive most of their blood supply from the hepatic artery, whereas normal hepatocytes feed from the portal vein. TAE can be performed using lipiodol, polyvinyl alcohol (PVA), gel foam powder or bland microspheres. TACE has the same principles, but single-agent chemotherapy (doxorubicin, cisplatin, streptozocin) is added, followed by embolizing agents.
There is no evidence about whether TACE offers superior results when compared with TAE, or at least when treating patients with midgut NETs liver metastases, which are mostly chemo-resistant.
Importantly, given the absence of robust randomized trials demonstrating superiority of one technique over the other, both TAE and TACE are considered reasonable approaches for patients with hepatic-predominant disease not suitable for R0 surgical resection. Because targeted agents are not widely available in Brazil due to lack of reimbursement by the public system, TAE/TACE are often utilized to treat NET patients with liver metastases. However, we are unaware of studies on liver embolization from Brazil. Thus, our study aimed to evaluate the radiographic, biologic, and clinical response, safety of TAE and TACE in patients with NETs presenting with hepatic metastases treated at two Brazilian cancer centers.
We performed a retrospective study in patients presenting with metastatic NETs treated with TAE and/or TACE at AC Camargo Cancer Center and Cancer of Institute of Sao Paulo. The selection of patients was made by convenience sampling from a database of carcinoid syndrome and pancreatic NETs. Eligible patients had histological diagnosis of neuroendocrine tumor of any origin, unresectable and measurable metastatic hepatic disease, and underwent at least one procedure of TAE or TACE. The first procedure of embolization was performed in June 2005. The following clinical data were collected retrospectively from electronic medical records: sex, age at the time of first embolization procedure, cell differentiation, ki67 index, metastatic sites, and treatment outcomes. Hepatic tumor burden was stratified by <50 and >50% liver volume involvement using simple visual estimate.
The primary endpoints were tumor response and hepatic progression free survival (HPFS), which were calculated from the date of first embolization. Secondary endpoints were overall survival (OS) and toxicity assessment. This study was conducted in accordance with the protocol, Good Clinical Practice guidelines of the International Conference on Harmonization (ICH GCP), applicable local laws and regulatory requirements.
Embolization therapies included TAE and TACE. The choice between TAE and TACE was based on the decision of the referring radiologist and the patient's oncologist. The technique, materials and number of therapy sessions were at the discretion of the treating interventional radiologist. TAE was performed using microspheres (Embospheres, Merit Medical, Utah, USA; Embozene, CeloNova, TX, USA) or polyvinyl alcohol (PVA) in sizes ranging from <150 to 500um. TACE was performed using lipiodol and doxorubicin. Technical details have been described previously.
All relevant images were retrieved from radiology picture archiving systems to analyze hepatic tumor burden. Images included magnetic resonance (MRI) and computed tomography (CT) scans of the abdomen. Radiological response rates (any radiological tumor shrinkage) were retrospectively determined according to radiological reports. Images were performed every 1-3 months after the procedure. In functioning tumors, dosage of 24 hours urinary 5-HIAA was collected 1-3 months before and after the embolization procedure.
Baseline characteristics were compared between TAE e TACE groups using Chi-square test and Fisher's exact test for discrete variables, ANOVA methods for continuous variables, and Wilcoxon and Kruskal-Wallis methods for non-normal continuous variables. Survival curves were calculated by the Kaplan-Meier method. HPFS was defined as the time from the start of TAE or TACE until the date of progression, based on radiological reports, in liver or death. OS was defined as the time from the start of TAE or TACE until the date of death or last follow-up. All analyses were performed using the SPSS software, version 22 (IBM Corporation, Armonk, NY, USA).
From June 2005 to January 2018, we included 36 patients. Their baseline characteristics are summarized in
In a median follow up of 40.8 months, the median HPFS was 38.9 months, and the mean OS was 98 months (95% CI 73 - 123 months; median not reached). The disease control rate (complete response + partial response + stable disease) was 92.3% (12/13 patients) in the case of TACE and 91.3% (21/23 patients) in the group undergoing TAE. In patients with functioning tumors, clinically significant symptomatic control was seen in 62.5% (10/16 patients) in the TAE group and 50% (4/8 patients) in the case of TACE. There was no significant difference in the proportion of patients achieving reduction of at least 50% of 5HIAA in relation to type of embolization: TAE vs TACE (5/11 patients, 45.5% vs 3/6 patients, 50%; respectively). The median number of embolization procedures was 1 (range 1-5). Fifteen patients underwent more than one embolization procedures.
| Variable |
| No. Patients (%) |
| p value |
|---|---|---|---|---|
|
| Total | TAE | TACE |
|
| Gender Female | 18 (50) | 12 (52.2) | 6 (46.2) | 0.72 |
| Male | 18 (50) | 11 (47.8) | 7 (53.8) |
|
| Age, y Median (range) | 62 | 63 | 59 | 0.97 |
|
| (19-80) | (19-80) | (41-76) |
|
| Primary tumor Midgut | 20 (55.6) | 13 (56.5) | 7 (53.8) | 0.52 |
| Pancreas | 7 (19.4) | 3 (13) | 4 (30.8) |
|
| Lung | 3 (8.3) | 2 (8.7) | 1 (7.7) |
|
| Unknown | 6 (16.7) | 5 (21.7) | 1 (7.7) |
|
| Histological Grade 1 | 15 (50) | 11 (52.4) | 4 (44.4) |
|
| 2 | 13 (43.3) | 10 (47.6) | 3 (33.3) | 0.14 |
| 3 | 2 (6.7) | 0 | 2 (22.2) |
|
| Hepatic Tumor Burden < 50% | 18 (51.4) | 11 (47.8) | 7 (58.3) | 0.55 |
| = 50% | 17 (48.6) | 12 (52.2) | 5 (41.7) |
|
| Bone Metastases Yes | 10 (27.8) | 6 (26.1) | 4 (30.8) | 0.76 |
| No | 26 (72.2) | 17 (73.9) | 9 (69.2) |
|
Abbreviations: TAE, transarterial embolization; TACE, transarterial chemoembolization.
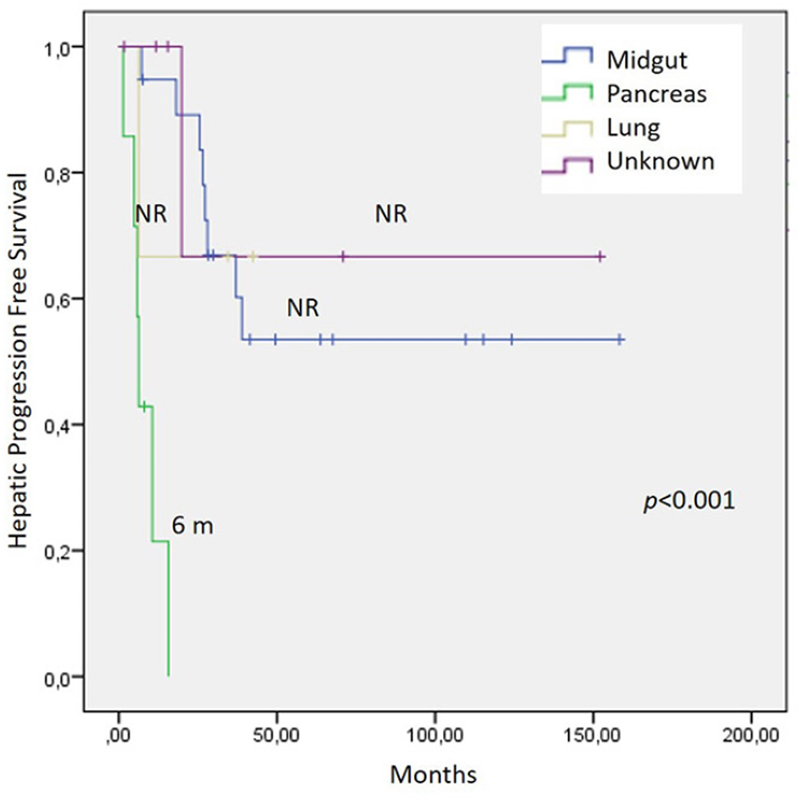
No significant differences were found in HPFS by type of embolization procedure: TAE vs TACE (nonreached vs. 37 months, p =0.34); or by number of embolizations: 1 vs more than one (37 vs 38 months, p =0.98); or by hepatic tumor burden ( p =0.93). Pancreatic primary was associated with significantly shorter HPFS ( p <0.001), as in showed in
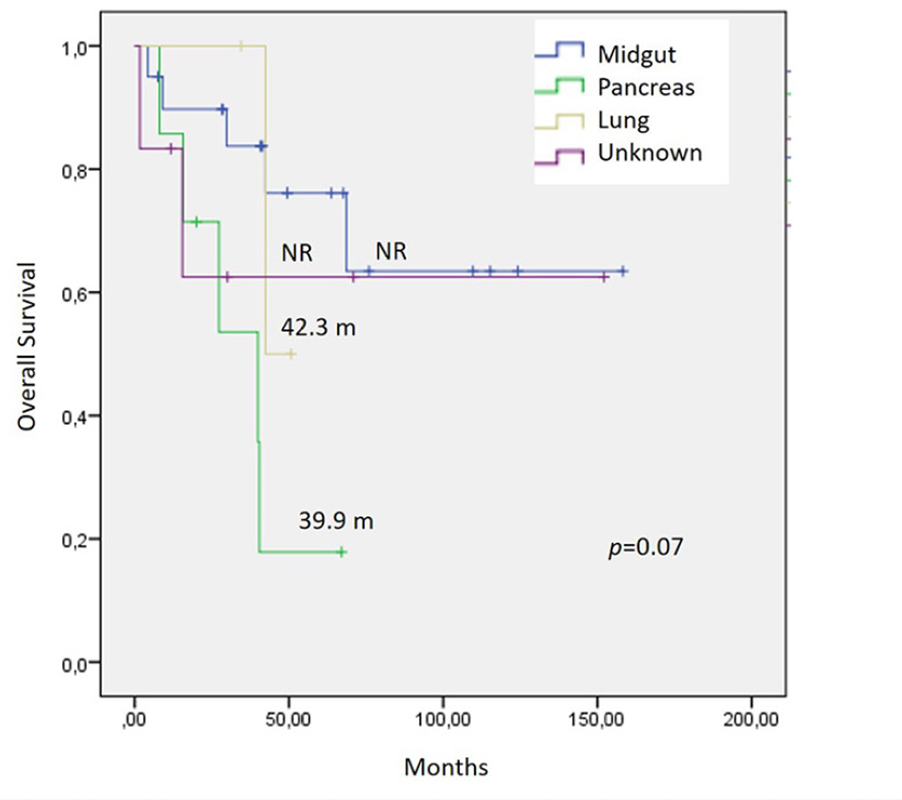
In terms of OS, no significant differences were found by type of embolization procedure: TAE vs TACE (42 months vs. not-reached, p =0.29), or by number of embolizations: 1 vs more than one (42 months vs not-reached, p =0.15); or by hepatic tumor burden ( p =0.19). Pancreatic primary showed a tendency of shorter OS ( p =0.07), as shown in
The most frequent adverse event of any grade was abdominal pain after the procedure in 13.8% (5/36) of patients. Fever was reported in 5.5% (2/36), and 2 patients developed biloma (one with TACE and one with TAE). There were no cases of procedure-related deaths.
This study shows improved clinical outcomes following TAE or TACE with significant symptomatic control and radiologic response. Our experience compares similarly with those of previously reported series from around the world. As we know, there have been no randomized controlled trials to confirm the survival benefit of TAE or TACE, and the positioning of these therapies in the treatment sequencing of NETs is not well defined in guidelines.
In numerous studies of embolization therapy, patients with functioning NETs presenting with liver metastases showed up to 75% of symptomatic improvement in flushing and diarrhea.
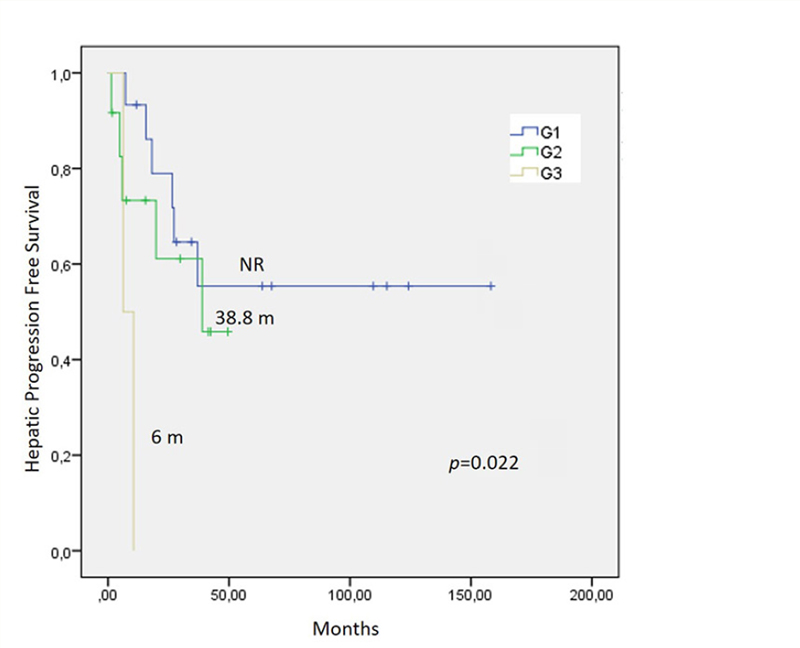
Figure 1 Hepatic Progression Free Survival after embolization procedure (TAE or TACE) in relation to tumor grade. Abbreviations: HPFS, Hepatic Progression Free Survival; TAE, transarterial embolization; TACE, transarterial chemoembolization; NR, not reached.
Figure 2 Hepatic Progression Free Survival after embolization procedure (TAE or TACE) in relation to primary site. Abbreviations: HPFS, Hepatic Progression Free Survival; TAE, transarterial embolization; TACE, transarterial chemoembolization; NR, not reached.
The reported median progression free survival and median overall survival from previous embolization studies ranged between 16 to 23 months and 18 to 80 months, respectively.
Figure 3 Overall Survival after embolization procedure (TAE or TACE) in relation to primary site.Abbreviations: OS, Overall Survival; TAE, transarterial embolization; TACE, transarterial chemoembolization; NR, not reached.
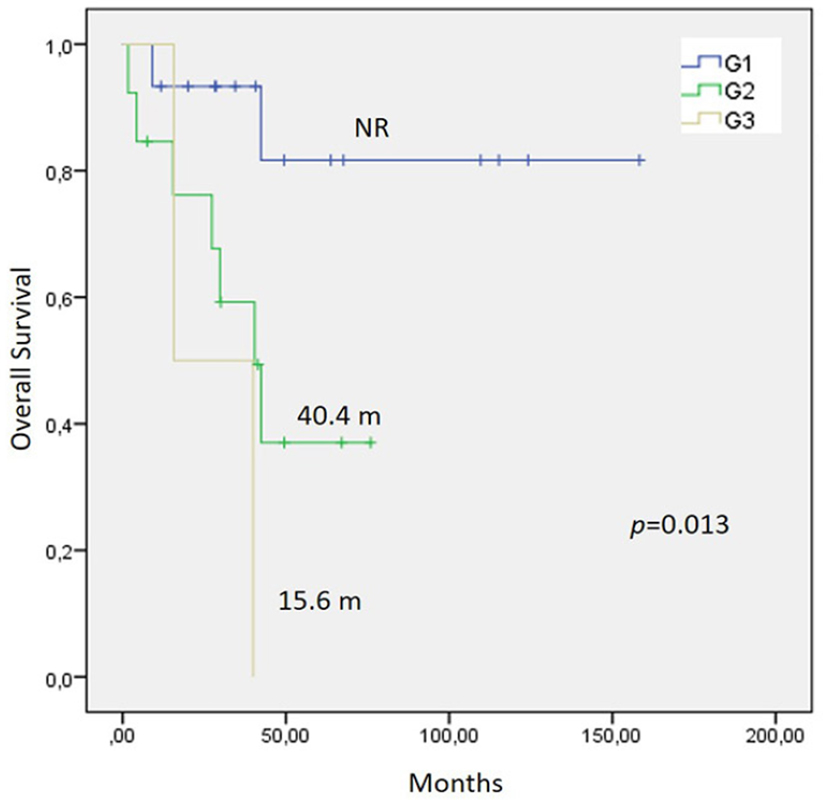
Figure 4 Overall Survival after embolization procedure (TAE or TACE) in relation to tumor grade. Abbreviations: OS, Overall Survival; TAE, transarterial embolization; TACE, transarterial chemoembolization; NR, not reached.
In our study, higher histological grade derived in shorter HPFS and OS, in concordance with other series.
Previous studies have reported conflicting survival outcomes for pancreatic NETs versus NETs from other origin.
Survival outcomes by type of embolization modality (TAE or TACE) in this study were within range of other series.
Adverse events were mild in our population, which is concordant with reported morbidity of TAE and TACE.
In the context of metastatic NETs, randomized phase 3 trials with systemic therapies showed improvement in PFS versus placebo, in the case of somatostatin analogues, PROMID (14.3 months) and CLARINET (median PFS not reached); and with everolimus, RADIANT 3 (11 months). Our study demonstrates that embolization therapy with a median PFS of 27.2 months is effective and safe, and is an excellent option for patients with functioning tumors particularly in the public system of developing countries like ours, where long-acting presentations of somatostatin analogues (SSA) are often not available. In these cases, a recommendation is to hospitalize the patient, initiate treatment with short-acting SSA, and control the symptoms with TAE or TACE, in order to avoid carcinoid crisis.
In terms of new loco-regional therapies, radioembolization with 90-Y in metastatic NETs is a new technique with limited but growing use. Similarly to other techniques, it has been reported to reduce symptoms in approximately 50% of patients with functioning tumors.
Our study has the inherent limitations of its retrospective design, as well as a small cohort size. Prospective studies are still awaited and should clarify the optimal indication of TAE or TACE. However, our study is the first in our region reporting results of these hepatic artery embolization techniques, showing that TAE and TACE are effective and feasible treatment options in NET patients with unresectable liver metastasis.
In conclusion, we believe that TAE and TACE are effective to treat liver metastases from well- differentiated NETs. Both techniques have apparently similar efficacy, and therefore we prefer to perform TAE35 because it is cheaper and less toxic. Embolization procedures can be repeated if good hepatic function is present. Importantly, our results reinforce the fact that these procedures are not good options for G3 tumors.
The authors have stated that they have no conflicts of interest.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.