Breast cancer is one of the most common cancers in women worldwide,
We have recently verified the switchability between the reference and a generic tamoxifen formulation prescribed to breast cancer patients at the Brazilian National Cancer Institute (INCA).
This study was conducted following Good Clinical Practice (ICH-GCP) and the clinical protocol was approved by INCA’s Ethics Committee (CAAE: 26125819.4.0000.5274).
Postmenopausal women (n=33), aged 50-84 years, with ER+ breast cancer, were recruited at INCA and provided written, informed consent. Self-reported race/color, according to the Brazilian census, was as follows: White, 15; Brown (Pardo in Brazilian Portuguese), 14; Black, 4. Individual weight averaged 71.9kg (range 46-92kg). At the beginning of the study, all patients had been receiving daily doses of anastrozole (1mg p.o.) for a minimum of 3 months, as part of their adjuvant treatment.
This open label study comprised three consecutive phases of 8-10 days each. A bracketed design was adopted, such that the test anastrozole formulation in current use at our institution (Anya, Sun Farmacêutica do Brasil Ltda., 1mg tablets, batch JKX1371A) was provided in phases 1 and 3, whereas in phase 2 the patients were given the reference anastrozole formulation (Arimidex®, AstraZeneca do Brasil Ltda., 1mg tablets, batch 51570). In one of the last 2 days of each phase, i.e., 7-9 days after continuous use of a given formulation, a blood sample (3ml) was collected before the daily dose of anastrozole. The blood samples were centrifuged at room temperature within 15min. after collection, the plasma was separated and stored at -20°C. Anastrozole plasma concentrations were measured by liquid-chromatography tandem mass spectrometry (LC-MS/MS), as described in Supplementary information.
The through plasma concentrations of anastrozole were used to estimate the genetic component of pharmacokinetic variation, rGC, following the repeated drug administration (RDA) procedure.
One-way ANOVA was used for comparison of the through plasma concentrations of anastrozole across the three study phases, and the ř-test was used for pairwise comparisons between the reference and each test formulation. Statistical significance was set at p<0.05.
Patients referred no intercurrent adverse effects following switches of anastrozole formulations. Three blood samples were collected according to the study protocol from 30 patients; three patients had missing samples in one study phase and were excluded from the statistical analyses.
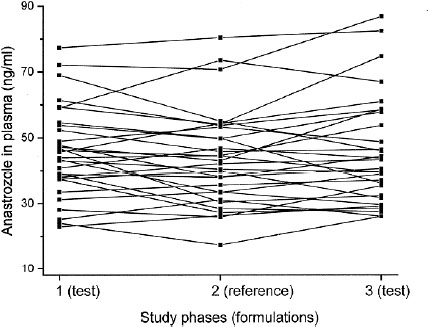
Figura 1 Plot of the individual through concentrations of anastrozole in plasma in the three study phases. The test formulation was used in phases 1 and 3, and the reference formulation was used in phase 2.
| Anastrozole concentrations (ng/ml) | Phase 1 Test | Phase 2 Reference | Phase 3 Test |
|---|---|---|---|
| Minimum | 22.9 | 17.4 | 26.1 |
| Maximum | 79.6 | 80.4 | 86.9 |
| Mean | 46.1 | 43.8 | 45.9 |
| Median | 44.8 | 42.6 | 42.0 |
| IQR1 | 38.1 | 33.4 | 33.2 |
| IQR3 | 53.4 | 52.4 | 56.8 |
We applied the RDA methodology to explore the interindividual variation in the through plasma concentrations of anastrozole. We initially compared data for phases 1 and 3, in which the same anastrozole formulation (test) was used. In a second analysis, data from the three phases were compared, based on the fact that there was no difference in the plasma concentration data for the reference and test formulations. The results of these analyses are shown in
| Anastrozole concentrations | N | rGC (CI95%) | ANOVA |
|---|---|---|---|
| Phase 1 vs. phase 3 | 30 | 0.87 (0.72-0.94) | p<0.0001 |
| Phase 1 vs. phase 2 vs. phase 3 | 30 | 0.94 (0.86-0.97) | p<0.0001 |
This is to our knowledge the first postmarketing surveillance trial of anastrozole in Brazilian patients.
Our study cohort consisted of postmenopausal women under treatment with daily anastrozole (1mg p.o.) for a minimum of three months, as part of their adjuvant treatment for ER+ breast cancer. The results indicate that the test formulation provided individual plasma concentrations of anastrozole that did not differ from the concentrations obtained with the reference formulation, thus verifying switchability between the reference and the test formulation currently used in our institution. Although not strictly a bioequivalence test, the current study has the added strength of adopting a bracketed protocol, by which patients were exposed to the test formulation before and after the switch to the reference formulation, allowing for repeated comparison of the two formulations. Accordingly, from a pharmacokinetic perspective, switching between these formulations appears to be safe. We emphasize, however, that as is the case for conventional bioequivalence tests, the present results apply specifically to the batches tested and do not guarantee bioequivalence for other batches of the reference and/or other similar or generic products. We are aware that our results derive from single, rather than serial blood samples, as is commonly performed in bioequivalence trials. Nevertheless, in all phases of this study the blood samples were collected >7 days of daily intake of anastrozole, which assures achievement of steady-state pharmacokinetics of this drug.
We found no data for Brazilian women under treatment with anastrozole for comparison, but the range and interindividual variability of plasma concentrations for the reference formulation in this study (phase 2) is consistent with published data from North American cohorts.
In conclusion, this postmarketing surveillance trial verified the switchtability between the reference and the test anastrozole formulation currently used in our institution. The bracketed protocol adopted adds confidence to this conclusion, and may serve as a frame for future trials of postmarketing assessment of other generic and switchable similar drug products. We acknowledge as limitations of our study, the possibility of non-avowed lack of adherence to the anastrozole prescription and drug-interactions with other medications used by the patients that might influence anastrozole disposition.
Individual data of the through plasma concentrations of anastrozole used to assess switchability between the test and reference formulations are shown in
MVC: Collection and assembly of data, Final approval of manuscript, Provision of study materials or patient.
RO: Collection and assembly of data, Final approval of manuscript, Provision of study materials or patient
LS: Collection and assembly of data, Final approval of manuscript, Provision of study materials or patient
PP: Collection and assembly of data, Final approval of manuscript, Provision of study materials or patient
RL: Collection and assembly of data, Final approval of manuscript
VCF: Collection and assembly of data, Final approval of manuscript
ACM: Data analysis and interpretation, Final approval of manuscript, Manuscript writing
GSK: Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
Anastrozole was extracted from plasma by adding 50µL of sample to a plastic microtube followed by the addition of 200µL of acetonitrile containing the internal standard (anastrozol-d12 15ng/mL). The mixture was vortex-mixed and centrifuged. Afterwards, a aliquot of 1µL of the supernatant was injected into the liquid-chromatography tandem mass spectrometry (LC-MS/MS) system. The LC-MS/MS was a Acquity I-Class coupled to a Xevo TQS triple quadrupole mass spectrometer, from Waters (Milford, USA). The chromatographic separation was performed in a Acquity BEH C8 (100x2.1mm, 1.7μm) column, from Waters. The column was kept at 35ºC. Elution was performed in gradient modo, with mobile phases composed of water with 0.1% formic acid (mobile phase A) and acetonitrile with 0.1% formic acid (mobile phase B). The gradient program was as follows: 95% of A for 1min., followed by a linear gradient to 10% in 3min., which was hold for 1min., and then returning to initial conditions in 4.1min. Total run time was 6min. Mobile phase flow rate was 0.3mL/min. Electrospray ionization in positive mode was used, with capillary voltage of 1kV, ionization source temperature of 500ºC, desolvatation gas flow of 900L/h, cone gas flow of 50L/h, and source temperature of 150ºC. The following MRM transitions were monitored for anastrozole: 294.1 to 115.05 (quantification) and 294.1 to 225.15 (qualification), with cone voltage of 35V and collision energies of 58 and 22V, respectively. The MRM transition of anastrozole-d12 was 306.15 to 237.25, with cone energy of 35V and collision energy of 20V. The assay is linear from 1 to 200ng/mL, with intra-assay precision of 3.9-6.9%, inter-assay precision of 2.4-5.8%, and accuracy from 94.3-102.6%. Matrix effect was 5.5%.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. World Health Organization (WHO0. International Agency for Research on Cancer (IARC). Home [Internet]. WHO/IARC, 2022.
2. Instituto Nacional de Câncer (INCA). Incidência [Internet]. INCA, 2022.
3. ATAC Trialists’ Group. ‘Arimidex’ (anastrozole) versus tamoxifen as adjuvant therapy in postmenopausal women with early breast cancer-efficacy overview. J Steroid Biochem Mol Biol [online]. 2003, vol. 86, p. 399-403. https://doi.org/10.1016/s0960-0760(03)00350-9 Ver referência
4. Santen, RJ and Brodie, H and Simpson, ER and Siiteri, PK and Brodie, A. History of aromatase: saga of an important biological mediator and therapeutic target. Endocr Rev [online]. 2009, vol. 30, p. 343-75. https://doi.org/10.1210/er.2008-0016 Ver referência
5. Agência Nacional de Vigilância Sanitaria (ANVISA). Medicamentos similares [Internet]. ANVISA, 2022.
6. Yang, YT and Nagai, S and Chen, BK and Qureshi, ZP and Lebby, AA and Kessler, S. Generic oncology drugs: are they all safe?. Lancet Oncol [online]. 2016, vol. 17, p. e493-e501. https://doi.org/10.1016/S1470-2045(17)30016-5 Ver referência
7. Ximenez, JP and Lanchote, VL and Bello, MA and Iocken, FHS and Obadia, RCM and Sousa, VP. Post-marketing assessment of generic tamoxifen in Brazilian breast cancer patients. Basic Clin Pharmacol Toxicol [online]. 2020, vol. 126, p. 432-6. https://doi.org/10.1111/bcpt.13368 Ver referência
8. Instituto Nacional de Câncer (INCA). Institucional [Internet]. INCA, 2021.
9. Kalow, W and Endrenyi, L and Tang, BK. Repeat administration of drugs as a means to assess the genetic component of pharmacological variability. Pharmacology [online]. 1999, vol. 58, p. 281-4.
10. Ozdemir, V and Kalow, W and Tang, BK and Paterson, AD and Walker, SE and Endrenyi, L. Evaluation of the genetic component of variability in CYP3A4 activity: a repeated drug administration method. Pharmacogenetics [online]. 2000, vol. 10, p. 373-88. https://doi.org/10.1097/00008571-200007000-00001 Ver referência
11. Buzdar, AU and Robertson, JF and Eiermann, W and Nabholtz, JM. An overview of the pharmacology and pharmacokinetics of the newer generation aromatase inhibitors anastrozole, letrozole, and exemestane. Cancer [online]. 2002, vol. 95, p. 2006-16. https://doi.org/10.1002/cncr.10908 Ver referência
12. Dudenkov, TM and Liu, D and Cairns, J and Devarajan, S and Zhuang, Y and Ingle, JN. Anastrozole aromatase inhibitor plasma drug concentration genome-wide association study: functional epistatic interaction between SLC38A7 and ALPPL2. Clin Pharmacol Ther [online]. 2019, vol. 106, p. 219-27. https://doi.org/10.1002/cpt.1359 Ver referência
13. Ingle, JN and Kalari, KR and Buzdar, AU and Robson, ME and Goetz, MP and Desta, Z. Estrogens and their precursors in postmenopausal women with early breast cancer receiving anastrozole. Steroids [online]. 2015, vol. 99, p. 32-8. https://doi.org/10.1016/j.steroids.2014.08.007 Ver referência
Dados de acesso insuficientes para visualização no mapa.