The Brazilian Constitution grants the right to universal health to all Brazilian citizens. In such context, the Brazilian Unified Health System (Sistema Único de Saúde, SUS, in Portuguese) aims to provide universal health coverage within the country. Pharmaceutical care is also granted, even though there are huge challenges to properly attain these civil rights. It is widely known that the success of oncological treatment is primarily determined by early diagnosis and adequate treatment. This is even more important for time-sensitive diseases, such as bladder cancer. Even though SUS is universal in Brazil, it is not always efficient, and there are situations in which the users seek legal aid aiming to obtain the desired access to health treatments.
To aid in these lawsuits, the Center for Technical Support of the Judiciary (Núcleo de Apoio Técnico do Poder Judiciário, NAT-Jus, in Portuguese) was created. It integrates the judiciary system with relevant health institutions, aiming to help the judges in scientific matters. Since 2019, it has released over 50 thousand technical notes (TNs) based on individual lawsuits (77% regarding medications, 18%, procedures, and 5%, health products).
Currently, there are several challenges in SUS for patients treated for bladder cancer. Waiting times in most public hospitals are long.
These treatments have increased patient survival in the metastatic setting, but they have also increased the costs.
The present study aimed to evaluate lawsuits against SUS to obtain better treatment for patients with bladder/ureteral cancer.
We conducted a cross-sectional study to evaluate the TNs issued by NAT-Jus regarding lawsuits filed by patients against SUS from 2019 to 2023, concerning bladder or ureteral cancer (International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] codes C66 or C67). Maps were created on the MapChart website (mapchart.net). The prices of the medications were based on the list by the Chamber for the Regulation of the Medication Market (Câmara de Regulação do Mercado de Medicamentos, CMED, in Portuguese) of the Brazilian Ministry of Health, considering 18% of tax.
Approval of the Institutional Review Board was not required for the present study, as only anonymous public data was used, according to article 2 of Resolution no. 510/2016 of the Brazilian National Health Council (Conselho Nacional de Saúde, CNS, in Portuguese).
A total of 137 TNs were issued for lawsuits filed by patients being treated for bladder/ureteral cancer. Most plaintiffs were male patients (70.8%), with a mean age of 69.1 ± 17.6 (range: 21–92) years; 129 cases were associated with bladder cancer, and 8, with ureteral cancer.
The lawsuits had been filed with the intent to obtain medications (67%), medical care or procedures (26%), or other health products (7%) (
| Request | Technical note | Favorable | |
|---|---|---|---|
| Surgical procedure | 20 | 75.0% | (15) |
| | 4 | 100.0% | (4) |
| | 9 | 88.9% | (8) |
| | 7 | 42.8% | (3) |
| Specialist consultation | 7 | 100.0% | (7) |
| Hospital admission | 2 | 50.0% | (1) |
| Home care | 2 | 50.0% | (1) |
| Exams | 3 | 0 | (0) |
| Materials | 4 | 100.0% | (4) |
| Medications | 87 | 71.3% | (62) |
| Lawsuits | Favorable | ANVISA approval | CONITEC approval | NCCN guidelines | ||
|---|---|---|---|---|---|---|
| Pembrolizumab | 46 | 69.6% | (32) | Yes | – | Yes |
| Avelumab | 13 | 76.9% | (10) | Yes | – | Yes |
| Atezolizumab | 5 | 40.0% | (2) | Yes | – | Yes |
| Nivolumab | 1 | 100% | (1) | Yes | – | Yes |
| Erdafitinib | 2 | 100% | (2) | Yes | – | Yes |
| Enfortumab vedotin | 1 | 100% | (1) | Yes | – | Yes |
| BCG vaccine | 13 | 92.3% | (12) | Yes | Yes | Yes |
| Chemotherapy | 5 | 40.0% | (2) | Yes | Yes | Yes |
Abbreviations: ANVISA, Agência Nacional de Vigilância Sanitária (Brazilian Health Regulatory Agency); BCG, Bacillus Calmette-Guerin; CONITEC, Comissão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde (National Committee of Incorporation of New Technologies into the Brazilian Unified Health System); NCCN, United States National Comprehensive Care Network.
Pembrolizumab was the medication most often requested by patients undergoing treatment for bladder or ureteral cancer, with 1,349 requests out of more than 50 thousand TNs. Bladder or ureteral cancer was responsible for 3.4% of all of the requests for pembrolizumab. Erdafitinib was the reason for 2 additional TNs, registered under code C64 (kidney cancer), and related to renal pelvis tumors with fibroblast growth factor (FGFR) mutations.
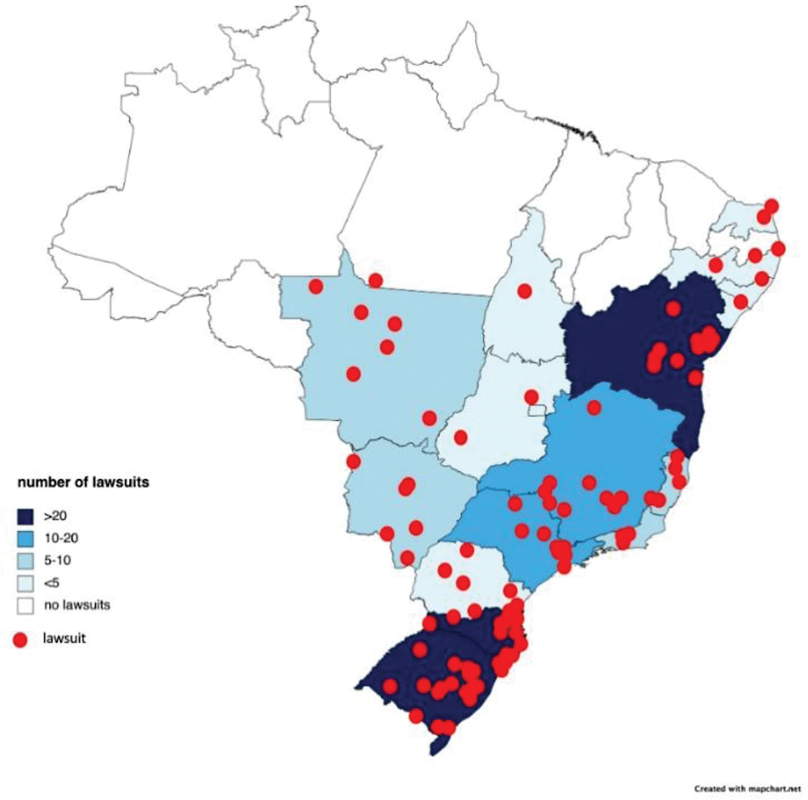
The distribution of the lawsuits in terms of the Brazilian states and cities is outlined in
Map 1 Distribution of lawsuits filed by patients with bladder or ureteral cancer according to Brazilian state.
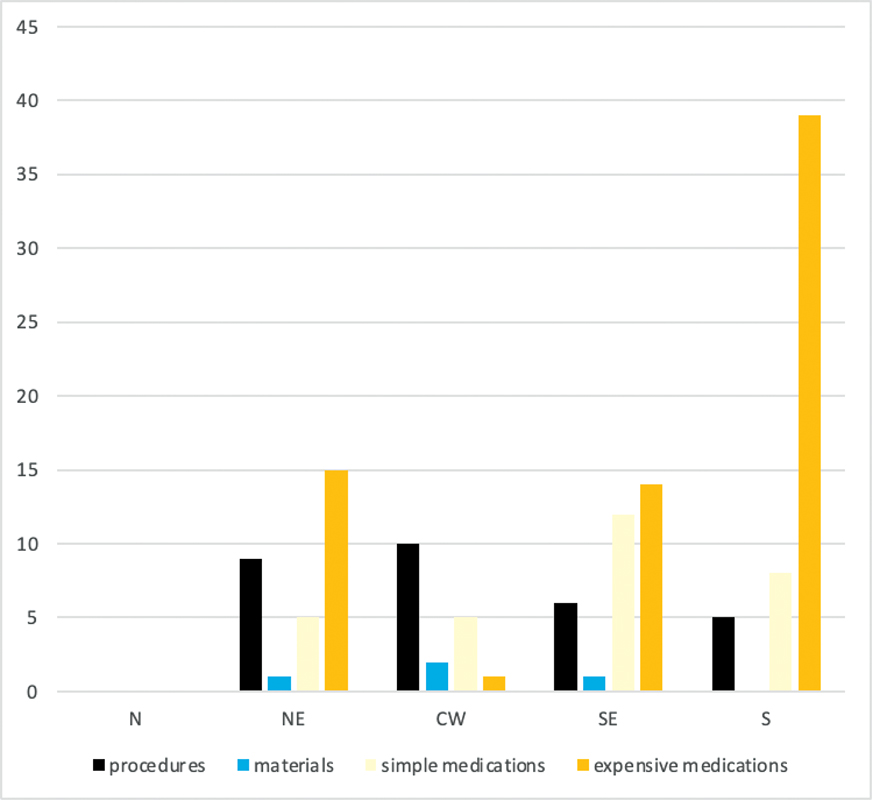
Fig. 1 Distribution of lawsuits according to reason in each Brazilian region. Abbreviations: N, North; NE, Northeast; MW, Midwest; SE, Southeast; S, South.
The costs of some of the medications involved in the lawsuits are demonstrated in
| Drug | Commercial name in Brazil | Manufacturer | Presentation | Price in BRL (no tax) | Price in BRL (+ 18% in tax) | Estimated cost/year (in BRL) |
|---|---|---|---|---|---|---|
| Erdafitinib | (oral) | 753,563.04 | ||||
| Erdafitinib | Erfandel | Janssen | 3 mg X 84 | 33,557.67 | 47,097.68 | |
| Erdafitinib | Erfandel | Janssen | 3 mg X 56 | 50,336.53 | 70,646.54 | |
| Erdafitinib | Erfandel | Janssen | 4 mg X14 | 11,185.89 | 15,699.23 | |
| Erdafitinib | Erfandel | Janssen | 4 mg X28 | 22,371.79 | 31,398.46 | |
| Erdafitinib | Erfandel | Janssen | 4 mg X56 | 44,743.57 | 62,796.91 | |
| Erdafitinib | Erfandel | Janssen | 5 mg X28 | 27,964.74 | 39,248.08 | |
| Pembrolizumab | 312,608.32 | |||||
| Pembrolizumab | Keytruda | Merck Sharp & Dome | 100 mg/mL (4mL) | 13,921.08 | 19,538.02 | |
| Avelumab | (intravenous) | 719,974.08 | ||||
| Avelumab | Bavencio | Merck S/A | 20 mg/mL (10 mL) | 5,343.65 | 7,499.73 | |
| Atezolizumab | (intravenous) | 525,102.40 | ||||
| Atezolizumab | Tecentriq | Roche | 1200 mg (20 mL) | 23,383.87 | 32,818.90 | |
| Atezolizumab | Tecentriq | Roche | 840 mg (14 mL) | 16,368.71 | 22,973.23 | |
| Enfortumab vedotin | (intravenous) | 1,103,811.72 | ||||
| Enfortumab vedotin | Padcev | Adium | 20 mg | 4,853.72 | 6,812.12 | |
| Enfortumab vedotin | Padcev | Adium | 30 mg | 7,282.65 | 10,221.09 | |
| Nivolumab | (intravenous) | 208,405.44 | ||||
| Nivolumab | Opdivo | Bristol-Myers Squibb | 40 mg/mL (4 mL) | 3,093.57 | 4,341.78 | |
| Nivolumab | Opdivo | Bristol-Myers Squibb | 100 mg/mL (10 mL) | 7,733.91 | 10,854.42 | |
| BCG | (intravesical) | 18,768.33 | ||||
| Mycobacterium bovis | Imuno BCG | Fundação Ataulpho de Paiva | 40 mg (1 unit) | 356.59 | – | |
| Mycobacterium bovis | Imuno BCG | Fundação Ataulpho de Paiva | 40 mg (2 units) | 713.20 | – | |
| Mycobacterium bovis | Urohipe | Uno Healthcare | 40 mg (1 unit) | 318.38 | 446.85 | |
| Mycobacterium bovis | Urohipe | Uno Healthcare | 40 mg (2 units) | 636.79 | 893.73 | |
| Gemcitabine | (intravesical) | 28,965.62 | ||||
| Gemcitabine | GCIB | Cristália | 1 g | 1,051.84 | 1,282.73 | |
| Gemcitabine | Gemzar | Eli Lilly BR | 1 g | 1,074.74 | 1,310.66 | |
| Gemcitabine | Gemcitabine | Accord | 1 g | 698.58 | 851.93 | |
| Gemcitabine | Gemcitabine | Zydus Nikkho | 1 g | 698.58 | 851.93 | |
| Gemcitabine | HETGEM | Camber | 1 g | 603.20 | 735.61 | |
| Gemcitabine | Gemcitabine | Farma Vision | 1 g | 603.20 | 735.61 | |
| Vinflunine | (intravenous) | 188,096.00 | ||||
| Vinflinine | Javlor | Pierre Fabre | 25 mg/mL (2 mL) | 602.39 | 845.45 | |
| Vinflunine | Javlor | Pierre Fabre | 25 mg/mL (10mL) | 2939.12 | 4125.02 |
Abbreviations: BCG, Bacillus Calmette-Guerin; CMED, Câmara de Regulação do Mercado de Medicamentos (Chamber for the Regulation of the Medication Market).
The incidence and prevalence of bladder cancer is increasing in Brazil.
The SUS is a universal health system, and health care is a constitutional legal right in Brazil. The three branches of power of the Brazilian government work to balance these rights. Whereas the Executive branch manages SUS, the Judicial branch can be assessed by anyone who believes that their rights are not fully granted.
Even though Brazil is one of the few countries that recognizes health as a legal right, SUS faces serious challenges, such as underfunding, improper distribution of health services throughout the country, population aging, lack of precise information, etc.
Access to medications has been one of the most common demands in Brazilian courts in lawsuits filed by oncological patients. These lawsuits are normally associated with a high economic burden, and they must be evaluated with caution. There are specific criteria that are recommended in this judicial decision process: a technical analysis; medication registry in the Brazilian Health Regulatory Agency (Agência Nacional de Vigilância Sanitária, ANVISA, in Portuguese); clinical guidelines; incorporation of the medication into SUS (after CONITEC approval); inclusion of the medication in specific documents such as the Health Ministry's Diagnostic and Therapeutic Guidelines (Diretrizes Diagnósticas e Terapêuticas, DDT, in Portuguese) or the Clinical Protocols and Therapeutic Guidelines (Protocolos Clínicos e Diretrizes Terapêuticas PCDT, in Portuguese), which guide cancer treatments in SUS.
Bladder cancer is already known to be an expensive disease.
The analysis of the lawsuits demonstrates contrasting realities. Whereas some patients are demanding relatively inexpensive treatments that should be promptly granted, others are demanding new and expensive technologies. Overall, the TNs were favorable in 72.3% of the lawsuits involving bladder/ureteral cancer. This rate is very similar to the ones previously reported in a study
There were 20 lawsuits demanding the right to surgical procedures: 4 of them were demanding cystoscopies and 9, transurethral resections of bladder tumors (TURBTs). These are essential procedures when treating a patient with bladder cancer, and they are already granted by law. The TNs were favorable in all of these cases, except one. More than 63% of these cases occurred in the Northeastern and Midwestern regions, which present lower Human Development Index (HDI) and less access to health services.
In two cases, patients required access to robotic and minimally-invasive technology to perform surgery, and an unfavorable recommendation was given in both cases. Additionally, there were 7 lawsuits demanding a specialist consultation (all came out favorable), 2 demanding hospital admission (50% favorable) and 2 demanding home-care treatment (50% favorable). Day-use materials such as diapers and catheters were demanded by 4 patients (100% favorable). In 3 cases, exams (positron-emission tomography [PET] scan) were required (100% unfavorable).
Lawsuits demanding medications were the most common, and some demanded access to basic treatments. In 12 cases, simple medications such as analgesics or nutritional supplements were the main issue (75% favorable). In 13 cases, the BCG vaccine was requested (92.3% favorable), and in 5, chemotherapeutic agents were requested (40% favorable).
However, most lawsuits requested access to expensive medications. The most requested drug was pembrolizumab (n = 66; 69.6% favorable), followed by avelumab (n = 13; 76.9% favorable), atezolizumab (n = 5; 50% favorable), erdafitinib (n = 2; 100% favorable), and enfortumab vedotin (n = 1; 100% favorable). Of the total, 56% of the requests for these expensive medications occurred in the Southern region, which is known to present a higher HDI and better access to health services.
The BCG vaccine and chemotherapeutic agents are recommended by guidelines, and they have been approved by ANVISA and CONITEC. Immunotherapeutic drugs, enfortumab vedotin, and erdafitinib are also recommended by guidelines and approved by ANVISA. However, these expensive drugs were not incorporated into SUS by CONITEC.
The CONITEC is the institution that evaluates the efficacy and safety of medications, and it also provides the Ministry of Health with a cost-effectiveness point of view. Recently, the concept of cost-effectiveness thresholds has been debated.
The TNs for lawsuits demanding IO therapeutic agents, TTs, or ADCs (IO + TT + ADC) for patients with bladder cancer aimed at obtaining BRL 58.4 million in the studied period. The Brazilian Federal Government lost the causes, representing BRL 42.1 million in expenses with IO + TT + ADC medications within the period evaluated.
In the period evaluated (2019–2023), 88 thousand TNs were issued,
Federal expenditures with public health in Brazil were of approximately BRL 115.3 billion/year in the last years. There is an estimated deficit of BRL 21.7 billion each year. There are currently 520 thousand lawsuits regarding health issues. Over 50% of them are related to medications, and more than 90% are associated with medications not currently offered by SUS.
For bladder cancer, these lawsuits might skyrocket in the next few years. Immunotherapy is now used for NMIBC, MIBC, and metastatic bladder cancer. However, in the last year, a new combination of treatments has more than doubled the overall survival of patients with bladder cancer, an outcome rarely seen in oncologic drug development. It has been granted United States Food and Drug Administration (FDA) approval and caused a change in the guidelines of the United States National Comprehensive Care Network (NCCN) as a new first-line treatment for metastatic bladder cancer.
Currently, patients in Brazil with metastatic bladder cancer are mostly treated with chemotherapy regimens such as gemcitabine-cisplatin, gemcitabine-carboplatin, and methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC), with a total expenditure of treatment (6 cycles) ranging from BRL 30 thousand to BRL 50 thousand. However, the current NCCN guidelines recommend three main regiments as first-line options for patients with metastatic bladder cancer: chemotherapy followed by switch maintenance with avelumab; pembrolizumab; or the combination of pembrolizumab and enfortumab vedotin. These treatments would represent expenditures of BRL 769,974.08/year (chemotherapy + avelumab), BRL 312,608.32/year (pembrolizumab), and BRL 1,085,276.52/year (pembrolizumab + enfortumab vedotin). Therefore, not only prices might dramatically increase, but also, instead of a 3-month course of chemotherapy, patients in the new regimens will receive lifelong treatments.
If a rational and cautious evaluation of the incorporation of new technology into SUS is not adopted, the system will soon collapse. In such a context, further studies and collaborations between the government, the scientific community, the judiciary system, and patient advocacy organizations are extremely necessary and should be encouraged. New technologies are extremely beneficial for the medical practice; therefore, the Brazilian government has to face this reality and properly address viable solutions.
The Brazilian Constitution guarantees the right to universal healthcare for all citizens through SUS. However, there are significant challenges in realizing these rights, with patients resorting to the judicial system to access treatments. Bladder cancer treatment within SUS faces obstacles such as long queues and shortages of essential medications. Moreover, advanced and costly therapies are not widely available, straining SUS and resulting in increasing legal costs. Collaboration between the government, the scientific community, and patient advocacy organizations is crucial to ensure the sustainability of SUS in the face of these challenges.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Vidal, T J and Moraes, E L and Retto, M PF and Silva, M JSD. Demandas judiciais por medicamentos antineoplásicos: a ponta de um iceberg?. Cien Saude Colet [online]. 2017, vol. 22, p. 2539-2548.
2. [cited 2023 Dec 2] [online]. Available from: <https://www10.trf2.jus.br/portal/judiciario-vai-avaliar-impacto-das-notas-tecnicas-de-saude-nas-decisoes-judiciais/>.
3. Korkes, F and Timóteo, F and Martins, S. Dramatic Impact of Centralization and a Multidisciplinary Bladder Cancer Program in Reducing Mortality: The CABEM Project. JCO Glob Oncol [online]. 2021, vol. 7, p. 1547-1555.
4. Korkes, F and Palou, J. High mortality rates after radical cystectomy: we must have acceptable protocols and consider the rationale of cutaneous ureterostomy for high-risk patients. Int Braz J Urol [online]. 2019, vol. 45, p. 1090-1093.
5. Korkes, F and Timóteo, F and Ferrari, K L and Reis, L O. Bacillus Calmette-Guérin (BCG) Brazilian Backstage in Bladder Cancer. Int Braz J Urol [online]. 2021, vol. 47, p. 232-236.
6. iROC Study Team. Effect of Robot-Assisted Radical Cystectomy With Intracorporeal Urinary Diversion vs Open Radical Cystectomy on 90-Day Morbidity and Mortality Among Patients With Bladder Cancer: A Randomized Clinical Trial. JAMA [online]. 2022, vol. 327, p. 2092-2103.
7. Powles, T and Park, S H and Voog, E. Maintenance avelumab + best supportive care (BSC) versus BSC alone after platinum-based first-line (1L) chemotherapy in advanced urothelial carcinoma (UC): JAVELIN Bladder 100 phase III interim analysis. J Clin Oncol [online]. 2020, vol. 38, p. LBA1-LBA1.
8. Powles, T and Park, S H and Caserta, C. Avelumab First-Line Maintenance for Advanced Urothelial Carcinoma: Results From the JAVELIN Bladder 100 Trial After ≥2 Years of Follow-Up. J Clin Oncol [online]. 2023, vol. 41, p. 3486-3492.
9. Suzman, D L and Agrawal, S and Ning, Y M. FDA Approval Summary: Atezolizumab or Pembrolizumab for the Treatment of Patients with Advanced Urothelial Carcinoma Ineligible for Cisplatin-Containing Chemotherapy. Oncologist [online]. 2019, vol. 24, p. 563-569.
10. THOR Cohort 1 Investigators. Erdafitinib or Chemotherapy in Advanced or Metastatic Urothelial Carcinoma. N Engl J Med [online]. 2023, vol. 389, p. 1961-1971.
11. BLC2001 Study Group. Erdafitinib in Locally Advanced or Metastatic Urothelial Carcinoma. N Engl J Med [online]. 2019, vol. 381, p. 338-348.
12. [cited 2020 Jul 1] [online]. Available from: <https://www.cancer.org/latest-news/fda-approves-padcev-enfortumab-vedotin-ejfv-for-bladder-cancer.html>.
13. Korkes, F and Maluf, F. Increasing costs from bladder cancer in the Brazilian Health System: the role of establishing public health policies. Int Braz J Urol [online]. 2021, vol. 47, p. 443-447.
14. Korkes, F and Timóteo, F and Soledade, L CB. Stage-Related Cost of Treatment of Bladder Cancer in Brazil. PharmacoEconom Open [online]. 2022, vol. 6, p. 461-468.
15. [cited 2023 Dec 3] [online]. Available from: <https://www.gov.br/anvisa/pt-br/assuntos/medicamentos/cmed>.
16. Timoteo, F and Korkes, F and Baccaglini, W and Glina, S. Bladder cancer trends and mortality in the brazilian public health system. Int Braz J Urol [online]. 2020, vol. 46, p. 224-233.
17. Sievert, K D and Amend, B and Nagele, U. Economic aspects of bladder cancer: what are the benefits and costs?. World J Urol [online]. 2009, vol. 27, p. 295-300.
18. Coelho, T L and Ferré, F and Campos Neto, O H and Acurcio, F de A and Cherchiglia, M L and Andrade, E IG. Legal and health variations in drug litigation injunctions granted in Minas Gerais. Rev Saude Publica [online]. 2014, vol. 48, p. 808-816.
19. Pichon-Riviere, A and Drummond, M and Palacios, A and Garcia-Marti, S and Augustovski, F. Determining the efficiency path to universal health coverage: cost-effectiveness thresholds for 174 countries based on growth in life expectancy and health expenditures. Lancet Glob Health [online]. 2023, vol. 11, p. e833-e842.
20. [cited 2023 Dec 2] [online]. Available from: <https://www.gov.br/conitec/pt-br/assuntos/noticias/2022/setembro/conitec-aprova-proposta-de-uso-de-limiares-de-custo-efetividade-lce-nas-decisoes-em-saude>.
21. [cited 2023 Dec 2] [online]. Available from: <https://www.sites.tcu.gov.br/listadealtorisco/sistema_unico_de_saude_acesso_e_sustentabilidade.html>.
22. [cited 2023 Dec 2] [online]. Available from: <https://www.cnj.jus.br/impactos-da-judicializacao-da-saude-sao-debatidos-no-i-congresso-do-fonajus/>.
23. [cited 2023 Dec 5] [online]. Available from: <https://www.ejef.tjmg.jus.br/e-natjus-disponibiliza-novas-funcionalidades/>.
24. [cited 2023 Dec 5] [online]. Available from: <https://www.agenciabrasil.ebc.com.br/saude/noticia/2023-05>.
25. [cited 2023 Dec 5] [online]. Available from: <https://www.conjur.com.br/2022-nov-17/cnj-promove-evento-debater-demandas-saude-judiciario/>.
26. [cited 2023 Dec 5] [online]. Available from: <https://www.cnj.jus.br/tcu-e-estados-apontam-aumento-dos-gastos-com-a-judicializacao-da-saude/>.
27. Powles, T B and Perez Valderrama, B and Gupta, S. LBA6 EV-302/KEYNOTE-A39: Open-label, randomized phase III study of enfortumab vedotin in combination with pembrolizumab (EV+P) vs chemotherapy (Chemo) in previously untreated locally advanced metastatic urothelial carcinoma (la/mUC). Ann Oncol [online]. 2023, vol. 34, p. S1340.
Dados de acesso insuficientes para visualização no mapa.