Primary mediastinal large B-cell lymphoma (PMBL) is an aggressive B-cell lymphoma that has a low prevalence in the population, occurring in 2.4% of non-Hodgkin lymphoma cases, accounting for approximately 3,000 cases in Brazil per year.
Due to its distinct clinicopathological characteristics, PMBL has been identified as a specific entity recognized by the World Health Organization (WHO) classification of lymphoid neoplasms,
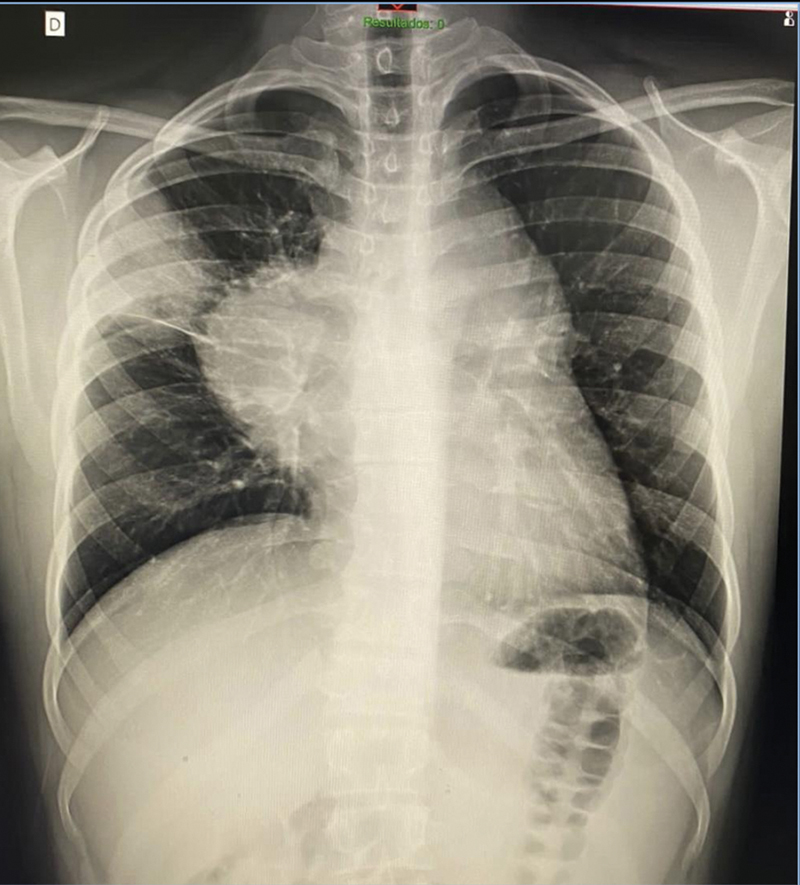
A 24-year-old white male patient came to the emergency room with symptoms of dyspnea. A chest X-ray was requested, and two masses were seen in the mediastinum region (
Fig. 1 Chest X-ray with evidence of mediastinal tumor masses.
Fig. 2 Patient with edema of limbs, chest, and cervical region due to thrombosis secondary to superior vena cava syndrome.
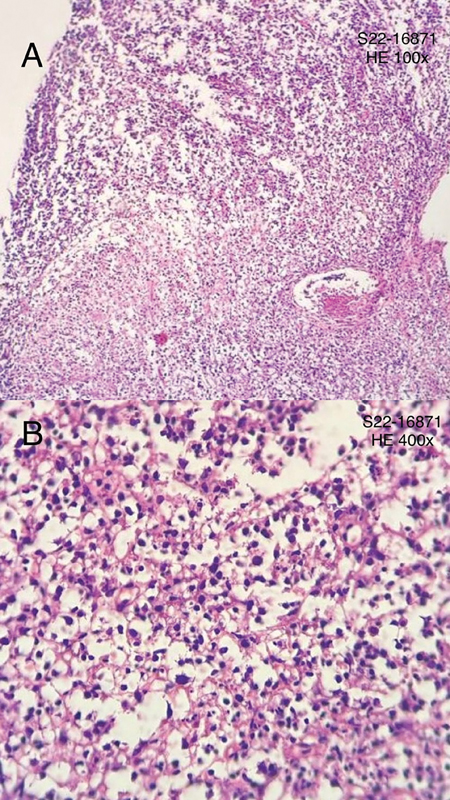
The biopsy of the mediastinal mass showed an anatomopathological diagnosis of small cell proliferation with extensive necrotic areas (
Fig. 3 (A) Proliferation of small lymphocytic cells and necrosis area (hematoxylin-eosin [HE]: 100x). (B) Proliferation of small lymphocytic cells (HE: 400x).
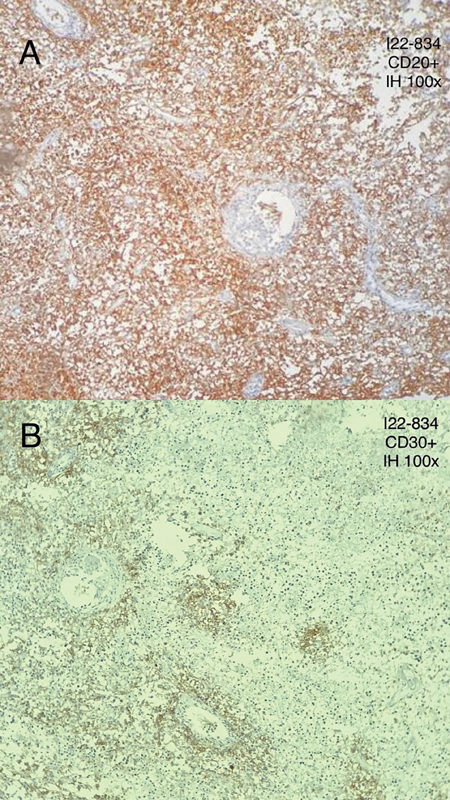
Fig. 4 (A) Positive diffuse immunolabeling of CD20 in atypical cells (100x). (B) Positive focal immunolabeling of CD30 in atypical cells (100x).
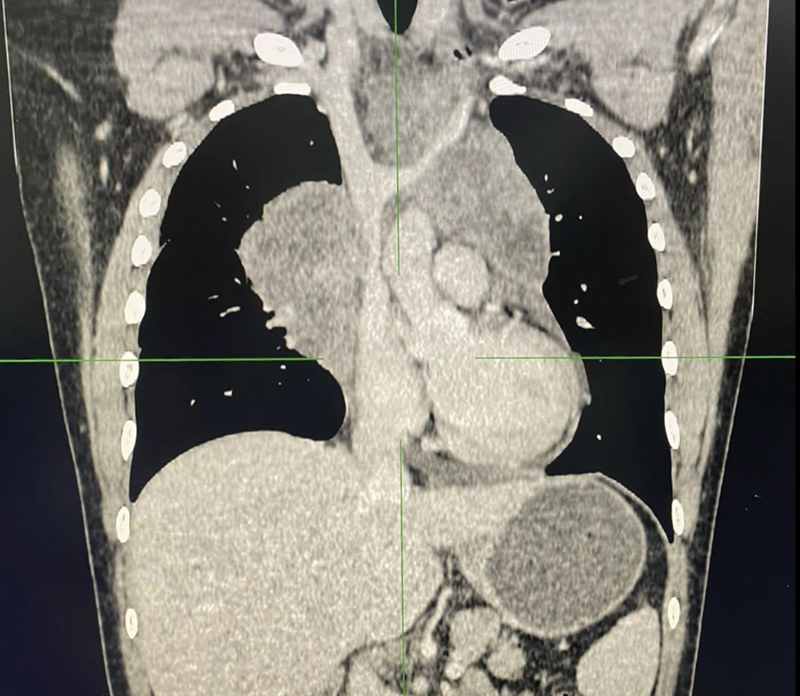
The positron emission tomography (PET) CT scan showed a lymph node cluster in the anterosuperior mediastinum (mediastinal bulky) measuring 17.2 × 9.9 × 15.4 cm, in close contact with the ascending thoracic aorta and SVC, suggesting supra-diaphragmatic nodal lesions in the thoracic region with glycolytic hypermetabolism, compatible with an active lymphoproliferative neoplasm and slight anterior and posterior pericardial effusion, with no signs of tamponade. Computed tomography angiography of the chest showed evidence of opacity and consolidation in the middle lobe of the right lung, as well as a heterogeneous mass in the anterosuperior mediastinum measuring 14.9 × 9.3 cm, involving the thoracic aorta in the region of the aortic arch, compressing the SVC (
Fig. 5 Chest angiotomography showing mediastinal masses involving the thoracic aorta and compressing the superior vena cava.
The treatment instituted was dose-adjusted etoposide, doxorubicin, and cyclophosphamide with vincristine and prednisone plus rituximab (DA-EPOCH-R), a combination of drugs indicated for the treatment of this disease: 6 cycles with an interval of 21 days each cycle.
Symptoms related to compression or invasion of local structures are common, such as dyspnea and cough.
The differential diagnosis of PMBL includes benign and malignant mediastinal tumors (which can cause external compression or direct invasion of the central venous system) and, less commonly, infectious and inflammatory entities that can present mediastinal involvement. Mediastinal tumors include DLBCL, with secondary mediastinal involvement, and the nodular sclerosis Hodgkin lymphoma.
Corroborating the frequently reported origin in the thymus, the positive immunohistochemical expression of AE1/AE3 in the mediastinal mass establishes its thymic origin. Its locally invasive presentation in the anterior mediastinum was also observed on complementary imaging tests. A retrospective analysis of cases of PMBL showed that 93% of patients had an invasion of adjacent mediastinal structures. In approximately half of the patients, the primary tumor measures > 10 cm in its largest dimension and, therefore, constitutes a bulky disease.
The DA-EPOCH-R therapy used is corroborated by the guidelines of the European Society for Medical Oncology and other medical organizations as first-line therapy.
The importance of early diagnosis of primary mediastinal large B-cell lymphoma, a neoplasm with a low prevalence, should be considered in the differential diagnosis in young patients with mediastinal manifestations, with a view to a precise therapeutic approach. The emphasis on clinical presentation, including compressive symptoms and SVCS, highlights the importance of early identification of these signs for effective management. In addition, the discussion on the specific immunophenotyping of PMBL and its WHO classification emphasizes its uniqueness among B-cell lymphomas.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Savage, K J. Primary mediastinal large B-cell lymphoma. Blood [online]. 2022, vol. 140, p. 955-970. https://doi.org/10.1182/blood.2020008376 Ver referência
2. British Society for Haematology Guidelines. The management of primary mediastinal B-cell lymphoma: a British Society for Haematology Good Practice Paper. Br J Haematol [online]. 2019, vol. 185, p. 402-409. https://doi.org/10.1111/bjh.15731 Ver referência
3. Alaggio, R and Amador, C and Anagnostopoulos, I. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia [online]. 2022, vol. 36, p. 1720-1748. https://doi.org/10.1038/s41375-023-01962-5 Ver referência
4. Lees, C and Keane, C and Gandhi, M K and Gunawardana, J. Biology and therapy of primary mediastinal B-cell lymphoma: current status and future directions. Br J Haematol [online]. 2019, vol. 185, p. 25-41. https://doi.org/10.1111/bjh.15778 Ver referência
5. Oliveira, F AM and Santos, A BVD and Brasil, S AB. Linfoma Primário De Mediastino: Análise Retrospectiva Dos Fatores Prognósticos E Resposta À Terapia De Primeira Linha Nos Pacientes Da Santa Casa De São Paulo De 2008-2018. Hematol Transfus Cell Ther [online]. 2022, vol. 44, p. S123. https://doi.org/10.1016/j.htct.2022.09.207 Ver referência
6. Besteiro, B and Teixeira, C and Gullo, I and Pereira, S and Almeida, M and Almeida, J. Superior vena cava syndrome caused by mediastinal lymphoma: A rare clinical case. Radiol Case Rep [online]. 2021, vol. 16, p. 929-933. https://doi.org/10.1016/j.radcr.2021.01.063 Ver referência
7. Seligson, M T and Surowiec, S M. Superior Vena Cava Syndrome. [Updated 2022 Sep 26]. StatPearls Publishing, 2024.
8. Zhou, H and Xu-Monette, Z Y and Xiao, L. Prognostic factors, therapeutic approaches, and distinct immunobiologic features in patients with primary mediastinal large B-cell lymphoma on long-term follow-up. Blood Cancer J [online]. 2020, vol. 10, p. 49. https://doi.org/10.1038/s41408-020-0312-7 Ver referência

Dados de acesso insuficientes para visualização no mapa.