Sarcomas are rare tumors and contribute to the incidence of all cancers, accounting for less than 1% of solid tumors in adults and accounting for 12,000 cases annually in the US, with 4,700 deaths. In the childhood they are more common, reaching 15% of neoplasias.(
The main symptom of the patient is the presence of a nodule or mass, with or without pain. The symptoms resulting from distant metastatic disease are related to the implantation site.(
Five-years disease-free survival in sarcomas according to the staging are: for stage I: 86%, II: 72% and III: 52%. The overall survival over five years is 90% for I, 81% for II and 56% for stage III.(
From the above, we define those who benefit from adjuvant radiotherapy such as high grade tumors and aggressive histologies (synovial sarcoma, pleomorphic, angiosarcomas, myxofibrosarcoma). Radiotherapy is effective for sarcomas, especially in the adjuvant setting.(
Despite its rarity, sarcoma has been a model for oncology in the last 50 years, from the development of neoadjuvant chemotherapy to the organization of better management in reference centers, to the development of targeted therapies based on basic and translational research in histological types. The international collaboration of specialized reference centers will be fundamental in the coming years to improve the outcome of patients with sarcomas.(
In this context, the objective of the present research is to characterize morbimortality information related to the treatment of sarcomas. Among the information collected, demographic, clinical, histopathological and treatment aspects: toxicity, intraoperative complications and postoperative complications occurred within 30 days of the first surgery. Thus, analyzes of the possible associations between the characterization aspects of the sarcoma population and the toxicity of the therapies were made.
This is a retrospective cohort study that analyzed information obtained from patients' charts enrolled in 2017 at Barretos Cancer Hospital, State of Sao Paulo, Brazil. All data collected follow ethical standards and have approval by local ethics committee (Barretos Cancer Hospital Ethics Committee, #1349/2017).
The inclusion criteria for the study were all patients who started sarcoma treatment during the year 2017. Patients who came for second opinion only and did not proceed with the treatment in the research institution were excluded.
A number of 61 consecutive sarcoma patients admitted to the service during the year of 2017 were analyzed.
The variables were characterized as demographic, clinical, tumor related (histopathological and anatomical data), as well the morbidity and mortality data that occurred from the first hospital visit up to 30 days after the first surgical procedure, and systemic therapy information in the maximum period of 3 cycles.
Patients were categorized according to validated diagnostic criteria, TNM classification and histological grade (G). The treatment of sarcomas in the institution follows a standardization using clinical staging. It is possible to differentiate the treatment of sarcomas between low grade and high grade tumors. This standardization allows the therapeutics to be homogeneous and allows analyzes of high reliability.
The main endpoint was the acute morbimortality data, graded according to CTCAE version 5.0 (Common Terminology Criteria for Adverse Events) of the National Cancer Institute of the United States of America. Other objectives were the characterization of the patient's population according to the several demographics, clinical and histopathological data.
A database was constructed and from it associations were made, the sarcomas were analyzed as a whole and also separately, from associations made within each histological type. Demographic characteristics were related to staging, histological subtype, surgical complications, toxicities of radiotherapy and chemotherapy, response to treatment, cause of death and survival.
Variables were described in categories. Continuous variables were measured with values, means and standard deviation. To identify associations of the patient characteristics and the presence of adverse events we used Fisher's exact test or chi-square test.
The study included 61 patients and
| Sociodemographic characterization | Minimum - Maximum | Mean |
|---|---|---|
| Age | 17-78 | 46,56 |
| BMI | 16,7-41,9 | 26,88 |
| Sociodemographic, clinical and histopathological characterization | Number | % |
| Gender Male | 34 | 55,70% |
| Female | 27 | 44,30% |
| Race/Ethnics White | 42 | 68,90% |
| Other | 19 | 31,10% |
| Morbidities Arterial hypertension | 12 | 19,70% |
| Allergy | 5 | 8,20% |
| Others | 15 | 25% |
| No morbidities | 32 | 52,50% |
| Tumor Type Soft-tissue Tumor | 45 | 77% |
| Cavity/ retroperitoneal Tumor | 16 | 26% |
| Anatomical site of the primary lesion Head and Neck | 3 | 4,90% |
| Thorax | 6 | 9,80% |
| Abdominal Wall | 7 | 11,50% |
| Retroperitoneal | 15 | 24,60% |
| Upper extremities | 6 | 9,80% |
| Lower extremities | 24 | 39,30% |
| Metastasis to diagnosis Present | 9 | 14,70% |
| Absent | 52 | 85,30% |
| Histological subtype of sarcoma Liposarcoma | 10 | 16,40% |
| Leiomyosarcoma | 10 | 16,40% |
| Synovial sarcoma | 8 | 13,10% |
| Chondrosarcoma | 5 | 8,20% |
| Others | 28 | 46% |
| Clinical Stage I | 23 | 37,70% |
| II | 10 | 16,40% |
| III | 14 | 23,00% |
| IV | 9 | 14,80% |
| Grade Low | 10 | 16,40% |
| Intermediate | 10 | 16,40% |
| High | 18 | 29,50% |
| Characterization of the Surgical Treatment Number % | ||
|---|---|---|
| Surgical Treatment Operated | 41 | 69,50% |
| Not operated | 18 | 30,50% |
| Surgical Complication No | 29 | 70,70% |
| Yes | 12 | 29,30% |
| Type of Surgical Complication Infection | 3 | 4,90% |
| Dehiscence | 2 | 3,30% |
| Seroma | 4 | 6,60% |
| Others | 3 | 4,90% |
| Characterization of the Chemotherapy and Radiotherapy Number % | ||
|---|---|---|
| Chemotherapy Neoadjuvant | 6 | 9,80% |
| Adjuvant | 7 | 11,50% |
| Metastatic Disease | 9 | 14,80% |
| Radiotherapy No | 43 | 70,50% |
| Yes | 14 | 23,00% |
| Morbidities* No | 55 | 90,16% |
| Yes | 6 | 9,84% |
| Mortality** No | 61 | 100,00% |
| Yes | 0 | 0,00% |
Regarding the clinical data (
Histopathological data shows the most prevalent subtypes were leiomyosarcoma and liposarcoma, followed by synovial sarcoma, chondrosarcoma, dermatofibrosarcoma and Ewing's sarcoma (
The majority treatment was surgery, performed in 41 patients (67.2%). There were surgical complications in 12 patients (29.3%). Adverse events were graded according to CTCAE version 5.0. Of the twelve, only 2 (16%) had grade III complications and the remaining grade I (84%). Three showed signs of infection, the first only at the surgical site (grade I), the second at the surgical site and nearby regions (grade I), and the third presented systemic symptoms (grade III). Six of them presented grade I adverse effects, two of them due to operative wound dehiscence and four due to seroma formation. The remainder presented grade III adverse effects, respectively, as a result of the abrupt small bowel obstruction, grade I adverse effect due to small fistula in colorectal anastomosis, and grade I adverse effect resulting from pelvic collection (
The chemotherapy was performed by 22 patients (
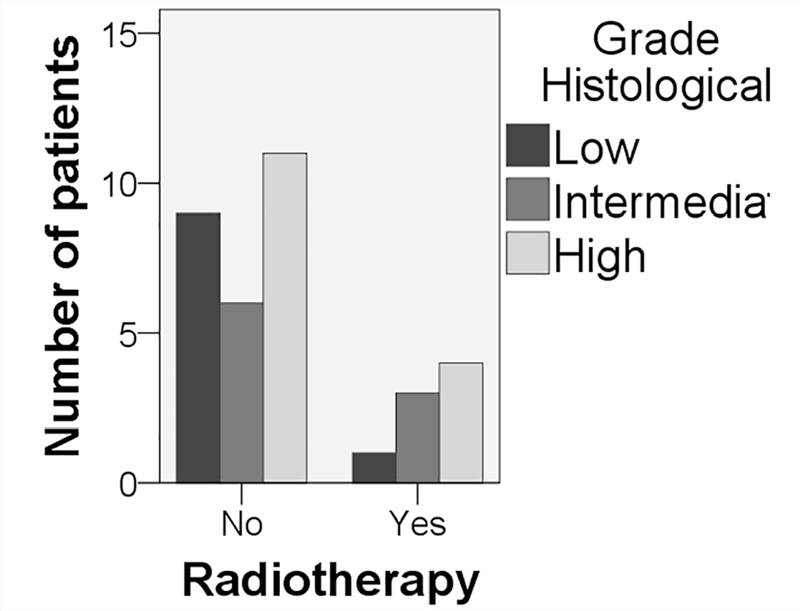
Figure 1 Relation of grade of sarcoma and indication of radiotherapy.
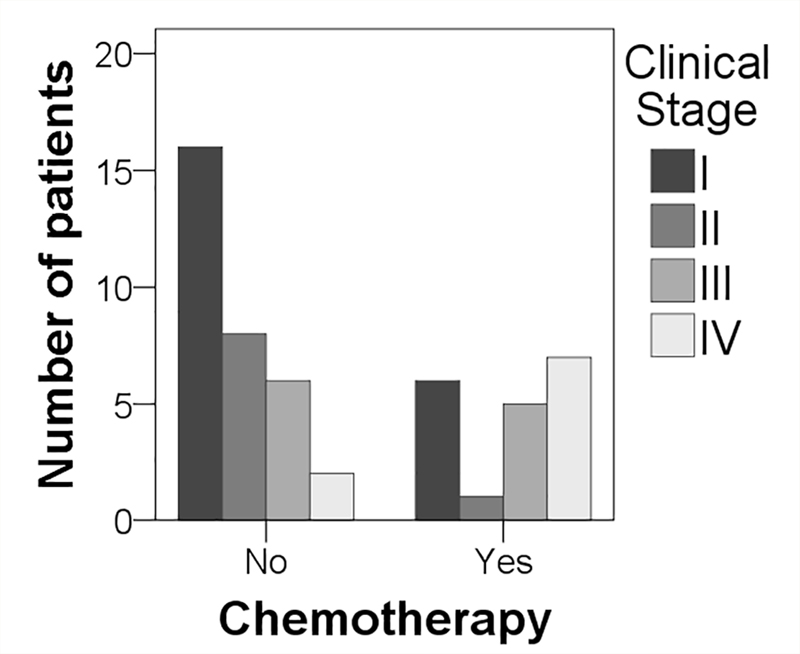
Figure 2 Indication of chemotherapy according to clinical stage.
Regarding gender, the female and male populations presented higher clinical stages I and II presentations. However, when comparing stage I and II separately from III and IV, there are 16 women in stages I and II, and 8 in stages III and IV, while there are 17 men in stages I and II, and 15 in stages III and IV. Thus, there is a prevalence of males in more advanced stages when compared to females.
Association tests were performed using BMI, histological grade, clinical stage and pretreatment morbidities according to operative complications, need for Intensive Care Units and readmissions during treatment. No association was found to any of adverse events (
| Variable | Category | Operative Complications | No Operative Complications | p value |
|---|---|---|---|---|
| Body Mass Index | Obese | 2 | 5 | 0.649 |
| Overweight | 2 | 3 | ||
| Normal Weight | 1 | 8 | ||
| Underweight | 0 | 1 | ||
| Histological Grade | Low | 2 | 6 | 0.866 |
| Intermediate | 3 | 5 | ||
| High | 4 | 4 | ||
| Clinical Stage | I | 4 | 14 | 0.144 |
| II | 3 | 5 | ||
| III | 4 | 3 | ||
| IV | 0 | 5 | ||
| Pretreatment Morbidities | Yes | 8 | 9 | 0.079 |
| No | 4 | 19 | ||
| Need for Intensive | No need for | |||
| Variable | Category | Care Units | Intensive Care Unit | p value |
| Body Mass Index | Obese | 0 | 6 | 0.125 |
| Overweight | 1 | 4 | ||
| Normal Weight | 1 | 8 | ||
| Underweight | 1 | 0 | ||
| Histological Grade | Low | 0 | 8 | 0.494 |
| Intermediate | 2 | 6 | ||
| High | 2 | 6 | ||
| Clinical Stage | I | 3 | 14 | 0.694 |
| II | 2 | 6 | ||
| III | 2 | 5 | ||
| IV | 0 | 5 | ||
| Pretreatment Morbidities | Yes | 1 | 15 | 0.056 |
| No | 8 | 15 | ||
| Variable | Category | Readmissions during treatment | No readmissions during treatment | p value |
| Body Mass Index | Obese | 0 | 7 | 0.047 |
| Overweight | 0 | 6 | ||
| Normal Weight | 2 | 10 | ||
| Underweight | 1 | 0 | ||
| Histological Grade | Low | 0 | 9 | 0.112 |
| Intermediate | 0 | 8 | ||
| High | 3 | 11 | ||
| Clinical Stage | I | 0 | 20 | 0.079 |
| II | 0 | 8 | ||
| III | 2 | 8 | ||
| IV | 2 | 7 | ||
| Pretreatment Morbidities | Yes | 3 | 20 | 1.000 |
| No | 3 | 25 |
Morbidities requiring readmission up to 30 days after starting treatment occurred with six patients (
The number of patients included, although small, when assessing the rarity of the disease and the time of inclusion in the study, is important and capable of generating useful data for analysis.
There are few studies on the characteristics of patients with sarcoma when compared to the other neoplasms. The prevalence of extremity location was also reported in studies by Siegel et al. (2014).(
Several studies have shown that the treatment of soft tissue sarcomas is usually surgical and is aimed primarily at total wide excision with free margins. From this, we can define those who benefit from adjuvant radiotherapy, since they are radiation- sensitive neoplasias. Low-grade tumors usually do not require adjuvant radiotherapy, whereas those of intermediate and high-grade tumors usually receive the complement of radiation therapy.(
Adjuvant chemotherapy is usually indicated in aggressive, high grade and metastatic tumors. The main chemotherapy drugs used in the treatment of sarcomas: Antracyclics (Doxorubicin and Epirubicin), Ifosfamide, Gemcitabine and Dacarbazine.(
A retrospective cohort study at the MD Anderson Cancer Center, showed that postoperative complications occurred more frequently after concomitant organ resection, and more patients had hospital admissions for at least 14 days after concomitant resection of organs. The complications observed were pneumonia and respiratory insufficiency, cardiac arrhythmia, intra-abdominal abscess, anastomosis leakage, renal artery thrombosis, wound infection requiring intervention and chylous ascites requiring drainage. It was also observed that concomitant organ resection was associated with an increased risk of postoperative complications in the univariate analysis, which remained significant after adjustment with other variables in the multivariate analysis.(
Our study did not separately evaluate the surgeries in which there was concomitant organ resection, however, we evaluated the most frequent postoperative complications. The main ones were associated with minor surgical wound complications such as seroma formation and local infection. Few complications (2 in 41 patients - 4.9%) required greater intervention, but there were no complications with imminent risk of death or related deaths.
Despite the small number of patients, it is possible to infer that the number of complications associated to the surgical treatment was high, with 12 of the 41 patients (29.3%). Morbidities requiring readmission up to 30 days after initiation of treatment were observed in 6 patients (9.84%), a significant value when we assessed the causes and concluded that the majority is related to treatment or disease, such as vascular access events, reaction to chemotherapy, febrile neutropenia. The occurrence of death up to 30 postoperative days or to 3 cycles of systemic therapy was not observed. Mortality up to 30 days was also evaluated in the Ikoma et al. (2018) cohort study, and it was also not observed.(
Although comorbidities are known complication factors of cancer therapies, we could not associate them in our study. A relevant criticism is the small number of patients included.
The bias of real data analysis in retrospective collection is always a risk that should be considered; however, the present research has obtained convergence of the results found with the literature. Another important aspect was that, although retrospective, this study was collected prospectively throughout the year 2017 and 2018, with the information collected shortly after it was obtained, with the possibility of elucidating information with the caregiver team.
The characterization of patients with soft tissue sarcomas was similar to that described in the literature. The morbidity associated with the treatment of sarcomas was high, but not very serious. Mortality was absent. Pre-therapy morbidities were not related to therapeutic complications.
This study generated relevant information about the clinical characterization and the treatment performed. It is important for the institutions that work with sarcomas in Brazil, because it evaluates patients' characteristics in a real scenario, making it possible to create realistic treatment strategies, also generating precious data for future research.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.