The diagnosis and management of cervical masses are eventually a challenge for the oncologist and the head and neck surgeon. There are a variety of malignant and non-malignant entities that can present with a growing mass in the neck. When we look at malignant thyroid masses specifically, the carcinomas, including papillary, folicular, medular and anaplastic are the most frequent tumours. The extrapulmonary small cell neuroendocrine carcinoma (EPSCC) is a rare type of cancer that can virtually arise from any organ, being even more rare in the thyroid gland. Its postulated that just 2-5% of small cell neuroendocrine carcinomas arise at extrapulmonary sites, and being such a rare entity, data regarding its epidemiology is scarce. It is thought to arise from a multipotent stem cell with neuroendocrine features. The microscopic appearance resembles small cell carcinoma of the lung, so its important to differentiate a metastasis from a pulmonary tumor from an extrapulmonary primary. The clinical features also remember the small cell lung cancer behavior, with rapid growing tumours and frequent systemic dissemination, carrying a dismal prognosis. As well as others neuroendocrine carcinomas from other sites a multidisciplinary approach is essential, and efforts to better understand molecular mechanisms that trigger the disease are very important.
This case report is about a 40-years-old female patient admitted to the Hospital Felício Rocho, in Belo Horizonte, Minas Gerais, with airway compression caused by a rapid growing cervical mass that appeared few weeks before (
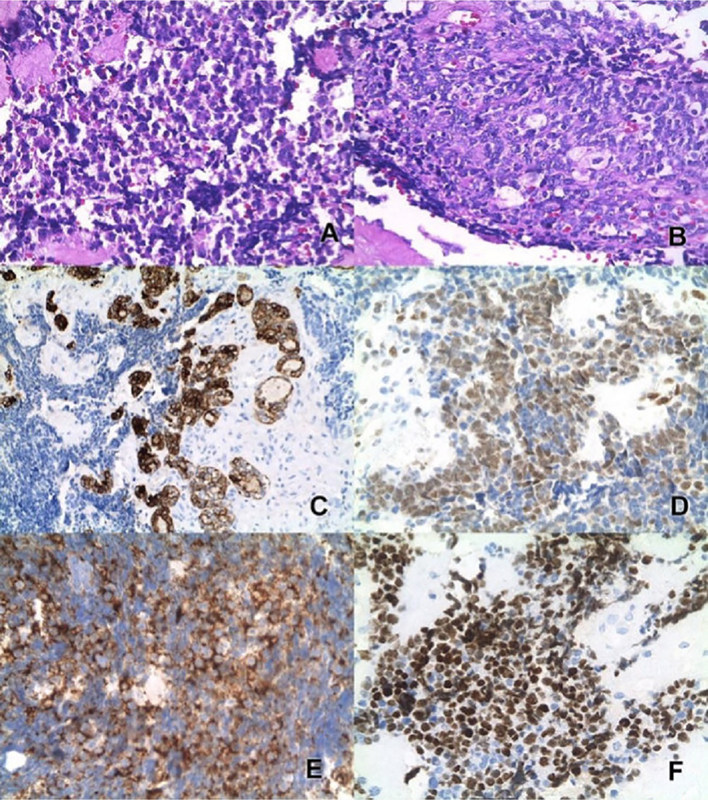
The initial immunohistochemical panel ruled out the possibility of lymphoma, as markers of epithelial differentiation (cytokeratins/EMA) were positive and lymphoid markers were negative.
The attending physicians debated the case and opted for thyroidectomy. During the procedure, the surgeon noted a thyroid gland with macroscopic alterations such as darkened color, friable tissue and periglandular fibrosis, which prevented its complete dissection and identification of the inferior laryngeal nerve. Therefore, a “near total” lobectomy was performed on the left side, due to the possibility of bilateral nerve injury if surgery continued under these circumstances. After surgery, rigid videolaryngoscopy showed preserved mobility of the vocal folds bilaterally, suggesting that there was no nerve damage.
Figure 1 Fast and progressive growth mass in the cervical region.
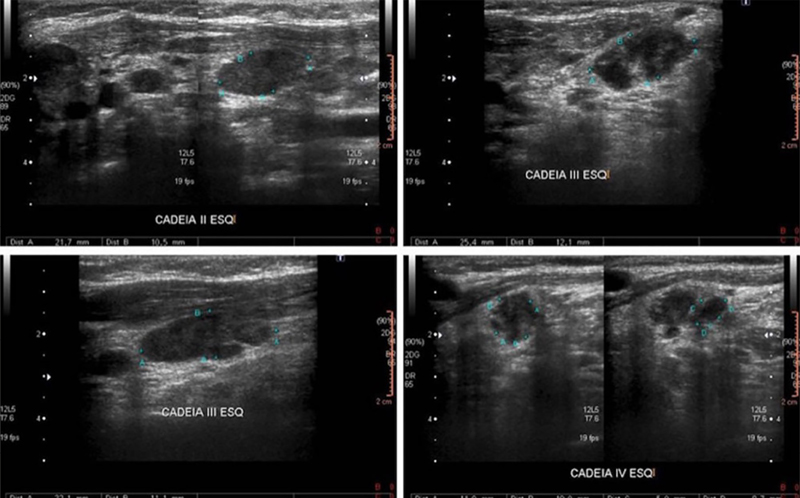
The histopathological report and immunohistochemistry of the postoperative specimen showed positivity of TTF-1, CD56 and synaptophysin, suggesting the diagnosis of small cell neuroendocrine carcinoma of the thyroid. TTF-1 is expressed in lung and thyroid carcinoma, and CD56 and synaptophysin positivity are suggestive of neuroendocrine differentiation. There were still palpable lymph nodes in the neck after surgery. “Ultrasonography evidenced numerical prominence of lymph nodes in bilateral cervical chains, some with increased dimensions, suspec ted for secondary neoplastic involvement (
Figure 2 Neoplastic tissue stained in H&E (A), areas of epithelial arrangement (B). In the reaction for cytokeratins, the small cells areas are negative, with expression in epithelial groups (C). Expression of FLI-1 (D), CD56 (E) and TTF-1 (F).
The patient underwent four cycles of chemotherapy with the EP protocol (Etoposide + Cisplatin), remaining with a small cervical lymph node clinically visible after the fourth cycle. She was then submitted to radiotherapy at this lymph node site (30 x 1.8 Gy) and lymphatic cervical drainage (25 x 1.8 Gy). After radiotherapy, the lymph nodes disappeared and were not visible or palpable. She was referred again to the head and neck surgeon to evaluate the possibility of resection of the remanescent thyroid. However, before the surgery was done, about one month later after finishing the neck radiotherapy, a strong lumbar back pain started. A nuclear magnetic resonance of the spine showed metastasis in lumbar vertebra with radicular compression in L5/S1. A surgical decompression was done, with rapid pain improvement. The pathological report was compatible with metastatic small cell neuroendocrine carcinoma. Restaging tomography of thorax and abdomen showed metastasis in many posterior lumbar vertebras and left external iliac lymphadenomegaly. The patient started with VCA chemotherapy (vincristine, cyclophosphamide, doxorubicin) every three weeks. About three weeks after the second cycle (before receiving the third), there was again worsening of the lumbar pain (L2) and a new magnetic resonance showed radicular compression in the second lumbar vertebra. The third cycle was postponed and the patient is on local palliative radiotherapy, which is still ongoing.
Figure 3 Bilaterally prominent cervical lymph nodes, more on the left. Some of them have globules, heterogeneous and/or irregular contours, with no obvious greasy threads, suspected for secondary neoplastic involvement
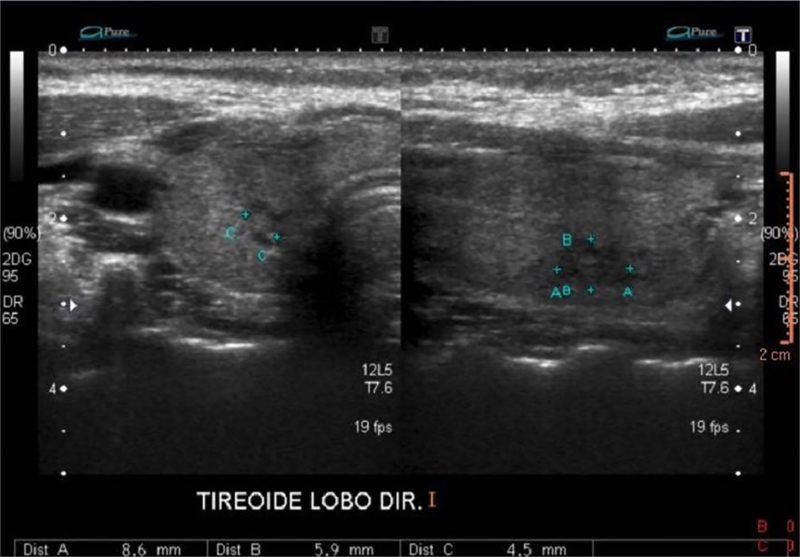
Figure 4 A predominantly isoechoic heterogeneous solid nodule with hypoechoic areas of permeation, imprecise limits and no apparent calcification in the lower third of the right lobe, measuring about 0.9 x 0.6 x 0.5 cm.
Small cell neuroendocrine carcinomas are a group of malignant tumours that can virtually arise from any organ, but lung primaries are the most frequent ones and primary lesions in the head and neck are very rare. Extrapulmonary small cell carcinoma (EPSCC) compromises only 2.5-4% of all small cell carcinomas, with an overall incidence of approximately 0.1 to 0.4% of all cancers.
Primary small cell neuroendocrine carcinoma of the thyroid are extremely rare, and just a few cases have been described in literature.
In the same way as small cell lung carcinomas (SCLC) and extrapulmonary primaries share similar morphology, some molecular alterations appear to be also common in both entities. Overexpression of p53, Rb inativation increased bcl-2 expression, telomerase activation, k-ras mutation and c-myc amplification were described,
EPSCC is characterised by aggressive clinical behaviour and dismal outcome with currently available treatment strategies.
There is not a consensus about the best treatment approach in EPSCC, including the thyroid primaries, since these tumours are rare and there isn't specific data about it. As the clinical course of these tumours resemble lung small cell neuroendocrine primaries, the treatment often used is similar.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.

Dados de acesso insuficientes para visualização no mapa.