Prostate cancer is the second most common cancer in men worldwide. It is estimated that by 2030, 1.9 million men will be diagnosed with prostate cancer globally, with around 50.000 deaths. In Brazil, 97,000 new cases were diagnosed in 2020, with approximately 18,000 deaths.
Since the 1950s, androgen deprivation therapy (ADT) is the backbone of treatment for metastatic disease.
Abiraterone acetate (AA) was developed in the 1990s and it is a potent selective inhibitor of CYP17A1, member of p450 cytochrome family and involved in androgen production. AA mechanism of action is based on reducing androgen synthesis, including at the tumor and microenvironment level, and at the adrenal gland.
Since the initial AA approval, several indications emerged, including mCRPC pre-docetaxel,
Despite the dose of 1,000mg fasting has been chosen as recommended phase 2 dose (RP2D), the safety and pharmacokinetics of AA when coadministrated with food was also tested.
In 2018, Szmulewitz et al.
In Brazil, AA at the label dose is not affordable to over 75% of patients treated under the public national health plan (Sistema Único de Saúde – SUS). However, a lower dose of 250mg with food may fit into the budget and has already been prescribed at some Brazilian centers.
After ethical approval (CAAE 59172022.1.0000.5415), a survey was created utilizing the questionnaire tool of the Research Electronic Data Capture (REDCap) of Hospital de Base.
The primary objective was to evaluate and describe the AA prescription pattern among medical oncologists in Brazil and which percentage of prescribers are knowledgeable of the literature supporting the prescription of AA low-dose. The secondary objectives included describing demographics of respondents and better understand the pattern of prescription of AA in Brazil.
Demographic characteristics were summarized in means, medians, and proportions. Logistic regression was employed to identify factors associated with the prescription of AA low-dose. We used the Peto odds methods for associations with 0-counts. Multivariable analyses were not performed. Data analysis was performed using the IBM SPSS statistical software version v. 28.0.10.
In total, 48 prescribers responded the survey - 45 medical oncologists and 3 urologists. Because of the small sample size, we decided to exclude urologists’ response from the statistical analysis. The median age of respondents is 35.5 years old and 55.6% are female '
| Medical oncologists N=45 | |
|---|---|
| Age - yr | |
| Median | 35.5 |
| Range | 28-70 |
| Gender – no. (%) | |
| Female | 25 (55.6) |
| Male | 20 (44.4) |
| Time since the complete of medical specialty – no. (%) | |
| <5 years | 23 (51.1) |
| 5-10 years | 7 (15.6) |
| >10 years | 15 (33.3) |
| Practice characteristic – no. (%) | |
| Public healthcare system | 4 (8.9) |
| Private healthcare system | 8 (17.8) |
| Public and private healthcare system | 33 (73.3) |
| Work at an academic institution – no. (%) | |
| Yes | 39 (86.7) |
| No | 6 (13.3) |
| Average proportion of patients with prostate cancer in their practice – % (SD) | 25% (16) |
| Had read the Szmulewitz et al. | N=44 |
| Yes | 38 (86.4) |
| No | 6 (13.6) |
| Awareness of the NCCN guidelines acknowledging the use of AA low-dose – no. (%) | N=44 |
| Yes | 36 (81.8) |
| No | 8 (18.2) |
When asked if they had read the phase II study by Szmulewitz et al. (2018),
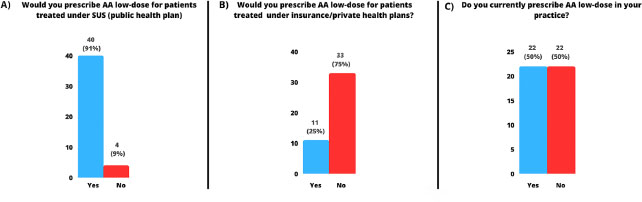
Figure 1 A) Percentage of medical oncologists who would prescribe and would not prescribe AA low-dose in the public health plan (SUS); B) Percentage of medical oncologists who would prescribe and would not prescribe AA low-dose in the private healthcare system; C) Percentage of medical oncologists who already prescribe AA low-dose in their clinical practices.
We investigated factors associated with the prescription of AA low-dose (
| OR (95% CI) | p-value | |
|---|---|---|
| Age | 1.02 (0.94-1.10) | 0.59 |
| Gender | ||
| Time since the end of medical specialty | 1.44 (0.44-4.75) | 0.54 |
| <5 years | Ref | 0.33 0.07 |
| 5-10 years | 2.33 (0.41-12.17) | |
| >10 years | 3.50 (0.88-13.92) | |
| Work at an academic institution Yes | Ref | 0.39 |
| No | 2.22 (0.36-13.61) | |
| Had read the Szmulewitz et al. | Ref | |
| No | 9.61 (1.75-52.74) | 0.02 |
| Awareness of the NCCN guidelines acknowledging the use of AA low-dose | Ref | 0.04 |
| Yes | 9.8 (1.09-88.2) | |
| No |
Concerning the corticosteroid prescription associated with AA, 41.9% of respondents use prednisone 5mg twice daily for all patients and 23.3% use 5mg twice daily to patients with mCRPC, and 5mg daily to CSPC. When inquired about corticosteroid switch upon PSA progression, 34.9% reported being adept to this practice. The most cited reason not to perform the steroid switch was not being familiar with the literature supporting this practice (75%).
We had 3 responses among urologists. All of them were male, aged 49, 29 and 34 years old, and worked at an academic institution. Two of them had completed their final specialties within 5 years, and the other over 10 years after the survey date. Prostate cancer patients represent between 5-20% of their clinical practice. All urologists’ respondents never had read the Szmulewitz et al.
In our surveyed population, most prescribers were knowledgeable about data supporting the use of AA low-dose. Moreover, over 90% of medical oncologists were willing to prescribe AA low-dose for patients treated under the Brazilian national health plan (SUS) — where resources are scarcer and treatment options are limited — and half were already using AA low-dose as part of their arsenal for prostate cancer treatment. As expected, physicians who had read the article by Szmulewitz et al.
Our survey share similarities with the work conducted by Patel et al. (2020)
While most of our surveyed oncologists would prescribe AA low-dose in the public health system (SUS), only 50% had already adopted AA low-dose in their practices. The reasons for that are likely multifactorial and are beyond the scope of this project. In a recent literature review, concerns about erratic exposure of AA under diverse dietary patterns are amongst potential reasons.
Lower doses of AA can result in up to 75% cost savings which is highly relevant to LMICs such as Brazil. Several data support the use of AA at a lower dose with food.
The dosing conundrum of oncology agents has been the subject of recent scrutiny by several groups including the Optimal Cancer Care Alliance (OCCA —
In reference to corticosteroid therapy, our study showed AA is most frequently prescribed (41.9%) in association with prednisone 5mg twice daily regardless of the treatment scenario, in line with the prescription patterns of to the pivotal trials COU-AA-301 and COU-AA-302(5,6) and in opposition to the LATITUDE trial that used 5mg/daily to CSPC.
We acknowledge several limitations of this study. First, the response rate of our survey was low, with only 48 respondents. Furthermore, only 3 urologists responded to the survey making our findings most applicable to medical oncologists. Secondly, our sample was acquired by convenience which by default induces biases in interpretation of results. For instance, our population was mostly constituted of physicians working at academic centers, who are more likely to be updated with medical literature. We hypothesize that awareness of AA low-dose is lower than what we found in this survey. Finally, our limited sample size prevented performing multivariable analyses.
It is important to discuss AA low-dose in Brazil and other LMICs, particularly in settings where the standard treatment is unavailable due to cost constraints. Larger studies (e.g., phase 3 trials) investigating AA low-dose are unlikely to occur as these are off the agenda of pharmaceutical industries.
This survey study showed a trend towards Brazilian medical oncologists prescribing AA lowdose. However, only half of the respondents already use AA-low in their practices. We advocate for broader use of AA low-dose, increasing accessibility.
No funding was used for this work.
| JPHN | Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing. |
| LAF | Final approval of manuscript, Provision of study materials or patient |
| JAS | Final approval of manuscript, Provision of study materials or patient |
| FLCF | Final approval of manuscript, Provision of study materials or patient |
| DVA | Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient |
The questions and possible answers (when multiple-choice) of the survey applied to physicians:
1 - Demographics data:
a) How old are you?
b) Gender;
c) What is your medical specialty? Possible answers: urologist or medical oncologist;
d) Where do you work? Possible answers: public healthcare system, private healthcare system or both.
e) How long has it been since the end of your medical specialization? Possible answers: < 5 years or >= 5 years;
f) Do your work at an academic institution? Possible answers: Yes or No;
g) What percentage of patients with prostate cancer do you treat in your clinical practice?
2 - AA prescription data:
a) Have you ever read “Prospective International Randomized Phase II Study of Low Dose Abiraterone With Food Versus Standard Dose Abiraterone In Castration-Resistant Prostate Cancer” by Szmulewitz RZ et al? Possible answers: Yes or No;
b) Do you know that AA low-dose (250 mg/day) with low-fat meal was incorporated by NCCN like an alternative option to the standard dose (1000 mg/day)?
c) Possible answers: Yes or No;
d) Would you prescribe AA 250 mg/day with low-fat meal in the public healthcare? Possible answers: Yes or No. If the answer was No:
d.1: Because I do not trust the data;
d.2: Because it is not the standard of care;
d.3: I would not because I do not know the literature basis;
Would you prescribe AA 250 mg/day with low-fat meal in private healthcare? Possible answers: Yes or No;
e) Do you already prescribe AA 250 mg/day with low-fat meal in your clinical practice? Possible answers: Yes or No;
3 - Novel antiandrogens prescription data
f) In which situations do you prescribe the novel antiandrogen therapies?
Possible answers: just to metastatic castration-resistant, to metastatic castration-sensitive AND castration-resistant, to metastatic and non-metastatic high and very high risk.
4 - Corticosteroid therapy data
g) Do you switch the corticosteroid therapy when PSA progressing? Possible answers: Yes or No. If the answer was No:
g.1: Because I do not know the literature embasament;
g.2: Because I do not trust the data;
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. GLOBOCAN 2020: estimated cancer incidence, mortality and prevalence worldwide in 2020. [Internet]. WHO, 2020.
2. Hellerstedt, BA and Pienta, KJ. The current state of hormonal therapy for prostate cancer. Cancer J Clin [online]. 2002, vol. 52, p. 154-79.
3. Scher, HI and Sawyers, CL. Biology of progressive, castration-resistant prostate cancer: directed therapies targeting the androgen-receptor signaling axis. JCO [online]. 2005, vol. 23, p. 8253-61.
4. Patel, A and Tannock, IF and Srivastava, P and Biswas, B and Gupta, VG and Batra, A. Low-dose abiraterone in metastatic prostate cancer: is it practice changing? Facts and facets. JCO Glob Oncol [online]. 2020, vol. 6, p. 382-6.
5. Bono, JS and Logothetis, CJ and Molina, A and Fizazi, K and North, S and Chu, L. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med [online]. 2011, vol. 364, p. 1995-2005.
6. Ryan, CJ and Smith, MR and Bono, JS and Molina, A and Logothetis, CJ and Souza, P. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med [online]. 2013, vol. 368, p. 138-48.
7. Fizazi, K and Tran, N and Fein, L and Matsubara, N and Rodriguez-Antolin, A and Alekseev, BY. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol [online]. 2019, vol. 20, p. 686-700.
8. Fizazi, K and Foulon, S and Carles, J and Roubaud, G and McDermott, R and Fléchon, A. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet [online]. 2022, vol. 399, p. 1695-707.
9. Attard, G and Murphy, L and Clarke, NW and Cross, W and Jones, RJ and Parker, CC. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet [online]. 2022, vol. 399, p. 447-60.
10. Sternberg, CN and Fizazi, K and Saad, F and Shore, ND and De Giorgi, U and Penson, DF. Enzalutamide and survival in nonmetastatic, castration-resistant prostate cancer. N Engl J Med [online]. 2020, vol. 382, p. 2197-206.
11. Fizazi, K and Shore, N and Tammela, TL and Ulys, A and Vjaters, E and Polyakov, S. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N Engl J Med [online]. 2019, vol. 380, p. 1235-46.
12. Smith, MR and Saad, F and Chowdhury, S and Oudard, S and Hadaschik, BA and Graff, JN. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med [online]. 2018, vol. 378, p. 1408-18.
13. Chi, KN and Spratlin, J and Kollmannsberger, C and North, S and Pankras, C and Gonzalez, M. Food effects on abiraterone pharmacokinetics in healthy subjects and patients with metastatic castration-resistant prostate cancer. J Clin Pharmacol [online]. 2015, vol. 55, p. 1406-14.
14. Abiraterone acetate [label]. Product monograph. Janssen, 2011.
15. Szmulewitz, RZ and Peer, CJ and Ibraheem, A and Martinez, E and Kozloff, MF and Carthon, B. Prospective international randomized phase ii study of low-dose abiraterone with food versus standard dose abiraterone in castration-resistant prostate cancer. JCO [online]. 2018, vol. 36, p. 1389-95.
16. National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. NCCN, 2022.
17. Zucca, LER and Neif, JAJ and Preto, DDA and Cordeiro Dias, IC and Araujo, HS and Carcano, FM. Real-world outcome with abiraterone low-dose plus prednisone in patients with mCRPC in a Brazilian Public Cancer Center. JCO [online]. 2020, vol. 38, p. e17563.
18. Harris, PA and Taylor, R and Thielke, R and Payne, J and Gonzalez, N and Conde, JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform [online]. 2009, vol. 42, p. 377-81.
19. Harris, PA and Taylor, R and Minor, BL and Elliott, V and Fernandez, M and O’Neal, L. The REDCap consortium: building an international community of software platform partners. J Biomed Inform [online]. 2019, vol. 95, p. 103208.
20. Scheffer, M. Demografia médica no Brasil 2023. FMUSP/AMB, 2023.
21. Dey, T and Goyal, S and Periasamy, K and Madan, R. Is lowdose abiraterone for prostate cancer an attractive strategy for limited resource settings?. Indian J Med Paediatr Oncol [online]. 2022, vol. 43, p. 40-6.
22. Leibowitz-Amit, R and Seah, J-A and Atenafu, EG and Templeton, AJ and Vera-Badillo, FE and Alimohamed, N. Abiraterone acetate in metastatic castration-resistant prostate cancer: a retrospective review of the Princess Margaret experience of (I) low dose abiraterone and (II) prior ketoconazole. Eur J Cancer [online]. 2014, vol. 50, p. 2399-407.
23. Shah, M and Rahman, A and Theoret, MR and Pazdur, R. The drugdosing conundrum in oncology — when less is more. N Engl J Med [online]. 2021, vol. 385, p. 1445-7.
24. Optimal Cancer Care Alliance. Homepage [Internet]. Optimal Cancer Care Alliance, 2022.
25. Araujo, D and Greystoke, A and Bates, S and Bayle, A and Calvo, E and Castelo-Branco, L. Oncology phase I trial design and conduct: time for a change - MDICT Guidelines 2022. Ann Oncol [online]. 2023, vol. 34, p. 48-60.
26. Fizazi, K and Tran, N and Fein, L and Matsubara, N and Rodriguez-Antolin, A and Alekseev, BY. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. [online]. 2017, vol. 377, p. 352-60.
27. Attard, G and Merseburger, AS and Arlt, W and Sternberg, CN and Feyerabend, S and Berruti, A. Assessment of the safety of glucocorticoid regimens in combination with abiraterone acetate for metastatic castration-resistant prostate cancer: a randomized, open-label phase 2 study. JAMA Oncol [online]. 2019, vol. 5, p. 1159-67.
28. Lorente, D and Omlin, A and Ferraldeschi, R and Pezaro, C and Perez, R and Mateo, J. Tumour responses following a steroid switch from prednisone to dexamethasone in castration-resistant prostate cancer patients progressing on abiraterone. Br J Cancer [online]. 2014, vol. 111, p. 2248-53.
29. Tannock, IF and Ratain, MJ and Goldstein, DA and Lichter, AS and Rosner, GL and Saltz, LB. Near-equivalence: generating evidence to support alternative cost-effective treatments. J Clin Oncol [online]. 2021, vol. 39, p. 950-5.
Dados de acesso insuficientes para visualização no mapa.