Irradiation of the pelvis is an essential component of the contemporary multidisciplinary approach to treat locally-advanced rectal cancer. Neoadjuvant therapy consisting of concurrent radiation and 5-fluorouracil (5-FU) chemotherapy prior to surgery has been shown to improve both recurrence-free and overall survival rates in patients with locally-advanced rectal cancer. Patients who are of reproductive age run a significant risk due to the presence of seminiferous tubules adjacent to the radiation treatment field. Even a single dose as low as 0.78 Gy is sufficient to cause azoospermia in almost all cases.
More focus has been placed on the adverse effects of the multimodal treatment in recent years as a result of an increase in the percentage of patients with advanced rectal cancer who are still alive.
In terms of the effects of radiation on the testicles, there are two distinct compartments. First, the highly radiosensitive seminiferous tubules, which is the site of spermatogenesis in the male reproductive system. Second, the Leydig cells, which are those that produce testosterone, are thought to be less radiosensitive than spermatogonia.
If the therapy causes hypogonadism, this may have a profound impact on quality of life (QoL). This is frequently demonstrated by subtle changes, such as a reduction in lean body and muscle mass, as well as the development of psychological problems, such as a loss of libido, energy, and drive, or even depression and anxiety.
Hence in the present study, we determined the radiation doses that were administered to the testicles of male patients undergoing radiotherapy (RT) for the treatment of rectal cancer. We paid particular attention to the dose contribution of different radiation-delivery techniques to the testicles. In addition, we analyzed the effect of the treatment on sexual life using a QoL questionnaire. This research was submitted to and approved by the Ethics Committee under submission number KMIO/MEC/011/03.2018.
The study included 40 male patients with locally-advanced rectal cancer, who were sexually active, aged between 25 and 50 years, who would undergo neoadjuvant therapy followed by total mesorectal resection. Patients with comorbidities (diabetes, hypertension, cardiac diseases, and psychiatric illness), using drugs that affected sexual performance, and those with preexisting sexual/genital abnormalities were excluded. A neo adjuvant RT dose of 1.8 Gy per fr 5 days per week totaling a dose of 45 Gy in 25frs delivered in the supine position with thermoplastic immobilization was administered. Oral capecitabine 825 mg/m2 was adminstered concurrently on the days of the radiation treatment. Planning was performed for three techniques: three-dimensional conformal radiotherapy (3DCRT), intensity-modulated radiotherapy (IMRT), and volumetric-modulated arc therapy (VMAT); the testicular dose, testicular volume, tumor length and thickness, planning target volume (PTV), and the distance of the tumor from the anal verge in each plan were recorded. Finally, the effect of the treatment on sexual life was assessed through the QoL questionnaire pertaining only to sexual activity by European Organization for Research and Treatment of Cancer Quality of Life in Colorectal EORTC (QLQ-CR29) and the Functional Assessment of Cancer Therapy–Colorectal (FACT-C) after a minimum follow-up of 3 years.
We conducted descriptive and inferential statistical analyses; the continuous variables were expressed as mean ± standard deviation (SD) values, and the categorical variables were expressed ad numbers and percentages. The significance level was set to 5%.
One-way analysis of variance (ANOVA) was employed to determine if there were any statistically significant differences regarding the means of three or more independent (unrelated) groups. Specifically, it tests the null hypothesis.
The Student t-test (two-tailed, independent) was used to find the significance of study parameters on continuous scale between two groups (intergroup analysis) on metric parameters. The homogeneity of variance was assessed through the Levene test. The Pearson correlation was applied to the study variables to find their degree of relationship. The p-value was determined by referring to a t-distribution with n-2 degrees of freedom.
We used the IBM SPSS Statistics for Windows (IBM Corp., Armonk, NY, United States), version 22.0, and the R environment (R Foundation for Statistical Computing, Vienna, Austria), version 3.2.2, for the analysis of the data, and the Microsoft Word and Excel (Microsoft Corp., Redmond, WA, United States) were used to generate graphs, tables etc.
In the present study, the median age of the sample was of 38 years, and most patients presented moderately-differentiated adenocarcinomas, most commonly of 1b nodal status, T2 tumor stage, and Tumor, Node, Metastasis (TNM) stage IIIC; moreover 26/40 participants had a PTV ranging from of 1,000 to 1,500 cc.
The overview of the factors assessed in the study (
| Age: median (range) | 38 (range: 20–50) years |
| Histology (adenocarcinoma): n(%) | Well-differentiated: 14(35%) |
| Moderately-differentiated: 22(55%) | |
| Poorly-differentiated: 4(10%) | |
| Tumor, Node, Metatstasis stage: n(%) | IIA- 6(15%) |
| IIIA- 11(27.5%) | |
| IIIB- 10(25%) | |
| IIIC- 13(32.5%) | |
| Volume of the right testicle (cm3): mean ± SD | 21.29 ± 9.72 |
| Volume of the left testicle (cm3): mean ± SD | 17.47 ± 6.95 |
| External genitalia (cm3) | 264.63 ± 70.9 |
| Planning target volume (cm3): mean ± SD | 1350.9 ± 340.88 |
| Tumor length (cm): mean ± SD | 7.17 ± 2.71 |
| Tumor thickness (cm): mean ± SD | 1.71 ± 1.12 |
| Distance of the tumor from the anal verge (cm): mean ± SD | 3.6 ± 2.48 |
| Follow-up | Minimum of 3 years; all patients completed the follow-up |
| Patients alive at the end of the follow-up: n(%) | 31(77.5%) |
| Participants assessed through the EORTC QLQ-CR29 and FACT-C: n(%) | 27(67.5%) out of 31(77.5%) alive included |
Abbreviations: EORTC QLQ-CR29, European Organization for Research and Treatment of Cancer Quality of Life in Colorectal; FACT-C, Functional Assessment of Cancer Therapy–Colorectal; SD, standard deviation.
| Correlation with | Tumor length (cm) | Tumor thickness(cm) | Distance of the tumor from the anal verge (cm) | |||
|---|---|---|---|---|---|---|
| r-value | p-value | r-value | p-value | r-value | p-value | |
| IMRT (mean) | ||||||
| Dose to the right testis (cGy) | 0.003 | 0.987 | 0.149 | 0.358 | -0.004 | 0.982 |
| Dose to the left testis (cGY) | -0.039 | 0.812 | 0.170 | 0.294 | 0.031 | 0.851 |
| Dose to the external genitalia (cGy) | 0.193 | 0.234 | 0.251 | 0.119 | -0.234 | 0.146 |
| 3DCRT (mean) | ||||||
| Dose to the right testis (cGy) | 0.070 | 0.667 | 0.164 | 0.312 | -0.101 | 0.534 |
| Dose to the left testis (cGY) | -0.104 | 0.523 | 0.169 | 0.296 | -0.104 | 0.525 |
| Dose to the external genitalia (cGy) | 0.061 | 0.706 | 0.260 | 0.105 | -0.248 | 0.123 |
| VMAT (mean) | ||||||
| Dose to the right testis (cGy) | 0.202 | 0.212 | 0.286 | 0.174 | -0.091 | 0.577 |
| Dose to the left testis (cGY) | 0.128 | 0.431 | 0.283 | 0.177 | -0.063 | 0.697 |
| Dose to the external genitalia (cGy) | 0.309 | 0.523 | 0.268 | 0.195 | -0.273 | 0.188 |
Abbreviations: 3DCRT, three-dimensional conformal radiotherapy; IMRT, intensity-modulated radiotherapy; VMAT, volumetric-modulated arc therapy.
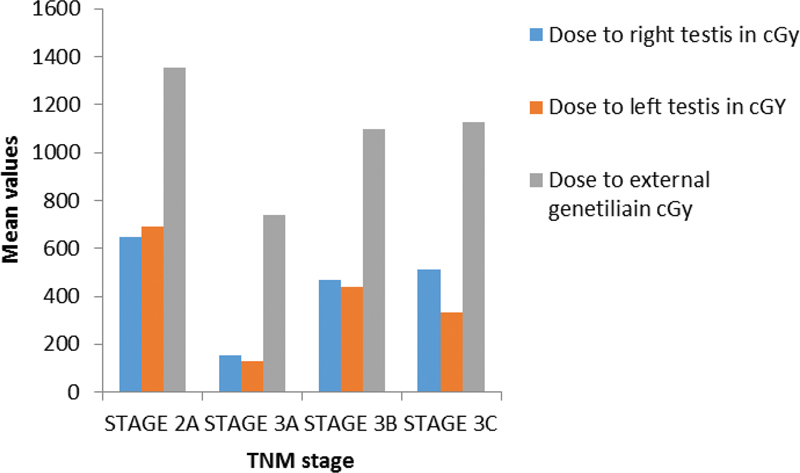
The dose of radiation delivered by IMRT to both right and left testis and the external genitalia was higher in patients in stage IIA than in those in stage IIIC (
Fig. 1 Dose of intensity- modulated radiotherapy (IMRT) based on the Tumor, Node, Metastasis (TNM) stage.
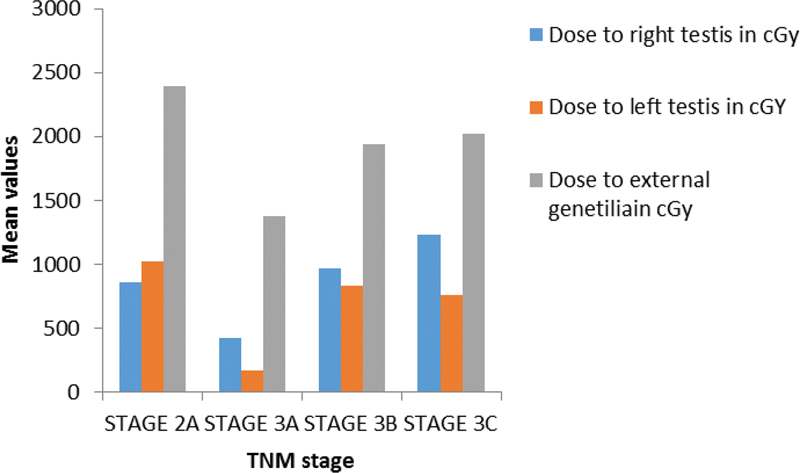
The dose delivered to the right testis by 3DCRT was higher in patients in stage IIIC, but was higher in the left testis and external genitalia in subjects in stage IIA (
Fig. 2 Correlation of the dose delivered to the TNM stage.
When VMAT protocol was delivered, the radiation dose to the right and left testis and the external genitalia was compared with the staging. There was a statistically significant difference regarding the stages of rectal cancer and the dose delivered to the left testis. However, when we compared the dose delivered to the PTV, there was no statistically significant difference regarding the right and left testis and the external genitalia (
| PTV cc | p-value | |||
|---|---|---|---|---|
| < 1,000 | 1,000-1,500 | > 1,500 | ||
| IMRT: mean ± SD | ||||
| Dose to the right testis (cGy) | 287.93 ± 394.19 | 326.72 ± 475.09 | 693.27 ± 803.73 | 0.212 |
| Dose to the left testis (cGY) | 225.78 ± 277.7 | 255.25 ± 413.89 | 624.56 ± 675.09 | 0.120 |
| Dose to the external genitalia (cGy) | 690.43 ± 343.9 | 912.82 ± 472.63 | 1485.17 ± 615.78 | 0.007** |
| 3DCRT: mean ± SD | ||||
| Dose to the right testis (cGy) | 909.23 ± 1455.77 | 708.26 ± 904.89 | 1362.18 ± 1232.33 | 0.257 |
| Dose to the left testis (cGY) | 789.4 ± 1242.17 | 434.81 ± 552.76 | 1140.69 ± 1353.26 | 0.107 |
| Dose to the external genitalia (cGy) | 1932.53 ± 1082.5 | 1658.17 ± 892.22 | 2341.09 ± 1276.84 | 0.206 |
| VMAT: mean ± SD | ||||
| Dose to the right testis (cGy) | 254.68 ± 342.73 | 381.98 ± 478.74 | 400.09 ± 277 | 0.837 |
| Dose to the left testis (cGY) | 229.13 ± 302.55 | 356.35 ± 469.94 | 342.04 ± 221.29 | 0.847 |
| Dose to the external genitalia (cGy) | 736.75 ± 370.34 | 1034.82 ± 574.39 | 1333.49 ± 576.02 | 0.171 |
Abbreviations: 3DCRT, three-dimensional conformal radiotherapy; IMRT, intensity-modulated radiotherapy; PTV, Planning target volume; SD, standard deviation; VMAT, volumetric-modulated arc therapy.
The 31 patients who were alive were submitted to a QoL analysis in terms of sexual activity: 4 patients did not respond, but the 27 patients who responded said they had resumed sexual activity without difficulty (score of 4). Most subjects had resumed their normal sexual life three months after the treatment. All patients reported that the main reason for delay in resuming sexual activity was nervousness about disease recurrence.
The present study results shows that treatment technique and PTV bear an influence on the incidental testicular dose, and it also highlights whether or not the tumor length and thickness, as well as the distance from the anal verge contribute enough to have an impact. One of the most interesting aspects of the study is the assessment of sexual life, which is also an integral QoL domain.
Various studies in literature have evaluated changes in the testicular dose among patients receiving external-beam RT for pelvic malignancy. Piroth et al.
Martin et al.
We would like to point out that most of the trials in the literature evaluate incidental testicular RT dose in prostate malignancy, whereas there is very limited data on dose contribution in carcinoma of the rectum. And even in those studies, a major limiting factor is the assessment restricted to the 3 and 4-field RT delivery techniques. Hence, the analysis of the contribution of the radiation dose performed in the present study, with currently-employed conformal techniques (3DCRT, IMRT, and VMAT) in the treatment of rectal cancer around the world, is helpful in providing the much needed data.
In our institutional Scientific Review Board, it was pointed out to us the non-inclusion/non-utilization of testicular shielding, prone position, dose beyond 25 fr as a boost, and short-course RT. In the routine clinical practice, testicular shielding is not included in the treatment of carcinoma of the rectum, and since we perform long-course RT, with 45Gy/25fr as per the institutional protocol based on ACCORD 12/0405 PRODIGE 2 randomized trial,
One of the major limitations to the present study was the lack of assessment of testosterone levels prior to, during, and after the treatment. Since the planned treatment for rectal cancer was neoadjuvant therapy followed by mesorectal excision, the goal of the study was to assess whether there is any toxicity in the routine treatment practice; hence, we did not assess the testosterone levels in the present study.
In a review, Cherven et al.
In the current study, we found that many patients were reluctant to resume their sexual life out of concern about recurrence, fear of transferring an illness to the spouse/partner, and a feeling of embarrassment to discuss their sexual life with the clinicians or even with their spouse/partner. Most patients started showing improvements in QoL at the third month of follow-up, once they had gained enough confidence. According to a review by Bober and Varela,
The main idea behind the present study was to assess if the conformal techniques used to treat carcinoma of the rectum can lead to sexual dysfunction due to incidental testicular dose or not. The study findings shed light on the need to address the physical aspect of treating the disease, as well as the psychosocial, sexual and emotional aspects associated with the treatment; the findings also highlight the need for comprehensive patient counseling to clear any doubts which may hinder cancer survivals to resume their normal lives,. thereby mitigating any apprehensions faced by the patients and their spouse/partner while making treatment decisions based on the suggestions made by the clinicians.
In the current study, IMRT showed a significant reduction in the testicular dose when compared to 3DCRT and VMAT, the PTV had a statistically significant impact on the testicular dose, and, after the third month of follow-up, most patients resumed their sexual life.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Hermann, R M and Henkel, K and Christiansen, H. Testicular dose and hormonal changes after radiotherapy of rectal cancer. Radiother Oncol [online]. 2005, vol. 75, p. 83-88.
2. Martin, J M and Handorf, E A and Price, R A. Comparison of testicular dose delivered by intensity-modulated radiation therapy (IMRT) and volumetric-modulated arc therapy (VMAT) in patients with prostate cancer. Med Dosim [online]. 2015, vol. 40, p. 186-189.
3. Buchli, C and Martling, A and Arver, S and Holm, T. Testicular function after radiotherapy for rectal cancer–a review. J Sex Med [online]. 2011, vol. 8, p. 3220-3226.
4. Nichols, R C and Hu, C and Bahary, J P. Serum testosterone changes in patients treated with radiation therapy alone for prostate cancer on NRG oncology RTOG 9408. Adv Radiat Oncol [online]. 2017, vol. 2, p. 608-614.
5. King, C R and Brooks, J D and Gill, H and Presti, J C. Long-term outcomes from a prospective trial of stereotactic body radiotherapy for low-risk prostate cancer. Int J Radiat Oncol Biol Phys [online]. 2012, vol. 82, p. 877-882.
6. Zelefsky, M J and Fuks, Z and Hunt, M. High-dose intensity modulated radiation therapy for prostate cancer: early toxicity and biochemical outcome in 772 patients. Int J Radiat Oncol Biol Phys [online]. 2002, vol. 53, p. 1111-1116.
7. Ghadimi, M and Rödel, C and Hofheinz, R and Flebbe, H and Grade, M. Multimodal treatment of rectal cancer. Dtsch Arztebl Int [online]. 2022, vol. 119, p. 570-580.
8. Meistrich, M L. Effects of chemotherapy and radiotherapy on spermatogenesis in humans. Fertil Steril [online]. 2013, vol. 100, p. 1180-1186.
9. Izard, M A. Leydig cell function and radiation: a review of the literature. Radiother Oncol [online]. 1995, vol. 34, p. 1-8.
10. Kinsella, T J and Trivette, G and Rowland, J. Long-term follow-up of testicular function following radiation therapy for early-stage Hodgkin's disease. J Clin Oncol [online]. 1989, vol. 7, p. 718-724.
11. Dueland, S and Guren, M G and Olsen, D R and Poulsen, J P and Magne Tveit, K. Radiation therapy induced changes in male sex hormone levels in rectal cancer patients. Radiother Oncol [online]. 2003, vol. 68, p. 249-253.
12. Suresh, K and Chandrashekara, S. Sample size estimation and power analysis for clinical research studies. J Hum Reprod Sci [online]. 2012, vol. 5, p. 7-13.
13. Corp, I BM. IBM SPSS Statistics for Windows, Version 22.0. IBM Corp., 2013.
14. Piroth, M D and Hensley, F and Wannenmacher, M and Zierhut, D. [Male gonadal dose in adjuvant 3-d-pelvic irradiation after anterior resection of rectal cancer. Influence to fertility]. Strahlenther Onkol [online]. 2003, vol. 179, p. 754-759.
15. Gérard, J P and Azria, D and Gourgou-Bourgade, S. Clinical outcome of the ACCORD 12/0405 PRODIGE 2 randomized trial in rectal cancer. J Clin Oncol [online]. 2012, vol. 30, p. 4558-4565.
16. Cherven, B and Sampson, A and Bober, S L. Sexual health among adolescent and young adult cancer survivors: A scoping review from the Children's Oncology Group Adolescent and Young Adult Oncology Discipline Committee. CA Cancer J Clin [online]. 2021, vol. 71, p. 250-263.
17. Bober, S L and Varela, V S. Sexuality in adult cancer survivors: challenges and intervention. J Clin Oncol [online]. 2012, vol. 30, p. 3712-3719.
Dados de acesso insuficientes para visualização no mapa.