Typically used as an antidiabetic drug, metformin has been evaluated for the last few decades as a possible molecule capable of preventing cancer. The first data concerning a possible protective role of antidiabetic drugs in preventing carcinogenesis were published in 1978.
While the exact antineoplastic mechanisms induced by metformin are unknown, decreased stimulation of insulin growth factor (IGF) receptor present in tumor cells through a reduction in serum insulinemia
More recently pre-clinical studies have demonstrated that metformin has also direct cytotoxic effects on cancer stem cells by interfering with their glycolysis and energy production pathways.
Despite a biological rational for metformin effect, there are conflicting evidences to support the use of metformin as a primary or secondary cancer prophylaxis. In our last review, 2 years ago,
We performed an update search from the systematic review published in 2014 of clinical studies that evaluated the role of metformin in cancer, specifically with the focus of articles about cancer prevention of solid tumors. Eligible studies were fully reported prospective or retrospective cohorts, case-control or population-based-studies that have evaluated metformin alone or combined with other agents for primary or secondary cancer prevention. Studies that evaluated pre-malignant lesions were also included. We exclude case reports, pediatric studies or studies of lymphoproliferative diseases.
The search for articles was conducted through PubMed. We used the medical subject headings (MeSH descriptors) “ neoplasms ”, “ cancer ” and “ metformin ”, limiting the search to “ humans ”, from March 1st 2014 (data from the last review) until May 16 2017 and to the English language. Two independent investigators (MN, MCLAS) performed the search and collected information on tumor type, clinical setting, study design, number and characteristics of study populations, and clinical outcomes.
Given the large number of studies retrieved, we divided our results according to the following sites of cancer: general (articles that analyzed cancer incidence despite of primary site), breast, gynecological, colorectal, hepatocellular, lung, head and neck, prostate and miscellaneous cancer (primary sites of cancer described specifically in a few articles).
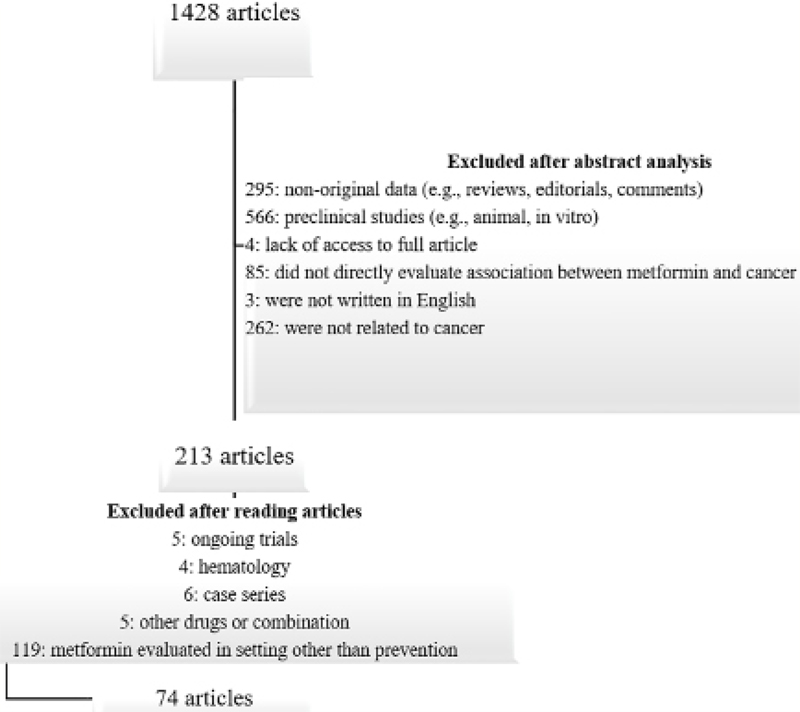
From March 2014 to May 16 2017, 1,428 potentially eligible articles were identified. After excluding 295 non-original data (e.g., reviews, editorials, comments), 566 preclinical studies (e.g., animal, in vitro), four incomplete studies, 85 studies which did not directly evaluate association between metformin and cancer, 3 studies not written in English (Danish, Polish and Chinese), 262 studies not related to cancer and four studies without access to full text, we finally selected 213 articles. Out of these 213 articles, we excluded five ongoing trials, four studies about hematological disease, six small case series (with less than 10 patients) and five articles with other antidiabetic drugs or drug combination. Finally, we had selected 193 articles, of which 74 analyzed the role of metformin in cancer prevention (
Figure 1 Selection of articles
Since our last review,
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Kong et al, 2014 (17) | Prospective cohort •3,303 type II diabetic patients, using metformin •5,062 type II diabetic patients, using other drugs | Association between metformin use and incidence of cancer in diabetic patients | Treatment with metformin (HR =0.39; 95% confidence interval: 0.25 - 0.61; p <0.001) reduced any cancer incidence. |
| Tsilidis et al, 2014 (11) | Retrospective cohort •51,484 type II diabetic patients, who first started using metformin •18,264 type II diabetic patients, who first started using sulfonylurea •26,072 type II diabetic patients, who started using other drugs or drug combination | Association between metformin use and cancer incidence in diabetic patients | Compared with sulfonylurea users, metformin users had no difference in total cancer incidence (HR= 0.96; 95% CI 0.89-1.04). Colorectal (HR= 0.92; 95% CI 0.76-1.13), prostate (HR 1.02; 95% CI 0.83-1.25), lung (HR= 0.85; 95% CI 0.68-1.07), and postmenopausal breast (HR= 1.03; 95% CI 0.82-1.31) cancer incidences were also similar. |
| But et al, 2014 (13) | Retrospective cohort •1,188 metformin users •113 metformin non-users •22,093 no anti-diabetic use | Incidence of cancer between patients using metformin, other drugs or no anti-diabetic medication | There were no significant difference in caner incidence between users and non-users of metformin (HR 1.03; CI 0.72-1.34). |
| Kowall et al, 2015 (12) | Retrospective cohort •15,786 type II diabetic patients, who used metformin •67,70 type II diabetic patients, who used other drugs | Difference between other anti-diabetic drugs and metformin in the incidence of cancer in diabetic patients | In multivariable adjusted models, HR were 1.09 (95% CI 0.87-1.36) for sulfonylurea, 1.14 (95% CI 0.85-1.55) for insulin, and 0.94 (95% CI 0.67-1.33) for other anti-diabetes drugs, when compared with metformin use. |
| Jones et al, 2015 (14) | Observational follow up after a randomized study •2,220 type II diabetic patients taking rosiglitazone •2,227 type II diabetic patients taking metformin/sulfonylurea | Incidence of cancer in diabetic patients using rosiglitazone, compared with those using metformin/ sulfonylurea | There were no significant difference in relative risk (and 95 % CI) for different cancers diagnosis (bladder, breast, colorectal, liver, prostate and melanoma), except for pancreatic cancer (HR= 0.31; 0.11-0.85). |
| Lin et al, 2015 (18) | Retrospective cohort •145,080 non-diabetic patients •34,823 type II diabetic patients divided into metformin users or non-users | Association between diabetes and metformin use with cancer incidence | Metformin users had a decreased incidence of lung (AHR 0.62; 0.45- 0.85, p< 0.05) and liver (AHR 0.64; 0.49-0.83, p< 0.05) cancer, and marginally of colorectal cancer (AHR 0.74; 0.53-1.03, p = 0.075). |
| Valent F, 2015 (19) | Retrospective cohort •75,1678 non-diabetic patients •63,119 diabetic patients using metformin •52,869 diabetic patients using other drug | Association between diabetes mellitus status and metformin use with cancer incidence | Metformin users had a modest reduced incidence of gastrointestinal cancer (HR =0.993; 0.992-0.994) in diabetic patients, except for the small intestine, the rectum, and the gallbladder cancers, where no association was found. |
| Chen et al, 2015 (20) | Retrospective cohort •2,223 type II diabetic patients using metformin •3,965 type II diabetic patients using sulfonylurea •1,137 type II diabetic patients using other drugs | Incidence of cancer between patients using metformin or other anti-diabetic medication | Adjusted HR of cancer was 1.36 in the sulfonylurea group (95% CI 1.11-1.67, p=0.003), when compared with metformin group. There were no significant differences between metformin and other anti-diabetic medications than sulfonylurea. |
| Gong et al, 2016 (21) | Prospective cohort •137,342 non-diabetic women •1,100 type II diabetic women using metformin •7,384 type II diabetic women metformin non-users | Association between diabetes mellitus status and metformin use with cancer incidence and mortality | When compared with non-diabetic women, metformin users had similar cancer incidence (HR= 1.13; 95% CI 1.04-1.23), while women using other anti-diabetic drugs had higher cancer incidence (HR 1.10; 95% CI 1.00-1.21; p = 0.66). |
| Holden et al, 2016 (15) | Retrospective cohort •5,536 type II diabetic patients using insulin and metformin •6,484 type II diabetic patients using insulin monotherapy | Incidence of cancer between patients using combination of insulin and metformin or insulin monotherapy | There were no statistical difference in cancer incidence between diabetic patients treated with insulin plus metformin, when comparing with insulin monotherapy (AHR 0.96, CI 0.80-1.15). |
| Hicks et al, 2017 (16) | Prospective cohort •108,258 type II diabetic patients newly-prescribed metformin •29,496 type II diabetic patients newly-prescribed other drugs | Incidence of viral associated cancer in patients with type 2 diabetes using metformin | Metformin was not associated with a decreased rate of viral associated cancer (HR 0.92, 95% CI 0.65-1.32), regardless of the duration of metformin use or the viral etiology. |
HR, hazard ratio; AHR, adjusted hazard ratio; CI, confidence interval
Five studies reported no association between metformin use and cancer risk
In a large prospective cohort named World Health Initiative,
Cancer-specific mortality was similar between diabetics using metformin and non-diabetics, but it was higher among diabetics taking other antidiabetic agents (p=0.007). The other two large studies revealed a possible role of metformin in cancer primary prevention for lung [Adjusted Hazard Ratio (AHR) 0.62 (0.45-0.85), p<0.05], liver [AHR 0.64 (0.49-0.83)]
Until 2014, in our first review, data about the role of metformin as a prevention for colorectal cancer (CRC) was based on retrospectives studies, a meta- analysis (with non-randomized studies) and a randomized trial composed by 26 patients, which analyzed a secondary prophylaxis for aberrant crypt foci.
Four of the retrospective cohorts were performed in diabetic patients who underwent screening colonoscopy, analyzing the difference in the incidence of pre-malignant lesions according to metformin use. Three of the studies showed that metformin use was associated with a lower incidence of colorectal adenomas or advanced adenomas.
These results were confirmed by a double-blind placebo-controlled multicenter study conducted in Japan that randomized 151 non-diabetic patients with previous history of colorectal polypectomy, to investigate the role of metformin as a secondary prophylaxis.
Another retrospective cohort performed in Taiwanese patients with type II diabetes compared the risk of colorectal cancer between ever-users and never- users of metformin. The results showed that metformin ever-users had a significantly lower risk of colorectal cancer (HR 0.5; 95% CI 0.45-0.56). The effect of the cumulative duration of metformin therapy was also evaluated and the HR (95% CI) for the first (<27.1 months), second (27.1-58.1 months) and third tertile (>58.1 months) was 0.86 (CI 0.76-0.98), 0.51 (CI 0.45-0.59), 0.26 (CI 0.23-0.30).
In one of the case-control studies, metformin use was also associated with a decreased colorectal cancer risk, while in the other case-control study this reduction was observed only among women.
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Cho et al, 2014 ( | Retrospective cohort • 912 type II diabetics with metformin use • 2193 type II diabetics without metformin use | Association between long-term metformin use and polyp/adenoma incidence | Metformin group had lower colorectal lesions than non-metformin group [(39.4% vs. 62.4%, P<0.01) and (15.2% vs. 20.5%, P<0.01)]. |
| Cardel et al, 2014 ( | Case-control • Cases: 2,088 type II diabetics with a primary colorectal cancer, metformin users • Controls: 9,060 sampled among subjects with type II diabetes, not using metformin | Association between long-term metformin use and CRC incidence | There were no association between metformin use and CRC incidence [0.83 (95% CI 0.68-1.00)]. It was suggested a possible protective effect for women (Odds Ratio 0.66 vs. 0.99 for men). |
| Onitilo et al, 2014 ( | Retrospective cohort • 2,882 type II diabetic patients, using insulin • 5,679 type II diabetic patients, using metformin • 886 type II diabetic patients, using sulfonylurea • 3,113 type II diabetic patients, using any of the above | Association between glycemic control and glucose-lowering medication use and incidence of breast, prostate or colon cancer | Metformin use was associated with reduced risk of breast [HR= 0.65 (0.45 - 0.94)] and prostate [HR= 0.71 (0.52 - 0.98)] cancer. There was no significant association between metformin and colon cancer incidence. |
| Kim et al, 2015 ( | Retrospective cohort • 151 type II diabetics with metformin use • 89 type II diabetics without metformin use | Association between long-term metformin use and adenoma/advanced adenoma incidence | Metformin group had lower advanced adenoma incidence compared with the non-metformin group (relative risk [RR], 0.09; p=0.011), although rate of total colorectal adenoma was similar between groups. |
| Higurashi et al, 2016 ( | Phase III trial • 79 assigned to the metformin group • 72 to the placebo group | Metformin as a second prophylaxis of colorectal polyp/adenoma in non-diabetic patients | Colorectal polyps (RR= 0.67; 95% CI 0.47-0.97) and adenomas (RR= 0.60; 95% CI 0.39-0.92) were less frequent in the metformin group than in the placebo group. |
| Jain et al, 2016 ( | Retrospective cohort • 88 type II diabetic patients, using insulin only • 211 type II diabetic patients, using metformin only • 40 type II diabetic patients, using combination of insulin and metformin | Effect of combination treatment with insulin and metformin on colon adenoma and advanced adenoma | There was no statistically significant association between insulin and metformin use and adenoma or advanced adenoma detection rates. |
| Rosato et al, 2017 ( | Case-Control • 1,147 colorectal cancer cases • 1,594 controls | Association between type II diabetes, antidiabetic medications, and the risk of colorectal cancer. | Metformin use was associated with a decreased colorectal cancer risk (OR 0.47; 95% CI 0.24-0.92). The association was stronger for > 10 years of use of metformin (OR 0.36). Insulin, otherwise, was associated with an increased colorectal cancer risk (OR 2.20; 95% CI 1.12-4.33). |
| Tseng, 2017 ( | Retrospective cohort •153,270 type II diabetic patients, ever-users of metformin •16,331 type II diabetic patients, never-users of metformin | Association between colorectal cancer and use of metformin in type II diabetic patients | Metformin users had a lower risk of colorectal cancer (HR 0.5; 95% CI 0.45-0.56). The HR for the first, second and third tertile of cumulative duration of metformin therapy was 0.86 (95% CI 0.76-0.98), 0.51 (95% CI 0.45-0.59), 0.26 (95% CI 0.23-0.30). |
| Han et al, 2017 ( | Retrospective cohort •106 type II diabetic patients, with metformin use •151 type II diabetic patients,, without metformin use | Effect of metformin on recurrence of colorectal adenoma in diabetic patients with previous colorectal adenoma | Metformin use was associated with lower colorectal adenoma recurrence (HR 0.57; 95% CI 0.38-0.85). |
Until 2014, two meta-analysis had shown lower risk of developing liver cancer in diabetic patients taking metformin
The prospective study was performed in a Taiwanese nationwide database population of diabetic and hepatitis-B-infected patients to analyze the incidence of hepatocellular cancer (HCC) or non-liver cancers. The metformin users did not experience reduction in incidence of liver cancer in comparisons with nonusers but the incidence of general cancer was lower among metformin users.
The nested-case control studies were performed in large population databases. Diabetic individuals who developed HCC during follow-up were selected as cases and matched (according to time of metformin use, dosage, age and diabetes diagnostic time) to individuals in the same cohort who did not have HCC. The results were ambiguous. Numerically, the odds ratio favored the use of metformin as a protective factor for the onset of HCC; however, in two of them we find no statistical significance
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Hagberg et al, 2014 ( | Case-control • Cases: 305 HCC and diabetics, metformin users • Controls: 1,151 diabetics matched for demographic and clinical data | Association between metformin use and HCC incidence | No association between liver cancer and metformin-only use (OR=0.74 (95% CI=0.45-1.20). No other association was found with other antidiabetic drugs and HCC incidence. |
| Chen et al, 2015 ( | Prospective cohort • 71,847 Taiwanese patients with a recorded diagnosis of Hepatitis B Virus (HBV) infection 4,774 - Metformin-only 8,861 - Statin-only 5,121 - Statin + Metformin 53,037 - no medication users | Incidence of liver cancer and other cancer in metformin users, statin users and combination users, in Hepatitis B patients. | Patients taking only metformin had risk- adjusted HRs of 0.82 (95% CI, 0.75-0.90) for all cancers, 0.97 (95% CI, 0.84-1.14) for liver cancer, and 0.75 (95% CI, 0.67-0.84) for non-liver cancers. The statin only-use and the association use revealed significance in its protective role regarding all cancers, liver cancer and non-liver cancers. |
| Bosetti et al, 2015 ( | • Case-control Cases: 190 diabetics with HCC diagnosis during follow up Control: 3,772 diabetic subjects matched to each case | Incidence of HCC during follow-up | Reduced risk of HCC with metformin use (OR = 0.57, 95%CI 0.41-0.79). |
| Chen et al, 2015 ( | • Case-control Cases: 340 patients recently diagnosed with diabetes and metformin users Controls: 1,360 patients diabetic patients matched at a 4:1 ratio | Incidence of HCC in a population recently diagnosed with type II diabetes | Metformin combinations with sinvastatin, atorvastatin, or rosuvastatin decreased HCC incidence (OR = 0.30, 0.30, and 0.24; 95% CI = 0.15-0.59, 0.16-0.54, and 0.08-0.70, respectively). |
HR, hazard ratio; OR, odds ratio; CI, confidence interval.
Results presented in 2014 about metformin and breast cancer incidence were provided by observational data with conflicting results and a meta-analysis of retrospective studies suggesting a possible benefit of metformin as a chemoprophylaxis for breast cancer. We found seven new studies in this setting: one prospective cohort, five retrospective and one case control study.
A universal system of National Health Research Institutes was implemented in Taiwan, which allowed a big data collection of diabetic woman, to analyze the incidence of breast cancer between metformin users and nonusers.
The prospective cohort evaluated women aged 65 years or older enrolled in Medicare in the United States who initiated monotherapy with metformin or sulfonylureas. No significant difference was seen in the risk of breast cancer between the two groups.
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Tseng CH, 2014 ( | Retrospective cohort • 19,1195 type II diabetic patients, using metformin • 28,5087 type II diabetic patients, metformin never-users | Association between long-term metformin use and incidence of breast cancer in diabetic patients | Metformin use, was associated with low breast cancer incidence (HR 0.630; CI 0.597-0.665); p<0.0001. |
| Besic et al, 2014 ( | Retrospective cohort • 128 type I/II diabetic patients, using metformin • 125 type I/II diabetic patients, not using metformin • 320 non-diabetic patients | Association between long-term metformin use, diabetes and molecular subtype of breast cancer | Diabetic diagnosis and metformin use were associated with different molecular subtypes of breast cancer (p = 0.01). Metformin users had a biggest proportion of luminal A and a smaller proportion of triple negative breast cancer. Compared to metformin non-users, metformin users had a smaller T stage (p = 0.03). |
| Tseng CH, 2015 ( | Retrospective cohort Type II diabetic patients insulin users (59,798): • 53,420 metformin users • 6,378 metformin non-users • Type II diabetic patients insulin never-users (422,235): • 259,203 metformin users • 163,032 metformin non-users | Impact of metformin use in breast cancer incidence between insulin users and non-users diabetic patients | The use of insulin without other antidiabetic drug was associated with breast cancer risk (HR 1.413, CI 1.030-1.940). Metformin showed a protective role for breast cancer among patients using insulin (HR 0.798, 95 % CI 0.741-0.859). |
| García- Esquinas et al, 2015 ( | Case-control study Type II diabetic postmenopausal woman, using or not metformin: • 1,018 breast cancer patients • 1,243 matched controls | Association between long-term metformin use and incidence of breast cancer among diabetic patients | Diabetes was not linked to increased breast cancer incidence (OR 1.09; 95 % CI 0.82-1.45), although it increased the risk of developing triple negative tumors (OR 2.25; 95 % CI 1.22-4.15). Among diabetics, the incidence of Hormone Receptor positive/HER2 negative tumors was associated with duration of metformin treatment (OR per year 0.89; 95 % CI 0.81-0.99). |
| Calip et al, 2016 ( | Retrospective cohort • 5,700 type II diabetic patients, using metformin • 4,350 type II diabetic patients, not using metformin | Association between different medication use and breast cancer incidence in diabetic patients | Metformin use did not influence breast cancer incidence (HR 0.86; 95% CI 0.65-1.12), except for those treated during 1-2.9 years (HR 0.39; 95% CI 0.19-0.80) versus nonusers. |
| Hong et al, 2017 ( | Prospective cohort • 45,900 women aged 65+ who initiated monotherapy with metformin • 13,904 women aged 65+ who initiated monotherapy with sulfonylureas | Relative risk of breast cancer for older women initiating metformin versus sulfonylureas | The risk of breast cancer did not differ between metformin initiators and sulfonylurea initiators (HR 1.2; 95% CI 0.94-1.6). |
| Lega et al, 2017 ( | Retrospective cohort • 1,519 women with diabetes and breast cancer, exposed to metformin • 1,606 women with diabetes and breast cancer, not exposed to metformin | Association between metformin and breast cancer stage at diagnosis | There was no association between metformin use and an earlier stage of breast cancer (OR 0.98; 95% CI 0.81-1.19). |
There were two studies about metformin and prevention of gynecological cancer in our first review in 2014. They were both retrospective and did not find difference in endometrial and ovarian cancer incidence with metformin use.
Diabetic patients ineligible from Women's Health Initiative (WHI) were included in an observational study, divided into three groups based on the type of drugs utilized at the time of study entry. This observational cohort showed an elevated risk of endometrial cancer according to diabetic duration (HR=1.31, 95% CI 1.08-1.59) even after adjusting for body mass index (BMI). There was no significant association between metformin use and endometrial cancer incidence.
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Luo et al, 2014 ( | Prospective cohort • 83,860 non-diabetic women • 529 type II diabetic patients, using metformin alone • 3,718 type II diabetic patients, metformin never-users | Association between diabetes and long-term metformin use with endometrial cancer incidence | There were no differences in endometrial cancer risk between metformin users and non-users (HR 1.00, CI 0.62-1.62). |
| Tseng CH, 2015 ( | Retrospective cohort • 193,369 type II diabetic patients, using metformin • 286,106 type II diabetic patients, metformin never-users | Association between long-term metformin use and incidence of ovarian cancer in diabetic patients | The risk of ovarian cancer was reduced between patients using metformin (HR 0.546, CI 0.474-0.628). |
| Ko et al, 2015 ( | Retrospective cohort • 456,838 type II diabetic patients, new users of metformin • 84,290 type II diabetic patients, new users of sulfonylureas | Association between metformin use and incidence of endometrial cancer in diabetic patients | Metformin use was not associated with a reduced endometrial cancer incidence (HR 1.09, CI 0.88-1.35). |
| Soffer et al, 2015 ( | Retrospective cohort • 4,887 type II diabetic patients, using only metformin • 22,037 type II diabetic patients, using a combination including metformin • 14,865 type II diabetic patients, not using metformin • 24,989 type II diabetic patients, not using any anti-diabetic drug | Association between long-term metformin use and incidence of breast, endometrial or ovarian cancer | There were no significant differences between metformin users and non-users in breast cancer or all cancers combined risk. |
| Tseng CH, 2015 ( | Retrospective cohort • 193,005 type II diabetic patients, metformin ever-users • 285,916 type II diabetic patients, metformin never- users | Association between metformin use and endometrial cancer incidence in diabetic patients | Metformin users showed a reduced risk of endometrial cancer when compared to metformin non-users (HR 0.675, CI 0.614-0.742). |
| Tseng et al, 2016 ( | Retrospective Cohort • 132,971 type II diabetic patients, metformin ever-users • 6,940 type II diabetic patients, metformin never-users | Effect of metformin use in the risk of cervical cancer. | Metformin users had a significantly lower risk of cervical cancer (HR 0.55; 95% CI 0.40-0.77). The results were supported by analysis in a matched cohort. |
| Franchi et al, 2017 ( | Nested Case-Control • 376 diabetic women with endometrial cancer • 7,485 diabetic matched controls | Association between endometrial cancer and the use of metformin and other antidiabetic drugs. | There was no significant association between endometrial cancer and use of metformin (OR 0.99; 95% CI 0.80-1.23), sulfonylureas (OR 1.14; 95% CI 0.91-1.42), insulin (OR 0.72; 95% CI 0.34-1.56), and other antidiabetic drugs (OR 1.21; 95% CI 0.75-1.95). |
| Kwon et al, 2017 ( | Nested Case-Control • 492 women with endometrial cancer and antidiabetic drug use • 4404 controls | Association between type of diabetic pharmacotherapy and endometrial cancer risk. | There was no difference in endometrial cancer risk between those using metformin and those using other classes of medications (OR 1.5; 95% CI 0.9-2.4). |
HR, hazard ratio; OR, odds ratio; CI, confidence interval
Back in 2014 we found several studies suggesting reduced risk of prostate cancer (PCa) with metformin.
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Tseng CH, 2014 ( | • Retrospective Cohort 209,269 men with new onset type 2 diabetes and never-metformin users (9,642 had prostate cancer) 186,212 men with new onset type 2 diabetes and ever-metformin users (2,776 had prostate cancer) | Incidence of prostate cancer on a time-dependent manner regarding metformin exposure | The incidences of prostate cancer were 737,10 and 239,42 per 100,000 person- years among never-users and ever-users, respectively. The adjusted HR for ever- versus never-users was 0.476 (95% CI, 0.454-0.499; p<0,001). The incidence of prostate cancer decreased with longer duration of metformin use (> 21,5 months). |
| Bensimon et al, 2014 ( | • Nested Case-Control 935 metformin users men with prostate cancer and history of type II diabetes Cases: 112 prostate cancer deaths Controls: 268 controls | Evaluate the association between prostate cancer mortality and all-cause mortality, and metformin exposure, either by post-diagnostic, as well as duration and dose-response metformin use. | Post-diagnostic metformin use was not associated with a decreased risk of cancer-specific mortality (RR, 1.09; 95% CI, 0.51-2.33), and also not associated with all-cause mortality (RR, 0.79; 95% CI, 0.50-1.23). Secondary analysis revealed that a cumulative duration >938 days of metformin use was associated with an increased mortality risk (RR, 3.20; 95% CI, 1.00-10.24). |
| Danzig et al, 2015 ( | • Retrospective Cohort 767 diabetic men undergoing radical prostatectomy for prostate cancer. 76 patients statins-only users 56 patients metformin- only users 42 patients dual users | Interaction between statin and metformin use in biochemical recurrence (BCR) | Neither statin nor metformin use alone was significantly associated with BCR-free survival. The dual use had significantly lower BCR risk (HR=0.2; P=0,037) in multivariate analysis. |
| Nordstrom et al, 2015 ( | • Retrospective Cohort 185,667 men having a first recorded PSA test 18,574 men having a first prostate biopsy | Association between prescribed medications, prostate specific antigen (PSA) levels and the risk of either any prostate cancer or high-grade disease | Men on medication (at least 75mg/ dose aspirin, statin, insulin and metformin) had 14% lower PSA levels when compared with men who were not on medication (95% CI: -17 to -12). There were no significant associations between antidiabetic medication and the risk of prostate cancer. |
| Randazzo et al, 2015 ( | Prospective Cohort • 4,314 men were followed up and information on exposure to metformin. PSA levels and prostate cancer diagnosis were collected. Metformin users = 150 patients | Incidence of prostate cancer in this population-based PSA- screening trial according to metformin use | No significant differences in prostate cancer incidence were observed: 7.3 % metformin users vs. 8.7 % non users (p = 0.5). PSA levels and tumor grade did not differ between groups. |
| Merrick et al, 2015 ( | • Prospective Cohort 1,034 patients who underwent transperineal biopsy because of either an elevated PSA or a prior biopsy finding of atypical small acinar proliferation/ prostatic intraepithelial neoplasia 881 nondiabetic patients 65 diabetic metformin- user patients 88 diabetic non metformin-user patients | Incidence of prostate cancer in the three groups | - There was no difference in between the 3 cohorts, regarding: Prostate cancer diagnosis (Non diabetic patients 56%; diabetic metformin-user patients 67.7%; diabetic non metformin-user patients 53.4% [p=0.153]) Gleason score (Non diabetic patients 41.2%; diabetic metformin-user patients 38.6%; diabetic non metformin-user patients 40.4% [p=0.960]) Number of positive biopsy cores (Non diabetic patients 38.1%; diabetic metformin-user patients 31.8%; diabetic non metformin-user patients 38.3% [p=0.764]) Risk group stratification (Non diabetic patients 13.6%; diabetic metformin-user patients 18.2%; diabetic non metformin- user patients 17% [p=0.877]). |
| Murtola et al, 2015 ( | • Retrospective Cohort Two Cohorts 3,241 men from Finnish Prostate Cancer (PCa) Screening Trial (801 new cases of prostate cancer found) Hospital cohort identified 1,983 new cases of prostate cancer (outside screening programs) | - Association between the presence of SNP's of genes involved in energy metabolic pathways and PCa risk and prognosis. Association between antidiabetic drug use and PCa risk and prognosis and the presence of SNP's. | - Thirty SNP's were associated with PCa risk (HR = 1.57, 95% CI 1.37-1.81; p<0,001) and ten SNP's associated with survival (HR = 1.51, 95% CI 1.15-1.98; p<0,001). The antidiabetic drugs (metformin or non-metformin) did not modify the association between genetic risk score and overall PCa risk. It also did not change the risk of high-grade disease. Genetic risk score was not a significant risk predictor in patients who had used antidiabetic drugs |
| Feng et al, 2015 ( | • Retrospective Cohort 205 patients with no anti-diabetic medications 141 patients, with use of any anti-diabetic medication other than metformin 194 patients, using metformin, with or without other anti-diabetic medications | Association between the use of metformin or other anti-diabetic medications and overall, low- and high-grade prostate cancer risk. | There was no association between metformin use and total (OR=1.19; p = 0,50), low- (OR=1.01; p = 0,96), or high-grade (OR=1.83; p = 0,19) prostate cancer. |
| Wang et al, 2016 ( | Retrospective Cohort 76,733 patients 59,906 Non-Hispanic White 4,234 Hispanics 12,593 African Americans 3,983 prostate cancer (PCa) diagnosis | - Racial/Ethnic disparity in incidence of PCa in type 2 diabetic men, non-metformin users. If the impact of metformin on reducing PCa incidence correlates with the race/ethnic groups disparity PCa incidence | The use of metformin alone or combined with statins was associated with a greater PCa incidence reduction in Hispanics (HR=0.62, 95% CI=0.49-0.80; p<0,01) compared to Non-Hispanic White (HR=0.91, 95% CI=0.81,1.02; p=0,11). A 31% reduction; p< 0,01. No other relation was found. |
| Jayalath et al, 2016 ( | Cross-Sectional Study • 326 prostate cancer-free men with type 2 diabetes | Association between metformin dose and prostate-specific antigen levels. | There was an 8% decrease in PSA per 500-mg/d increase in metformin (95% CI -13 to - 2%, p = 0.011). |
| Raval et al, 2016 ( | • Retrospective cohort 948 diabetic men with incident prostate cancer, metformin users 1,704 diabetic men with incident prostate cancer, non-metformin users | Association between metformin use and cancer stage at diagnosis among diabetic men with incident prostate cancer. | Metformin users had lower risk of advanced prostate cancer in comparison with nonusers (AOR 0.68; 95% CI 0.48-0.97). |
| Chen et al, 2017 ( | • Retrospective cohort 40,273 Non-Chinese diabetic patients, with no metformin exposure 32,971 Non-Chinese diabetic patients, with metformin exposure 3,899 Chinese diabetic patients, with no metformin exposure 2,858 Chinese diabetic patients, with metformin exposure | Impact of metformin exposure on prostate cancer risk in Asian and non-Asian man | There was no association between metformin use and prostate cancer among Chinese men. Among non-Chinese men, a decreased risk of prostate cancer was seen with metformin use only among men aged 50-59 (aHR 0.86, 95% CI 0.74-1.00). |
| Haring et al, 2017 ( | • Prospective cohort 78,615 men attending the Finnish Randomized Stud of Screening for Prostate Cancer 63,037 men without antidiabetic drugs use 15,578 men with antidiabetic drugs use | Effect of metformin and other antidiabetic drugs in prostate cancer incidence | Antidiabetic drugs were associated with a lower prostate cancer risk (HR 0.85; 95% CI 0.79-0.92). Metformin decreased overall prostate cancer risk in a dose-dependent manner (HR 0.81; 95% CI 0.69-0.95). |
HR, hazard ratio; RR, relative risk; OR, odds ratio; CI, confidence interval
The retrospective studies were mostly from large population databases.
A large Finnish prospective cohort also showed antidiabetic drugs decreased prostate cancer risk (HR 0.85; 95% CI 0.79-0.92), and metformin use was associated with a lower prostate cancer risk in a dose-dependent manner (HR 0.81; 95% CI 0.69-0.95).
Other retrospective studies found that the use of metformin, often combined with statins and other antidiabetic drugs, significantly decreased prostatic specific antigen (PSA) levels and prolonged biochemical free recurrence intervals.
In our last review, the studies failed to demonstrate any chemopreventive effect of metformin in lung cancer.
The third retrospective study did not find association between metformin use and lung cancer (HR 1.02; 95% CI 0.85-1.22).
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results | |||
|---|---|---|---|---|---|---|
| Tsai et al, 2014 ( | • Retrospective Cohort 47,356 Chinese diabetics Non metformin users - 28,282 Metformin users - 19.074 | Evaluate the incidence of lung cancer in a diabetic patients according to metformin use | The utilization of metformin was an independent protective factor, and the risk of developing lung cancer decreased progressively with either the higher cumulative dose (HR=0.26, 95% CI=0.15-0.43; p<0,001 - for over 1,095g of cumulative defined daily dose (DDD)) or the higher intensity of metformin use (HR=0.36, 95% CI=0.23-0.56; p<0,001 - for over 20 DDD/month intensity dose of metformin). | |||
| Sakoda et al, 2015 ( | • Retrospective Cohort 257,542.42 person-years, metformin never-users 171,015.06 person-years metformin users. | Incidence of lung cancer in patients with diabetes, using or not using metformin | No association was found between use or non-use of metformin regarding lung cancer risk (HR 1.02; 95% CI 0.85-1.22). | |||
| Tseng et al, 2017 ( | • Retrospective Cohort 280,159 type II diabetic patients, metformin ever-users 15,414 type II diabetic patients, metformin never-users | Association between lung cancer and metformin use in type II diabetic patients | Metformin ever-users had a significantly lower risk of lung cancer in the original sample (HR 0.58; 95% CI 0.50-0.67) and in a matched sample (HR 0.71; 95% CI 0.58-0.88). | |||
We could not find studies on metformin use and head and neck cancer prevention in our last review.
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Becker et al, 2014 ( | Retrospective Case-Control Study • 2,874 cases of Head and Neck cancer • 17,244 matched controls | Incidence of Head and Neck cancer (HNC) in diabetic patients using metformin | Use of metformin was not associated with altered risk of HNC, independently of the time of use of metformin (1-29 prescriptions: adjusted OR = 0.87, 95% CI 0.61-1.24 and > 30 prescriptions adjusted OR= 0.80, 95% CI 0.53-1.22). |
| Sandulache et al, 2014 ( | Retrospective Cohort • 205 patients with Laryngeal Squamous Cell Carcinoma (SCC) • 43 individuals with diabetes diagnosis (21% of 205 individuals) | Association between metformin use and pathologic and clinical outcomes. | Patients using metformin presented with more early-stage tumors (T1 and T2) and less regional metastasis (N0; 81% metformin users vs 50% metformin non-users). At end of study, 76% of patients taking metformin were alive, compared to 41% for diabetics not on metformin and 51% for non-diabetics. |
| Yen et al, 2015 ( | Historical Prospective Cohort • 33,300 patients with diabetes, who used metformin • 33,300 patients with diabetes who had not been treated with metformin but were matched by sex, age, and index date and the comorbidities | Incidence of head and neck cancers in patients with diabetes mellitus comparing ever versus never metformin-users. | The incidence of head and neck cancer was 0.64 times lower in the metformin users group (p<0.01). A multivariate Cox proportional hazard regression analysis adjusted for sex, age, comorbidities geographic distribution, and monthly income showed an adjusted HR of 0.66 (95% CI 0.55-0.79) in favor of metformin use. |
| Tseng CH, 2016 ( | Retrospective Cohort • 1,273 patients with Oral cancer in the ever users of metformin group (288,198 patients) • 119 patients with oral cancer in the never users of metformin group (16,263 patients) | Incidence of oral cancer in patients with diabetes mellitus type 2 comparing ever versus never metformin-users. Incidence of oral cancer regarding cumulative doses of metformin. | The incidence of oral cancer in metformin ever users and never users were 92,7/100,000 person-years and 163,6/100,000 person-years, respectively. The overall hazard ratios suggested a significantly lower risk [0.584 (0.483-0.707) for PS-adjusted model, and 0.562 (0.465-0.678) for IPTW model]. |
| Figueiredo et al, 2016 ( | Case-Control Study • 1,021 head and neck cancer (HNC) cases • 1,063 controls | Association between diabetes mellitus and HNC. Impact of metformin use on the risk of HNC. | There was a decreased risk of HNC among diabetic patients (OR 0.68; 95% CI 0.49-0.95). The risk was further decreased among diabetic metformin users (0.54; 95% 0.29-0.99). |
HR, hazard ratio; RR, relative risk; OR, odds ratio; CI, confidence interval
The Taiwanese National Health Research Institutes also looked at head and neck cancer incidence in diabetic patients, according to metformin use.
They found reduced incidence of oral cancer between metformin users [AHR 0.658 (0.48-0.70)] in a time- dependent survival analysis. It could also demonstrate a possible dose-response relationship between metformin and oral cancer incidence, when the time of use was longer than 21.5 months. Another retrospective cohort study comparing clinical- pathological information of patients with laryngeal squamous cell-carcinoma
Another Taiwanese study,
In a Brazilian case-control study, there was also an association between metformin use and decreased head and neck cancer risk (OR 0.68; 95% CI 0.49-0.95).
Several studies also evaluated the preventive effects of metformin in other tumor types such as bladder,
| Author | Study design, population and intervention | Objectives and primary endpoints | Main results |
|---|---|---|---|
| Tseng CH, 2014 ( | • Retrospective cohort 40,8189 type II diabetic patients, using metformin 532,519 type II diabetic patients, metformin never- users | Association between long-term metformin use and incidence of bladder cancer in diabetic patients | The bladder cancer incidence was lower between patients using metformin, when compared with metformin never- users (0.382, CI 0.360-0.405). Duration of the treatment had a protective effect. |
| Mamtani et al, 2014 ( | Retrospective cohort •71,472 type II diabetic patients, new users of metformin •16,128 type II diabetic patients, new users of sulfonylureas | Association between metformin use and bladder cancer incidence in diabetic patients | There was no evidence of a reduction in bladder cancer incidence with the use of metformin (HR 0.81, CI 0.60-1.09]), even after adjusting for treatment duration. |
| Goossens et al, 2015 ( | • Retrospective cohort 132,960 type II diabetic patients, using metformin 32,438 type II diabetic patients, using sulfonylureas | Association between long-term metformin and incidence of bladder cancer in diabetic patients | There was no difference in bladder cancer incidence between patients using metformin and sulfonylureas (HR 1.12, 95% CI 0.90-1.40). |
| Tseng CH, 2016 ( | • Retrospective cohort 171,753 type II diabetic patients, metformin users 75,499 type II diabetic patients, metformin never- users | Association between metformin use and incidence of kidney cancer in diabetic patients | Diabetic patients using metformin had a lower renal cell carcinoma incidence (HR = 0.279, 95% CI 0.254-0.307), when compared to metformin never- users. Duration of the treatment had a protective effect. |
| Becker et al, 2017 ( | • Case-control study 3,506 renal cell carcinoma cases among diabetic patients 21,038 diabetic patients, matched controls | Association between metformin use and renal cell carcinoma incidence | There was no evidence of a protective effect of metformin in renal cell carcinoma risk (adjusted OR = 1.18, CI 0.88-1.58), even between diabetic patients (adjusted OR = 0.91, CI 0.64-1.29). |
| Tseng CH, 2014 ( | • Retrospective cohort 795,321 type II diabetic patients, metformin ever-users 619,402 type II diabetic patients, metformin never- users | Association between metformin use and thyroid cancer incidence among diabetic patients | Results showed a reduced incidence of thyroid cancer among metformin users when compared with never-users (HR 0.68, CI 0.598-0.780). There was also a statistical significant benefit according to time of exposure to metformin. |
| Becker et al, 2015 ( | • Case-control study 1,229 thyroid cancer cases among diabetic patients 7,374 diabetic patients, matched controls | Association between metformin use and thyroid cancer incidence in diabetic patients | There was no evidence of an association between metformin use in diabetic patients and incidence of thyroid cancer (OR 0.70, CI 0.42-1.16). |
| de Jong et al, 2017 ( | • Prospective cohort 37,215 type II diabetic patients using metformin 19,899 type II diabetic patients using other drugs | Risk of gastrointestinal (GI) cancers in patients with type 2 diabetes using metformin applying a time-varying approach to antidiabetic drug | There was no association between GI cancer or specific GI cancer sites and the current use of metformin (HR 0.97, 95% CI 0.82-1.15). No association was seen neither between GI cancer and the cumulative dose of metformin. |
| Chak et al, 2015 ( | • Phase II randomized trial 36 patients randomized to metformin arm 33 patients randomized to placebo arm | Effect of metformin use in the level of pS6K1 Barrett's esophagus biopsies | There was no statistical difference in the median percent change from baseline for pS6K1values, between metformin and placebo arms (p 0.87). |
| Tseng et al, 2017 ( | • Retrospective cohort 288,013 type II diabetic patients, metformin ever-users 16,216 type II diabetic patients, metformin never- users | Association between metformin use and esophageal cancer in type II diabetic patients | There was a significantly lower esophageal cancer risk among metformin ever-users (HR 0.48; 95% CI 0.34-0.68). Analysis in a matched sample consistently supported this result. |
| Kim et al, 2014 ( | • Retrospective cohort Insulin non-users: 26,690 metformin users 6,288 metformin never- users Insulin users: 5,855 metformin users 1,156 metformin never- users | Association between metformin use and gastric cancer among diabetic patients | There was a statistical reduce in gastric cancer incidence among patients who did not use insulin, when comparing metformin users and non-users (HR 0.52; CI 0.34-0.79). There was no difference between metformin users or non-users, among patients that use insulin. |
| Tseng et al, 2016 ( | • Retrospective cohort type II diabetic patients, metformin ever-users type II diabetic patients, metformin never-users | Effect of metformin use in gastric cancer risk | Metformin ever-users had a lower risk of gastric cancer in comparison to never-users (HR 0.44; 95% CI 0.35-0.55). |
| Walker et al, 2015 ( | • Case-control study 536 pancreatic cancer cases among diabetic patients 869 diabetic patients, matched controls | Association between metformin use and pancreatic cancer incidence in diabetic patients | There was no association of metformin use and pancreatic cancer incidence (OR 1.01, CI 0.61-1.68), among diabetic patients. Duration of metformin use was not correlated with cancer risk. |
Of note, two retrospective cohorts were done in Taiwanese patients with type II diabetes mellitus, one evaluating the role of metformin in esophageal and the other in gastric cancer. A significantly lower risk of esophageal cancer (HR 0.48; 95% CI 0.34-0.68) and of gastric cancer (HR 0.44; 95% CI 0.35-0.55) were seen in metformin ever users in comparison with never users.
In this updated systematic review, similarly to our previous one, most studies that evaluated the primary and secondary chemopreventive effects of metformin showed conflicting results, with the great majority being retrospective with diabetic patients.
Specifically in colorectal cancer, pre-clinical and epidemiological studies had previously suggested a role of metformin in the prevention of colorectal pre-malignant lesions.
In the molecular classification of colorectal cancer, the CMS3, known as a metabolic subtype, shows genetic signatures suggesting a dysregulation of metabolic processes,
Until our last review in 2014, there were positive chemopreventive effects in hepatocellular cancer among metformin users.
Although recent retrospective studies have been conducted reinforcing the hypothesis that metformin could have a role in prevention of breast cancer, there are no randomized studies to confirm this assumption; furthermore eight retrospective studies revealed conflicting results.
Another hypothesis concerning metformin use and diabetes itself is that it could influence the risk of different molecular subtypes of breast cancer, also reinforcing the need to correct classification of breast cancers when studying their association with diabetes and this drug. Probably breast cancer is the best model about subdivision of different molecular subtypes of cancer. It is not acceptable anymore to name breast cancer as a unique diagnosis, considering its different risk factors, biological behavior and treatment response. Without understanding the correct molecular pathways that leads to development of each subtype, we may not see whether metformin may prevent or not cancer development. The next steps in metformin- prevention studies must include molecular analysis at randomization and including criteria.
Despite a biological rational that associates endometrial cancer and obesity, that could justify a potential role of metformin in preventing this type of cancer, results of the presented articles were mostly negative, with the exception of one that showed a reduced endometrial cancer incidence in the diabetic population using metformin.
Regarding prostate cancer, retrospective studies have suggested lower incidence of prostate cancer among diabetic patients taking metformin. Most studies relied on large population databases and were performed in a time-dependent survival analysis of metformin exposure. They have shown a numerical tendency towards smaller incidence of cancer in patients that used metformin, especially with prolonged use.
Considering these studies, although no clear association between metformin and cancer prevention was seen, the results still suggest that metformin might have some influence over prostate cancer onset that needs to be better understood. Pre-clinical data suggest that metformin represses prostate cell growth by inducing apoptosis through androgen receptor binding;
We found positive associations between metformin use and lower incidence of lung cancer,
Limitations of this systematic review are the heterogeneity of studies methods, populations and lack of information on metformin doses and time of use, which prevented any attempt to perform pooled analyses. Tumor heterogeneity, for example, in colorectal tumors and molecular profiles of breast cancer also could represent a limitation, because it would be necessary to reclassify tumors properly.
Furthermore, data are limited in terms of length of time necessary to benefit,
In conclusion, the best evidence for metformin as a chemopreventive agent comes from one randomized placebo-controlled trial that showed reduced incidence of colorectal pre-malignant lesions.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.