Testicular cancer, although a rare neoplasm, is a relevant condition for the young male population, because it is the most common cancer among men aged 20 to 40 years.
This neoplasm has a predilection for lymphatic dissemination to the retroperitoneal lymph nodes. Thus, retroperitoneal lymph node dissection (RLND) is essential in the treatment when patients present with lymph node metastasis. This is especially true when the procedure is performed for resection of residual lymph node masses after systemic chemotherapy.
Instituto Nacional de Câncer (INCA), in Rio de Janeiro, Brazil, is the referral hospital for the treatment of patients with testicular tumors in the state, and it receives many patients with this pathology. Therefore, the hospital performs many RLND surgeries to treat residual retroperitoneal lymph node masses after chemotherapy. At INCA, from 1999 to 2019, 120 postchemotherapy (PC) open RLNDs were performed to treat metastatic testicular tumors. Historically, RLND in this hospital was performed using an open approach. This is major surgery, with a prolonged postoperative recovery and a considerable complication rate, which ranges from 30 to 36%
Robot-assisted RLND (RARLND) was first described in 2006. Worldwide, many reports have demonstrated the safety, oncological efficacy, lower rates of complications and morbidity, and shorter hospital stays of RARLND compared with the open technique.
Robotic surgery was initiated at INCA in 2012. Over the years, increasingly complex surgeries have been performed with robotic platforms using this technique. Recently, RARLND has been used to treat testicular cancer. The hospital has performed this surgery in five cases, with excellent results. In the present study, we retrospectively evaluated the peri- and postoperative outcomes of RARLND in patients at INCA.
In the current observational and descriptive study, we retrospectively evaluated data contained in medical records. The five patients who underwent RARLND for the treatment of residual retroperitoneal testicular tumor masses after chemotherapy were included and evaluated retrospectively.
Pre-, peri-, and postoperative data were collected from each patient. The data included age, size of the residual retroperitoneal mass, histopathological report of lymphadenectomy, operative time, estimated bleeding, duration of drainage, hospital stay, readmissions, and complications within the first 30 days after surgery.
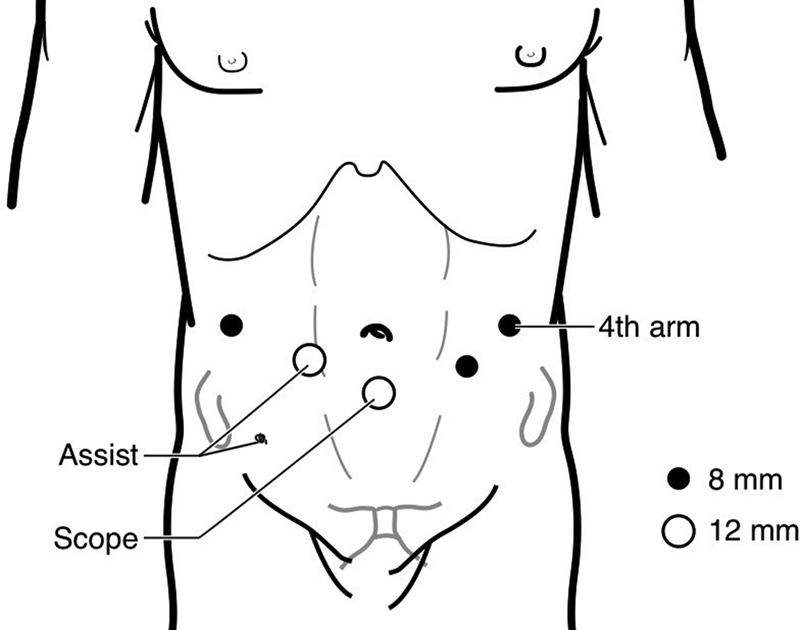
All surgeries were performed using the Da Vinci Si robotic platform (Intuitive Surgical, Inc., Sunnyvale, CA, United States). The surgery was performed transperitoneally, with the patient in the supine position under general anesthesia. The surgical procedure began with an infraumbilical incision in the midline, with the creation of a pneumoperitoneum and placement of a 12-mm trocar, through which a robot camera was positioned. Three additional robotic trocars were placed, as well as two additional trocars for the auxiliary surgeon (
Fig. 1 Trocar configuration for the approach with the Da Vinci Si robotic platform.
Surgery began by incising the posterior leaflet of the retroperitoneum under the terminal ileum, approximately 15 cm from the ileocecal valve, with access to the retroperitoneum and the vena cava. The cranial dissection proceeded over the vena cava to the duodenum and renal hilum, with cranial mobilization of intestinal loops and fixation of the free edge of the posterior peritoneum to the anterior abdominal wall with 2-0 monofilament suture. This maneuver is called the “puppet” technique. Lymph node dissection began with dissection of residual lymph node mass and excision of adjacent lymph nodes.
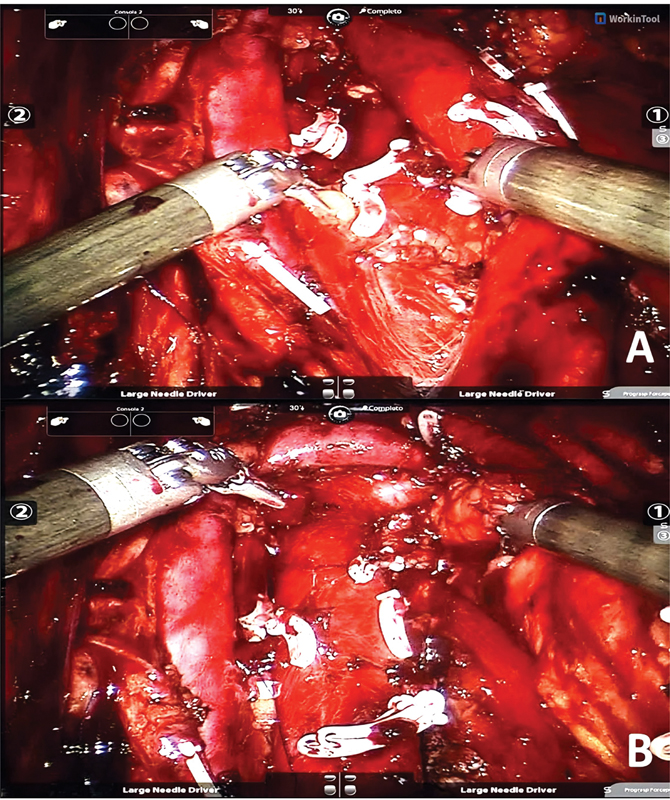
We dissected the paracaval lymph nodes from caudal to cranial, from the right common iliac bifurcation to the renal hilum, with the right ureter as a lateral limit. Subsequently, the interaortocaval lymph nodes and remaining para-aortic lymph nodes were dissected. The left ureter was the lateral limit. (
Fig. 2 (A) Dissection of interaortocaval lymph nodes in one patient. (B) Appearance at the end of the retroperitoneal lymph node dissection.
After reviewing hemostasis, when indicated, an intra-abdominal suction drain was placed (
The main outcomes analyzed were the intraoperative complication rate, estimated blood loss, operative time, duration of the abdominal drainage, length of hospital stay after surgery, complication rate during first 30 postoperative days, and hospital readmission rate. The variables and outcomes were expressed as values of medians with standard error.
These outcomes were compared with those observed in INCA patients undergoing conventional open surgery based on a recently-published retrospective study,3 as well as results from other cases of robot-assisted retroperitoneal lymphadenectomy available in the global literature. The present study was approved by the Ethics Committee of INCA under the following registration number: 55720422.7.0000.5274.
From August 2020 to November 2021, 5 RARLND surgeries were performed for the resection of residual retroperitoneal masses of testicular tumors after chemotherapy.
The mean age of the patients at the time of diagnosis was of 49.4 years. Currently, all patients are alive. The mean follow-up was of 6.4 months. The mean size of the resected mass was of 7.28 cm, with 60% of positivity for active neoplasia.
| Median | Standard error | |
|---|---|---|
| Age (years) | 37 | 6.12 |
| Mass size (cm) | 7.0 | 0.41 |
| Operative time (minutes) | 288 | 28.8 |
| Estimated blood loss (mL) | 180 | 50 - 400 |
| Duration of drain placement (days) | 1.0 | 0.50 |
| Length of hospital stay (days) | 3.0 | 0.58 |
| Complications within 30 days (%) | 0 | − |
Intraoperative complications were not observed, and the mean duration of the surgical procedure was of 307.4 (range: 253–414) minutes. The average estimated blood loss was of 180 (range: 50–400) mL. There was no need for intraoperative or postoperative blood transfusions.
Except for one patient, the abdominal suction drain was left in place at end of the surgery. The mean duration of drain placement was of 1.4 (range: 1–3) days. The mean length of hospital stays after surgery was of 3.2 (range: 2–5) days. No patient developed postoperative ileus.
The complication rate during the first 30 postoperative days was of 0%, and there were no hospital readmissions during this period. Data on the perioperative outcomes are summarized in
Regarding the results of the anatomopathological studies of the resected surgical specimens, we identified an active malignant neoplasm, a malignant mesenchymal neoplasm, an adenocarcinoma, and a neoplasm with an epithelial component in 3 patients (60%). In the other 2 patients (40%), the resected material consisted of lymph nodes with a focus of necrosis, without active neoplasia. The histopathological data are summarized and correlated with surgical time in
| Primary tumor | Lymph node dissection | Operative time (minutes) | |
|---|---|---|---|
| Patient 1 | Yolk sac | Mesenchymal malignant neoplasm | 256 |
| Patient 2 | Teratoma | Adenocarcinoma | 253 |
| Patient 3 | Seminoma | Necrosis | 317 |
| Patient 4 | Yolk sac | Neoplasm with epithelial component | 288 |
| Patient 5 | Yolk sac | Necrosis | 414 |
To date, no patient has received adjuvant chemotherapy after RLND. All patients are alive, without evidence of testicular tumor recurrence in the retroperitoneum or symptomatic lymphocele.
Advanced testicular tumors, unlike other neoplasms, present a high therapeutic response rate and long-term survival. This is true only if the intervention is initiated early and appropriately in combination with chemotherapy and surgery. The RLND procedure is an essential component of the treatment of patients with testicular tumors with residual retroperitoneal lymph node masses after chemotherapy, especially those with non-seminomatous germ cell tumors (GCTs).
Residual PC non-seminomatous GCT masses larger than 1 cm have a 45% probability of presenting a teratoma and a 15% probability of presenting a viable malignant tumor. Thus, RLND is recommended in these cases.
In case of seminomatous tumors, resection of a residual retroperitoneal lymph node mass after chemotherapy has a more restricted indication. In addition to being technically more difficult surgery, the percentage of viable tumors in this scenario is quite low. Thus, residual masses in seminomatous tumors smaller than 3 cm can be followed up. The larger masses should preferably undergo imaging exams through fludeoxyglucose F18 positron emission tomography-computed tomography (FDG PET-CT). Resection is indicated in cases of a positive uptake.
Residual-mass RLND surgery after chemotherapy is considered challenging even when performed by an experienced surgeon at a high-volume center. The conventional open RLND technique is associated with high morbidity and prolonged postoperative recovery. In the literature, this technique is associated with a general complication rate that can reach 50%.
The first RARLND was performed in 2006 by Patrick Davol in Pennsylvania. Since then, it has been disseminated worldwide, with encouraging results. Globally, several case series with a small number of patients have demonstrated acceptable operative times, lower levels of intraoperative bleeding, and shorter hospital stays, compared with those in the conventional technique. Most published series included patients who underwent primary retroperitoneal lymphadenectomy. Recently, robotic techniques have been extrapolated to include PC residual-mass resection, with favorable results.
The PC-RARLND case series by Kamel et al., published in 2016, included 12 patients, with a mean operative time of 312 minutes and a mean estimated blood loss of 475 mL. Only one patient had a major complication (Clavien-Dindo grade 3).
The largest case series available in the literature in this PC setting was published in 2021 in the World Journal of Urology by Abdul-Mushin et al.
In the present case series, RARLND was related to brief hospital stays after surgery and low mean intraoperative bleeding. Additionally, there were no intraoperative complications, nor complications in first 30 days; neither were there hospital readmissions.
In comparison with other case series in the global literature,
We compared the perioperative outcomes of our patients undergoing RARLND with those of patients who underwent the conventional open technique at our institution. This comparison was based on the results of another retrospective study conducted BY Souza3 in 2020 that included 120 patients who underwent surgery between 1999 and 2019.
It is very difficult to reliably compare the present study with the one conducted by Souza3 due to their differences in the number of patients and the fact that open surgery was performed in patients with retroperitoneal masses of varying sizes, which included severe disease. In addition, RARLND patients may be super-selected for the initial procedures. However, we can observe that the minimally-invasive technique resulted in a considerably-shorter hospital stay after surgery, of 3.2 days, compared to the 6.63 days observed with the conventional open technique. Regarding the complications, Souza3 reported rates of 13.3% of peri- and postoperative complications, compared to 0% in the present study.
| Mean | Range | ||||
|---|---|---|---|---|---|
| Age (years) | 27.0 | 34 | |||
| Length of hospital stay (days) | 6.63 | 52 | |||
| Complications: Clavien-Dindo grade | I | II | III | IV | V |
| Complications (n) | 0 | 2 | 12 | 2 | 0 |
The present study has limitations, including its retrospective design, the small number of patients, and the short follow-up period. Thus, a larger sample size and longer follow-up are necessary to draw definitive conclusions regarding this technique. We intend to publish updates and record additional experiences regarding this technique, and we also intend to conduct a study including a larger number of patients with a longer follow-up
In addition, another limitation of the current study is that the patients may have been super-selected. Thus, these results may not necessarily reflect reality. An update on this population with more heterogeneous patients is needed to draw definitive conclusions.
Despite being an initial experience, we believe that dissemination of these results will be of interest to the urological community, given the rarity of this surgical procedure using the robotic technique, especially in the scenario of resection of a residual retroperitoneal mass after chemotherapy. The largest studies in this scenario in the world literature included a maximum of 30 to 40 patients with collaboration between hospitals. Most publications include an average of 5 to 10 patients.
In 2017, Torricelli et al.
As it is a fundamental surgery to treat certain patients with advanced testicular tumors, RLND is of marked importance. In this scenario, greater use of the robotic technique may reduce morbidity and possible surgical sequelae in young patients with a long life expectancy.
In the literature, encouraging results have been reported for RARLND.
Despite the fact that the robotic approach is more expensive than the conventional approaches, the reduction in the rate of complications and length of hospital stay may counterbalance the cost and make the minimally-invasive technique more attractive to the Brazilian Unified Health System (Sistema Único de Saúde, SUS, in Portuguese).
The adequate selection of patients who will undergo the procedure through the robotic technique is essential according to the surgeon's experience and point on learning curve. Finally, we emphasize that, with the results herein reported, we cannot conclude that the robotic approach is superior to the conventional surgery; moreover, studies with larger sample sizes and longer follow-ups are necessary to draw definitive conclusions regarding this technique.
In conclusion, the present study highlights the safety and lower morbidity of RARLND, which may increase the acceptance and use of this technique. This would benefit patients, and it may help optimize the allocation of resources in SUS.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. National Cancer Institute. Bethesda, MD, 2017. , based on November 2016 SEER data submission, posted to the SEER web site, April [online]. Available from: <https://seer.cancer.gov/csr/1975_2014/>.
2. Rajpert-De Meyts, E and McGlynn, K A and Okamoto, K and Jewett, M AS and Bokemeyer, C. Testicular germ cell tumours. Lancet [online]. 2016, vol. 387, p. 1762-1774.
3. . Linfadenectomia retroperitoneal pós-quimioterapia no tratamento do câncer de testículo metastático: a série de casos de um centro oncológico no Brasil. Tese (Pós-graduação em urologia em oncologia) – Instituto Nacional de Câncer, Rio de Janeiro, :27 [online]. Available from: <>.
4. Chalfin, H J and Ludwig, W and Pierorazio, P M and Allaf, M E. Robotic primary RPLND for stage I testicular cancer: a review of indications and outcomes. Curr Urol Rep [online]. 2016, vol. 17, p. 41.
5. Hanna, N H and Einhorn, L H. Testicular cancer–discoveries and updates. N Engl J Med [online]. 2014, vol. 371, p. 2005-2016.
6. Rice, K R and Beck, S D and Bihrle, R and Cary, K C and Einhorn, L H and Foster, R S. Survival analysis of pure seminoma at post-chemotherapy retroperitoneal lymph node dissection. J Urol [online]. 2014, vol. 192, p. 1397-1402.
7. Davol, P and Sumfest, J and Rukstalis, D. Robotic-assisted laparoscopic retroperitoneal lymph node dissection. Urology [online]. 2006, vol. 67, p. 199.
8. Kamel, M H and Littlejohn, N and Cox, M and Eltahawy, E A and Davis, R. Post-Chemotherapy robotic retroperitoneal lymph node dissection: institutional experience. J Endourol [online]. 2016, vol. 30, p. 510-519.
9. Abdul-Muhsin, H and Rocco, N and Navaratnam, A. Outcomes of post-chemotherapy robot-assisted retroperitoneal lymph node dissection in testicular cancer: multi-institutional study. World J Urol [online]. 2021, vol. 39, p. 3833-3838.
10. Torricelli, F CM and Jardim, D and Guglielmetti, G B and Patel, V and Coelho, R F. Robot - assisted laparoscopic retroperitoneal lymph node dissection in testicular tumor. Int Braz J Urol [online]. 2017, vol. 43, p. 171.
Dados de acesso insuficientes para visualização no mapa.