Virtual reality (VR) may be used as a non-pharmacological intervention which is capable of managing psychological and physical symptoms in childhood cancer treatment.
Cancer pain can be caused by various processes, such as the course of the disease, nerve compression, the therapies administered, and, especially, the various procedures to which the patients are submitted.
In a study with children diagnosed with aggressive tumors of the central nervous system,
In recent literature reviews,
Therefore, distraction plays a role in the theory of attention to pain,
Much of the literature on anxiety addresses dental visits and surgical procedures, but premedical consultation anxiety—especially at a child's first appointment for a major diagnosis such as cancer—remains less explored. The current study evaluated the effect of virtual-reality glasses on children's perceptions of pain and anxiety before medical consultation during their initial blood collection in a pediatric cancer hospital.
The present is a randomized clinical trial with two arms and no blinding performed in a pediatric oncology hospital located in the state of São Paulo, Brazil, with children and adolescents in their first collection and medical consultation at our institution. Data collection took place from January to June 2023.
We included patients aged between 7 and 16 years with their first scheduled outpatient appointment. Patients with visual/auditory deficits, sensitivity to light, nausea or vomiting induced by visual stimuli, with tumors that prevent the use of the glasses, epilepsy, impeditive cognitive deficit, untreated anxiety or mental disorders, and organic cerebral syndrome with impeditive deficits were excluded according to the recommendations of the manufacturer and validation of the team.
The researchers evaluated pain in two moments to identify the need for intervention: during the invitation and in the precolection questionnaire. Patients with pain that required intervention were referred to the Center of Outpatient Complications for appropriate treatment.
Participants were recruited through convenience, non-probability sampling, as only patients attending their first consultation were eligible and recruitment depended on the hospital's flow. To estimate feasibility, we calculated the average number of first consultations within the age range of our inclusion criteria. The sample size was based on previous VR studies, considering 80% power, a 5% significance level, and effect sizes reported in the literature, resulting in an estimated requirement of approximately 80 participants.
The characterization questionnaire was created by the authors. To evaluate pain and anxiety before and after the collection, semi-structured questionnaires were also developed, based on Manzini's interview in social research theory,
The development of the semi-structured interview questionnaires was evaluated by a panel of health professionals composed of 4 nurses and 1 physician; the instruments were pilot-tested for clarity and feasibility. For the measurement of puncture pain, the numerical verbal scale was selected, because its use is a standard at our institution.
In the present study, we analyzed quantitative variables—age of the child and pain scores (0–10) before and during venipuncture—and qualitative variables, classified as nominal or ordinal.
Nominal variables: sex, family history of cancer, previous diagnosis, prior blood collection and related pain, pain before and during the procedure, anxiety regarding the medical consultation, and perception after the procedure. In the intervention group, additional items assessed prior knowledge of VR, participants' opinions about the headset, and their sensations and perceived performance during the VR game. and a comparison between collection with and without the glasses. The companions reported perceived pain in the child, usual reactions during blood draws, and evaluated the care provided; in the intervention group, they also commented on the headset's usefulness and benefits.
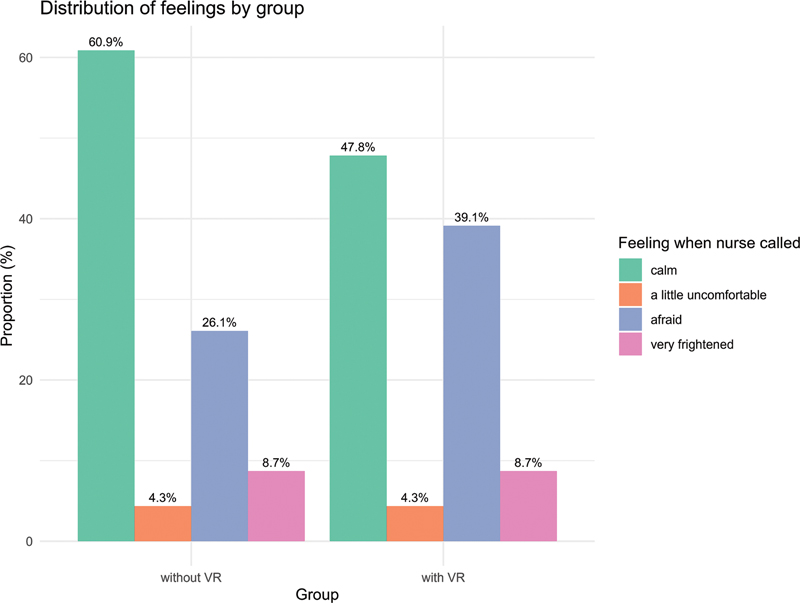
Ordinal variables: companion's level of schooling and kinship to the child, and the child's emotional state while waiting and when called for the procedure (calm, anxious, a little scared/uncomfortable, afraid, or very frightened).
The questionnaires followed the sequence of the encounter:
Participant and companion characterization – demographic data of the child and companion, family cancer history, and existing diagnoses.
Preprocedure (with/without) – current pain and intensity, previous blood collection experience, anxiety about the medical visit, and feelings while waiting and when called.
Postprocedure (with/without) – pain during venipuncture and intensity, anxiety regarding the medical visit, and immediate feelings after the procedure.
Additional items in the intervention group – before the procedure: knowledge of VR and interest in games; after the procedure: enjoyment and difficulty of the game, sensations while playing, perceived performance, and comparison between collection with and without the headset.
Companion interview – perception of the child's pain, typical pain behaviors, and evaluation of the care provided; in the intervention group, opinion regarding the headset and perceived benefits with two open questions: they were asked if they thought that the use of glasses brought benefits to the child/adolescent, and, if so, what benefits; moreover, both the companions in both groups were questioned about the quality of the care provided so far (if it was different from the other places where the child had already been treated).
At the first appointment, the pediatric patients followed the hospital's standard flow: medical record opening, laboratory tests, and nursing screening. During screening, the researcher invited eligible patients, obtained consent, and performed randomization through REDCap (Vanderbilt University). Blood collection was performed in an equipped office. The intervention group used VR glasses before the procedure, while the control group followed the conventional protocol. Patients and companions filled out the pre- and postprocedure questionnaires, and a nurse trained in blood collection and VR assisted the process.
The analysis of the sample involved frequency tables for qualitative variables and measures of central tendency and dispersion for quantitative variables. To compare the pain between groups, the Student's t-test or the Mann-Whitney test was used, according to the normality of the data evaluated by the Shapiro-Wilk test. The associations among categorical variables were analyzed through the Fisher's exact test or the Chi-squared test. The data were recorded in REDCap, version 11.1.18, and analyzed in the R (R Foundation for Statistical Computing) software, version 4.5.0, with a significance level of 5%. The answers to the open question were independently examined by two researchers, who grouped similar passages into descriptive thematic categories.
For the intervention, Mirage Solo VR glasses (Lenovo Group Limited) were used. The Peruvian company FeelsGood adapted the device by creating a hospital-specific game and blocking access to websites and other tools, allowing only this customized game to be used. When adjusted to the child's face, the game starts: the child uses eye movements to hit objects, with no sudden movements, scary scenarios, or penalties for missed objects. The game includes multiple immersive scenarios (sea, forest, sky, beach, camping), which change automatically.
During blood collection, the professional places the glasses 2 to 5 minutes before the puncture while preparing materials and performing antisepsis. At puncture time, a button intensifies visual and auditory stimuli, such as animated animals or characters, to distract the child. The procedure can be repeated, if necessary, as the game only ends when the glasses are removed. The glasses are hospital-safe, disinfectable, and the game can be played with headphones, using eye movements to interact with objects in the immersive scenarios.
The project was approved by the institutional Ethics Committee in December 2022 (under opinion no. 5.790.508), in accordance with resolution no. 466/2012 of the Brazilian National Health Council.
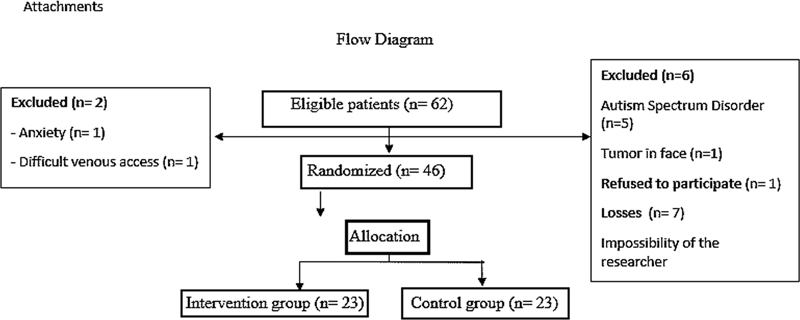
Fig. 1 Flow diagram of the study.
During the collection period, most patients attending their first consultation were invited to participate, with the exception of seven who were not approached because the researcher was not available at the time. There were two exclusions: the first was a patient with a previous diagnosis of anxiety, who, when trying the VR glasses, realized that it would not be possible to perform the collection without visually accompanying the procedure; therefore, this subject chose not to participate; the second exclusion was that of a patient with difficulty in terms of venous access, who needed another professional to complete the collection after two attempts with VR glasses, making it impossible to continue the intervention. Even so, this patient reported that the collection occurred in a quiet way, as they were used to multiple attempts.
The collection was carried out with 46 participants. With 23 participants per group, the study has 80% power to detect a standardized effect of Cohen's d = 0.845. Consequently, the study was adequately sensitive only to large-magnitude effects; medium- or small-magnitude effects may not have been detected. Therefore, non-significant results should be interpreted with caution. The study was discontinued before reaching the planned sample size due to the completion of the author's nursing residency.
| Intervention group | Control group | |||
|---|---|---|---|---|
| Sex: n (%) | ||||
| Male | 11 (47.9) | 12 (52.1) | ||
| Female | 12 (52.1) | 11 (47.9) | ||
| Mean age (years) | 12.56 ± 2.78 | 11.17 ± 2.55 | ||
| Already had a diagnosis: n (%) | ||||
| Yes | 9 (39.1) | 10 (43.5) | ||
| Not | 14 (60.9) | 13 (56.5) | ||
| Companion: n (%) | ||||
| Mother | 22 (95.7) | 20 (87) | ||
| Father | 1 (4.3) | 1 (4.3) | ||
| Others | − | − | 2 (8.7) | |
| Companion's level of schooling: n (%) | ||||
| Did not attend school | − | − | 1 (4.3) | |
| Incomplete elementary education | 1 (4.3) | 3 (13.1) | ||
| Complete elementary education | 4 (17.4) | 2 (8.7) | ||
| High school graduate | 14 (60.9) | 15 (65.2) | ||
| College graduate | 4 (17.4) | 2 (8.7) | ||
Both groups showed a homogeneous distribution in relation to sex. Regarding the companions, 42 patients (92%) were accompanied by their mothers.
| Control group: n (%) | Intervention group: n (%) | ||||
|---|---|---|---|---|---|
| p-value | |||||
| Are you feeling pain right now? | |||||
| Yes | 2 (8.7) | 5 (21.7) | 0.414 | ||
| No | 21 (91.3) | 18 (78.3) | |||
| Have you ever collected blood in other institutions? | |||||
| Yes | 23 (100) | 23 (100) | − | ||
| No | − | − | |||
| Do you feel pain when taking blood? | |||||
| Yes | 13 (56.5) | 16 (69.5) | 0.541 | ||
| No | 10 (43.5) | 7 (30.5) | |||
| Are you feeling anxious about the doctor's appointment now? | |||||
| Yes | 16 (69.5) | 18 (78.3) | 0.737 | ||
| No | 7 (30.5) | 5 (21.7) | |||
In the intervention group, 20 participants (87%) reported having heard of VR glasses; 100% of them said they liked games.
| Control group: n (%) | Intervention group: n (%) | p-value | |||
|---|---|---|---|---|---|
| Did you feel pain in the blood collection? | |||||
| Yes | 13 (56.5) | 14 (60.9) | 1 | ||
| No | 10 (43.5) | 9 (39.1) | |||
| If yes, with 0 meaning “no pain” and 10, “the worst pain you have ever felt in your life”, what level of pain did you feel in the exam collection? | Mean: 4.84 ± 2.1 | Mean: 4.57 ± 2.2 | 0.744 | ||
| Are you feeling anxious about the doctor's appointment now? | |||||
| Yes | 16 (69.5) | 10 (43.5) | 0.137 | ||
| No | 7 (30.5) | 13 (56.5) | |||
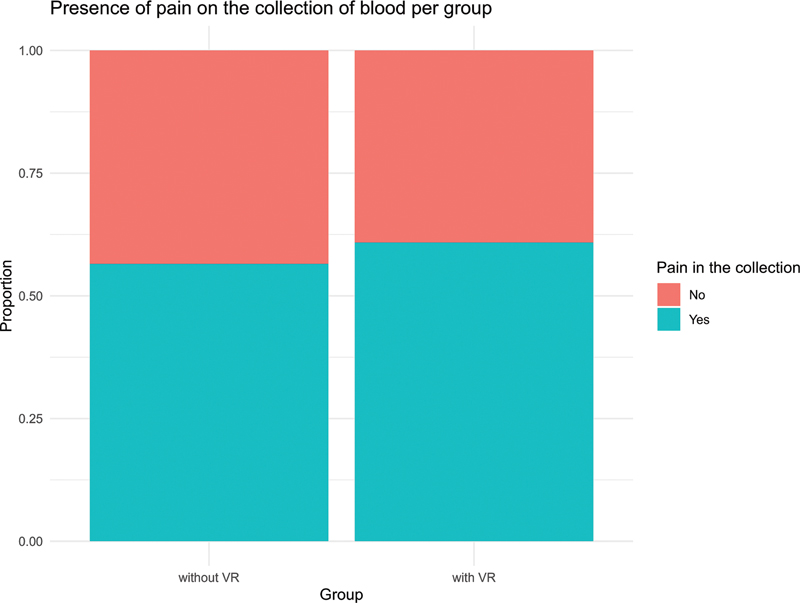
During the blood collection itself, 10 participants in the control group reported no pain, compared with 9 in the intervention group.
Fig. 2 Comparison of the presence of pain in the blood collection.
No association was observed between sex and the presence of pain (controls: p = 1; intervention group: p = 0.68), previous diagnosis (controls: p = 1; intervention group: p = 0.38), or participant age (controls: p = 0.476; intervention group: p = 0.989). Likewise, pain before the procedure was not associated with pain during collection (controls: p = 1; intervention group: p = 0.723).
It is important to note that the sample size was smaller than originally planned due to logistical limitations. The reduced number of participants may have lowered the statistical power of the analyses, potentially masking clinically-relevant differences between the groups.
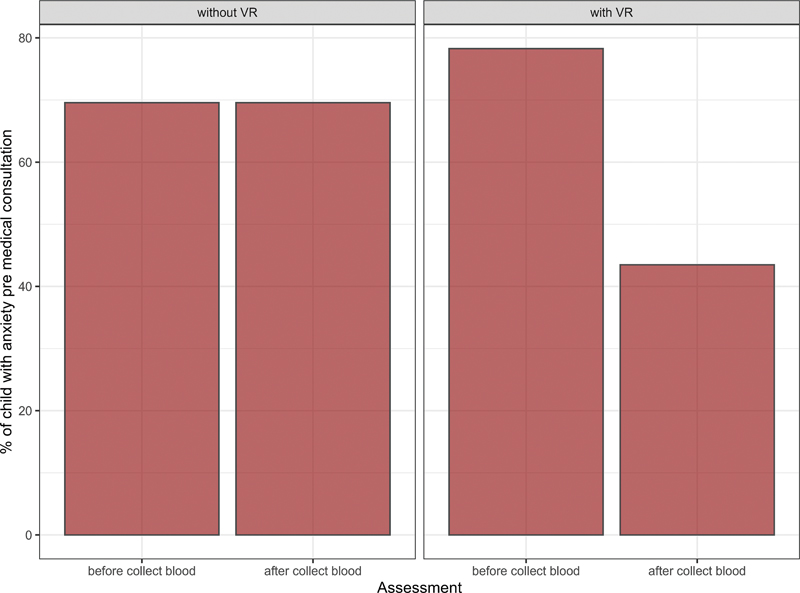
During the precollection questionnaire, there was no significant relationship between the participants' age and the presence of anxiety in either group (controls: p = 0.969; intervention group: p = 0.827). In the postcollection questionnaire, age had a significant association with anxiety in the control group (p = 0.049), but not in the intervention group (p = 0.573).
The sex of the participants had no significant influence on the presence of anxiety, either before or after collection, as evidenced by high p-values in both groups (precollection: p = 0.66 for the controls, and p = 0.64 for the intervention group; postcollection: p = 1.00 for the controls, and p = 0.68 for the intervention group). Similarly, there was no association between the presence of anxiety and the diagnostic history of the participants, with non-significant results in the pre- (controls: p = 0.405; intervention group: p = 1.00) and postcollection questionnaires (controls: p = 0.65; intervention group: p = 0.413).
In
Fig. 3 Comparison of premedical consultation anxiety before and after the blood collection between the groups.
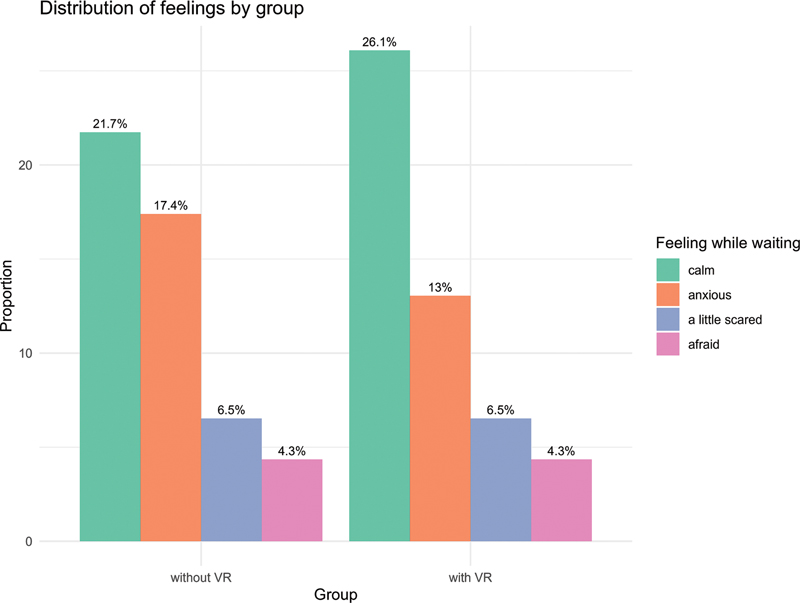
The anxiety of waiting was evaluated in two moments: during the waiting to be called and at the moment when the nurse called them. The waiting time for blood collection could vary according to the number of research participants in the day and the patient's call order for the previous evaluation. The waiting time varied from 20 minutes to 1 hour. There was no significant association regarding feelings in either group, with a p-value of 0.964 while they were waiting, and of 0.902 and when they were called.
Fig. 4 Comparison of the feelings while waiting between the groups.
Fig. 5 Comparison of the feelings when a nurse called betweenthe groups.
Patients in the intervention group were asked about adverse reactions to the use of VR glasses, such as nausea, vomiting, or headache, and 20 patients (87%) answered that they did not feel anything, while 3 (13%) reported having one of these symptoms.
Patients' responses to the intervention evaluation questionnaire showed statistical significance, indicating that they perceived a positive difference when using the VR headset compared with not using it. The question was asked so that the participants could compare this experience to previous experiences in other institutions. Moreover, when asked about their perception of the use of glasses, 100% stated they enjoyed the VR glasses, none found the game difficult, 91,3% said they think that they played well, and, when asked if they think it makes any difference to collect blood with VR, 82,6% said “yes”.
The companions' perception of pain during blood collection did not differ significantly between the groups. When asked if they thought their child/adolescent experienced pain, 9 companions in the control group and 4 in the intervention group answered “yes” (p = 0.189).
In the intervention group, 22 companions (95.7%) reported that the VR glasses were beneficial to the child/adolescent. In the descriptive thematic analysis of these responses, we identified 3 main categories: 11 companions reported that VR promoted calmness or reduced nervousness, 5 noted it provided distraction during collection, and 7 indicated that the tool “did well” or reduced the pain perceived.
The results of the present study corroborate the initial hypothesis that the use of VR can reduce medical preconsultation anxiety in children undergoing large-volume blood collections at their first diagnostic appointment. These findings are comparable to previous studies
In a systematic review of randomized clinical trials using VR to control cancer symptoms, Uçgun and Çitak
Consistent with other studies,
The descriptive qualitative analysis of the companions' responses revealed perceptions of well-being, distraction, and reduced nervousness, indicating relief of anxiety for patients and companions during collection. In the control group, age showed an inverse association with postcollection anxiety, whereas no such effect was observed in the intervention group, suggesting that VR may equalize the experience across age groups.
Anxiety related to diagnostic tests, popularly called scanxiety, was first described in 2011; since then, several studies have investigated the phenomenon. Literature reviews
In the current study, 100% of the patients in the intervention group reported having enjoyed using VR glasses; 82.6% noticed a difference during collection when using the feature. Virtual reality applications have been expanding, ranging from serious games for treatment to various distraction tools. Evidence suggests that interventions in which the patient actively participates generate a greater distraction effect than passive activities, such as merely watching a video.
Although 13% of the patients in the present study reported nausea during the use of VR glasses–an expected effect due to the sensitivity of part of the population to visual and auditory stimuli involving movement (motion sickness)
The limitations to the study are the exclusion of patients due to difficult venous access or heightened anxiety during collection, situations in which the researcher could not perform the procedure, the absence of a validated anxiety questionnaire, and the variable interpretation of the term “anxiety” according to age and previous experiences.
Virtual reality in prediagnosis blood collection in children with cancer reduced anxiety and was well accepted, but it did not significantly affect pain. The intervention showed potential to improve the emotional experience. These results support the implementation of VR as a complementary resource in pediatric cancer care.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Uçgun, T and Çitak, E A. Virtual reality for cancer symptom management: a systematic review of randomized controlled trials. Support Care Cancer [online]. 2025, vol. 33, p. 672. https://doi.org/10.1007/s00520-025-09738-6 Ver referência
2. Cheng, Z and Yu, S and Zhang, W and Liu, X and Shen, Y and Weng, H. Virtual reality for pain and anxiety of pediatric oncology patients: A systematic review and meta-analysis. Asia Pac J Oncol Nurs [online]. 2022, vol. 9, p. 100152. https://doi.org/10.1016/j.apjon.2022.100152 Ver referência
3. Tutelman, P R and Chambers, C T and Stinson, J N. Pain in Children With Cancer: Prevalence, Characteristics, and Parent Management. Clin J Pain [online]. 2018, vol. 34, p. 198-206. https://doi.org/10.1097/AJP.0000000000000531 Ver referência
4. Loeffen, E AH and Mulder, R L and Font-Gonzalez, A. Reducing pain and distress related to needle procedures in children with cancer: A clinical practice guideline. Eur J Cancer [online]. 2020, vol. 131, p. 53-67. https://doi.org/10.1016/j.ejca.2020.02.039 Ver referência
5. Mandrell, B N and Baker, J and Levine, D. Children with minimal chance for cure: parent proxy of the child's health-related quality of life and the effect on parental physical and mental health during treatment. J Neurooncol [online]. 2016, vol. 129, p. 373-381. https://doi.org/10.1007/s11060-016-2187-9 Ver referência
6. Gao, Y and Xu, Y and Liu, N and Fan, L. Effectiveness of virtual reality intervention on reducing the pain, anxiety and fear of needle-related procedures in paediatric patients: A systematic review and meta-analysis. J Adv Nurs [online]. 2023, vol. 79, p. 15-30. https://doi.org/10.1111/jan.15473 Ver referência
7. Comparcini, D and Simonetti, V and Galli, F. Immersive and Non-Immersive Virtual Reality for Pain and Anxiety Management in Pediatric Patients with Hematological or Solid Cancer: A Systematic Review. Cancers (Basel) [online]. 2023, vol. 15, p. 985. https://doi.org/10.3390/cancers15030985 Ver referência
8. Eccleston, C and Crombez, G. Pain demands attention: a cognitive-affective model of the interruptive function of pain. Psychol Bull [online]. 1999, vol. 125, p. 355-366. https://doi.org/10.1037/0033-2909.125.3.356 Ver referência
9. Atzori, B and Hoffman, H G and Vagnoli, L. Virtual Reality Analgesia During Venipuncture in Pediatric Patients With Onco-Hematological Diseases. Front Psychol [online]. 2018, vol. 9, p. 2508. https://doi.org/10.3389/fpsyg.2018.02508 Ver referência
10. Manzini, E J. A entrevista na pesquisa social. Didática [online]. , vol. 26/27, p. 149-158.
11. Moura, B F and Imparato, J CP and Parisotto, T M and Benedetto, M D. Child's anxiety preceding the dental appointment: evaluation through a playful tool as a conditioning feature. RGO Rev Gaúch Odontol [online]. 2015, vol. 63, p. 455-460.
12. Molina, C J and Valls, L L and Villegas, V F and Ruiz, S S. Nursing evaluation of pediatric preoperative anxiety: a qualitative study. Rev Lat Am Enfermagem [online]. 2023, vol. 31, p. e3738. https://doi.org/10.1590/1518-8345.6230.3738 Ver referência
13. Beltramini, A and Milojevic, K and Pateron, D. Pain Assessment in Newborns, Infants, and Children. Pediatr Ann [online]. 2017, vol. 46, p. e387-e395. https://doi.org/10.3928/19382359-20170921-03 Ver referência
14. Sandelowski, M. Whatever happened to qualitative description?. Res Nurs Health [online]. 2000, vol. 23, p. 334-340. https://doi.org/10.1002/1098-240x(200008)23:43.0.co;2-g Ver referência
15. Brasil. Conselho Nacional de Saúde. Resolução n° 466, de 12 de dezembro de 2012. ; Revoga as (RES. 196/96); (RES. 303/00); (RES. 404/08). Brasília: Diário Oficial da União; [online]. Available from: <https://www.gov.br/conselho-nacional-de-saude/pt-br/atos-normativos/resolucoes/2012/resolucao-no-466.pdf/view>.
16. Piskorz, J and Czub, M. Effectiveness of a virtual reality intervention to minimize pediatric stress and pain intensity during venipuncture. J Spec Pediatr Nurs [online]. 2018, vol. 23, p. e12201. https://doi.org/10.1111/jspn.12201 Ver referência
17. [Ph.D. thesis (Sciences)]. Ribeirão Preto: Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo; . [cited 2025 Aug 6]; [online]. Available from: <>. Ver referência
18. Bui, K T and Liang, R and Kiely, B E and Brown, C and Dhillon, H M and Blinman, P. Scanxiety: a scoping review about scan-associated anxiety. BMJ Open [online]. 2021, vol. 11, p. e043215. https://doi.org/10.1136/bmjopen-2020-043215 Ver referência
19. In: Anais Estendidos do XXIII Simpósio Brasileiro de Computação Aplicada à Saúde. Porto Alegre: Sociedade Brasileira de Computação (SBC); :102–107 [cited 2025 Aug 6] [online]. Available from: <>. Ver referência
20. Herrera, M DLC and Fuster-Casanovas, A and Catalina, Q M. Use of virtual reality in the reduction of pain after the administration of vaccines among children in primary care centers in Central Catalonia: Randomized clinical trial. PLoS One [online]. 2025, vol. 20, p. e0322840. https://doi.org/10.1371/journal.pone.0322840 Ver referência
21. Chun, G YC and Neves, NSdS and Fortes, C C and Nishino, L K and Santos, MAdO. Avaliação do desconforto sensorial causado por estimulação com realidade virtual em voluntários com e sem cinetose. Audiol Commun Res [online]. 2023, vol. 28, p. e2680. https://doi.org/10.1590/2317-6431-2022-2680pt Ver referência
Dados de acesso insuficientes para visualização no mapa.