Cervical cancer is a significant public health concern worldwide, ranking fourth in incidence and mortality among women in 2020.
The International Federation of Gynecology and Obstetrics (Fédération Internationale de Gynécologie et d'Obstétrique, FIGO, in French) staging system guides prognosis and treatment decisions by evaluating the extent of tumor invasion in the cervix and adjacent tissues such as the vagina, bladder, and rectum, along with lymph node involvement and metastasis to distant organs.
Classically, according to the main treatment guidelines,
Dueñas-González et al.
Given these considerations, there is a need to evaluate the effectiveness and tolerability of cisplatin and gemcitabine-based CRT in real-world settings, particularly in resource-limited regions. The present study aimed to compare the survival outcomes and toxicity profiles of patients with locally-advanced cervical cancer treated with cisplatin alone versus cisplatin plus gemcitabine at a high-complexity oncology center in the state of Acre, Brazil.
The current was a retrospective observational cohort study based on the analysis of medical records. The study aimed to evaluate the survival outcomes and treatment-related toxicity in patients with locally-advanced cervical cancer undergoing CRT protocols with cisplatin 40 mg/m2 alone or in combination with gemcitabine 125 to 300 mg/m2, administered weekly for 4 to 6 cycles, concurrently with external-beam radiotherapy (EBRT). No adjuvant chemotherapy was administered after the completion of radiotherapy in either group.
All patients received EBRT using cobalt-60 (Co60) at 1.25 MeV through a conformal technique, with a conventional fractionation regimen of 45 to 50.4 Gy delivered in 25 to 28 fractions. The CT was administered concomitantly with RT. Subsequently, high-dose-rate (HDR) brachytherapy was performed, delivering a total dose of 28 Gy to point A, divided into 4 insertions of 700 cGy per session, using an iridium-192 source.
The eligible patients were women diagnosed with cervical cancer (code C53 on the International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10]), staged according to the 2009 FIGO classification system, treated at the High-Complexity Oncology Unit in Rio Branco, Acre, between 2009 and 2016. Patients were required to have undergone 4 to 6 cycles of CT with either cisplatin alone or cisplatin combined with gemcitabine, concomitant with RT.
The exclusion criteria were incomplete medical records or illegible documentation that precluded data analysis. Data were collected on demographic and clinical variables, including age at diagnosis, histological subtype, FIGO stage, treatment initiation date, CT regimen and number of cycles, toxicity of the CT, recurrence date, death date, and last follow-up date for surviving patients.
Hematologic toxicities, including anemia, neutropenia, and thrombocytopenia, were graded according to the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0.
The categorical variables were analyzed using frequency distributions. Group comparisons were performed using the Pearson's Chi-squared test or the Fisher's exact test, as appropriate. The continuous variables were analyzed using descriptive statistics (median and standard deviation values). The Kolmogorov-Smirnov and Shapiro-Wilk tests were used to assess normality. Depending on data distribution, comparisons were performed using either the Student's t-test or the Wilcoxon rank-sum test.
The PFS and OS probabilities were estimated using the Kaplan-Meier method. Survival differences between groups were compared with the log-rank test. The Cox proportional hazards regression model was used to calculate hazard ratios (HRs) and 95%CIs to evaluate the impact of the prognostic variables on survival outcomes.
Toxicity incidence rates between the two groups were compared using the Pearson's Chi-squared test or the Fisher's exact test. A significance level of p < 0.05 was adopted for all statistical analyses. All statistical procedures were performed using the IBM SPSS Statistics for Windows (IBM Corp.) software, version 20.0.
Between 2009 and 2016, 54 patients with locally-advanced cervical cancer who underwent concurrent CRT were selected and divided into 2 groups for comparison. Group 1 (n = 27) received cisplatin alone, while group 2 (n = 27) received cisplatin combined with gemcitabine. By the time of data collection (March 2024), 43 of the 54 patients (79.6%) had died. The median follow-up was of 26.4 (range: 6.8–42.3) months.
According to the demographic data of the groups (
| Variables | Total | Group 1 | Group 2 | p-value | |||
|---|---|---|---|---|---|---|---|
| N = 54 | % | N = 27 | % | N = 27 | % | ||
| Age (years) | 0.586 | ||||||
| ≤ 46 | 28 | 51.9 | 15 | 55.6 | 13 | 48.1 | |
| > 46 | 26 | 48.1 | 12 | 44.4 | 14 | 51.9 | |
| Histology | 0.075 | ||||||
| SCC | 51 | 94.4 | 24 | 88.9 | 27 | 100.0 | |
| Adenocarcinoma | 3 | 5.6 | 3 | 11.1 | − | 7,27 | |
| FIGO stage | 0.295 | ||||||
| IB | 1 | 1.9 | − | − | 1 | 3.7 | |
| IIA | 2 | 3.7 | 1 | 3.7 | 1 | 3.7 | |
| IIB | 11 | 20.4 | 5 | 18.5 | 6 | 22.2 | |
| IIIA | 1 | 1.9 | − | − | 1 | 3.7 | |
| IIIB | 35 | 64.8 | 17 | 63.0 | 18 | 66.7 | |
| IVA | 4 | 7.4 | 4 | 14.8 | − | − | |
Abbreviations: FIGO, Fédération Internationale de Gynécologie et d'Obstétrique (International Federation of Gynecology and Obstetrics); SCC, squamous cell carcinoma.
Notes:p-value: Chi-squared test or the Fisher's exact test (significant p-value < 0.05); group 1: cisplatin; group 2: cisplatin and gemcitabine.
| Variables | n | Progression-Free survival | Overall survival | ||
|---|---|---|---|---|---|
| Hazard ratio (95%VI) | p-value | Hazard ratio (95%CI) | p-value | ||
| Age (years) | |||||
| ≤ 46 | 28 | Reference | Reference | ||
| > 46 | 26 | 1.331 | 0.350 | 1.398 | 0.278 |
|
| (0.731–2.422) | (0.763–2.565) | |||
| Histology | |||||
| SCC | 51 | Reference | Reference | ||
| Adenocarcinoma | 3 | 0.838 | 0.770 | 0.493 | 0.330 |
|
| (0.258–2.728) | (0.118–2.049) | |||
| FIGO Stage* | |||||
| IB-IIB | 14 | Reference | Reference | ||
| IIIA-IVA | 40 | 2.115 | 0.047 | 2.501 | 0.021 |
|
| (1.009–4.433) | (1.147–5.457) | |||
| Recidivism | |||||
| No | 44 | Reference | Reference | ||
| Yes | 10 | 3.141 | 0.003 | 1.410 | 0.363 |
|
| (1.487–6.636) | (0.672–2.958) | |||
| Treatment | |||||
| Group 1 | 27 | Reference | Reference | ||
| Group 2 | 27 | 0.496 | 0.027 | 0.544 | 0.055 |
|
| (0.266–0.924) | (0.291–1.014) | |||
Abbreviations: FIGO, Fédération Internationale de Gynécologie et d'Obstétrique (International Federation of Gynecology and Obstetrics); SCC, squamous cell carcinoma.
Notes:p-value: log-rank test (significant p-value < 0.05); group 1: cisplatin; group 2: cisplatin and gemcitabine.
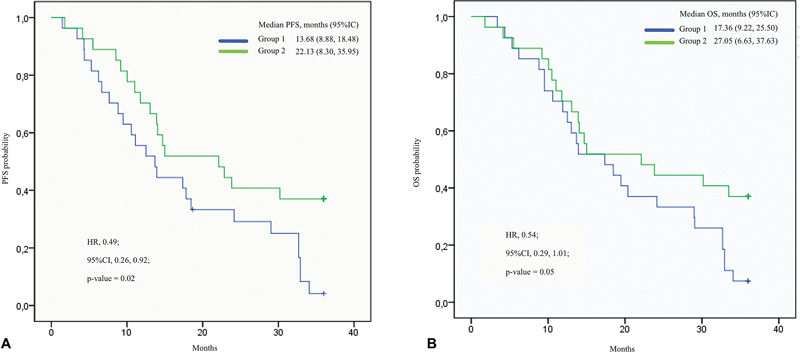
The median PFS in group 2 was of 22.13 months (95%CI: 8.30–35.95; p = 0.02), compared with 13.68 months (95%CI: 8.88–18.48; p = 0.02) in group 1. At 36 months, the PFS rate was of 37% in group 2, while in group 1, it was of 3.7%. The HR was of 0.49 (95%CI: 0.26–0.92; p = 0.02), indicating a 51% lower risk of disease progression or death in group 2 compared with group 1, with a statistically significant difference (
Fig. 1 Kaplan-Meyer model to estimate progression-free survival (PFS) (A) and overall survival (OS) (B) as a function of the chemotherapy protocol used in patients with cervical cancer in Acre between 2009 and 2016.
The median OS in group 2 was of 27.05 months (95%CI: 6.63–37.63; p = 0.051), compared with 17.36 months (95%CI: 9.22–25.50; p = 0.05) in group 1. At 36 months, the OS rate was of 37% in group 2 and of 7.4% in group 1. The HR was of 0.54 (95%CI: 0.29–1.01; p = 0.05), showing no statistically significant difference in OS between the groups. However, group 1 showed a lower survival curve than group 2, with a 54% lower risk of death, although this difference was numerical and not statistically significant (
The analysis of treatment-related toxicities (
| Toxicity | Group 1 | Group 2 | p-value | ||
|---|---|---|---|---|---|
| N = 27 | % | N = 27 | % | ||
| Hematologic | |||||
| Grade of anemia | |||||
| 1 | 8 | 29.6 | 10 | 37.0 | 0.08 |
| 2 | 14 | 51.9 | 17 | 63.0 | 0.02 |
| 3 | 4 | 14.8 | 6 | 22.2 | 0.04 |
| 4 | 1 | 3.7 | 2 | 7.4 | 0.12 |
| Grade of neutropenia | |||||
| 1 | 6 | 22.2 | 8 | 29.6 | 0.09 |
| 2 | 10 | 37.0 | 14 | 51.9 | 0.03 |
| 3 | 5 | 18.5 | 7 | 25.9 | 0.02 |
| 4 | 1 | 3.7 | 2 | 7.4 | 0.10 |
| Grade of thrombocytopenia | |||||
| 1 | 3 | 11.1 | 4 | 14.8 | 0.15 |
| 2 | 4 | 14.8 | 6 | 22.2 | 0.05 |
| 3 | 2 | 7.4 | 3 | 11.1 | 0.03 |
| 4 | 0 | 0 | 1 | 3.7 | 0.20 |
| Gastrointestinal | 6 | 22.2 | 7 | 25.9 | 0.072 |
| Genitourinary | 4 | 14.8 | 18 | 66.7 | 0.0005 |
| Peripheral neuropathy | 3 | 11.1 | 15 | 55.6 | 0.03 |
Notes: Group 1: cisplatin; group 2: cisplatin and gemcitabine; grade of hematological toxicities according to the Common Terminology Criteria for Adverse Events (CTCAE) Toxicity Classification, version 5.0; it was not possible to use this classification in the other toxicities due to the lack of standardization in the records; p-value: Pearson's Chi-squared test or Fisher's exact test, as applicable.
Regarding non-hematologic toxicities, genitourinary toxicity occurred more frequently in group 2 (66.7%) compared with group 1 (14.8%) (p = 0.0005). Peripheral neuropathy was significantly more frequent in group 2 as well (55.6% versus 11.1% in group 1; p = 0.03). No statistically significant differences were observed in terms of gastrointestinal toxicities between the groups (p > 0.05).
The current study evaluated the survival of patients with locally-advanced cervical cancer treated with concurrent CRT using cisplatin and gemcitabine (group 2) compared with cisplatin monotherapy (group 1). The findings demonstrate that the combined therapy reduces the risk of progression or death in PFS (HR: 0.49; 95%CI: 0.26–0.91; p = 0.02). However, although patients in group 2 showed a lower risk of death and longer survival curves, the difference in OS was not statistically significant (HR: 0.54; 95%CI: 0.29–1.01; p = 0.05).
These findings are consistent with those of previous studies, such as the one by Zarbá et al. (2003), a phase-I-II study that assessed the feasibility and efficacy of a weekly regimen with gemcitabine at 125 mg/m2 plus cisplatin 40 mg/m2 combined with EBRT for locally-advanced cervical cancer. Their results demonstrated that this combination was well tolerated, with manageable toxicity and an overall response rate of up to 86%.
Supporting these findings, the phase-III study by Dueñas-González et al.
Mell et al.
The high proportion of patients with advanced disease in the present study, particularly FIGO stage IIIB (64.8%), is consistent with data reported by Bhatla et al.
Another contributing factor is the quality of RT delivery in this cohort. All patients were treated with two-dimensional (2D) EBERT using a Co60 equipment, and three-dimensional (3D) conformal planning, but without image-guided radiotherapy (IGRT) or 3D brachytherapy. This limitation in RT technology may have negatively impacted local control and survival outcomes, as highlighted in previous studies.
Regarding treatment-related toxicities, the higher incidence of genitourinary toxicity in group 2 (p = 0.0005) may be attributed to the radiosensitizing effect of gemcitabine, which enhances the damage caused by RT to normal tissues, increasing the risk of radiation-induced cystitis and proctitis.
Hematologic toxicities were more prevalent in group 2, with a higher incidence of grade ≥ 2 anemia (p = 0.02) and grade ≥ 3 neutropenia (p = 0.03). These findings are consistent with those of studies
The demographic and clinical data of the patients in the present study, such as the predominance of SCC (94.4%) and the prevalence of FIGO stage IIIB (64.8%), are similar to those reported in the latest global statistics.
The methodological limitations to the current study include its retrospective design and the reliance on handwritten medical records, which introduced selection bias and data standardization issues. In particular, the limited sample size, of 54 patients, which was partly due to illegible documentation and missing data, hampered the robustness of the statistical analyses. Furthermore, the lack of standardized recording of non-hematologic toxicities restricted our evaluation of hematologic events, which were graded according to CTCAE version 5.0.
In conclusion, the findings of the current study suggest that the combination of cisplatin and gemcitabine may improve PFS in patients with locally-advanced cervical cancer. Importantly, this benefit was observed in a context of limited RT resources specifically, in a setting using two-dimensional 2D EBRT with a Co60 equipment and 3D conformal planning, but without IGRT or 3D brachytherapy. However, the impact on OS remains unclear, with borderline statistical significance and increased toxicity in the combination group. Further prospective, randomized studies are warranted to confirm these results, identify patient subgroups most likely to benefit, and optimize treatment protocols to improve both survival and quality of life.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Sung, H and Ferlay, J and Siegel, R L and Laversanne, M and Soerjomataram, I and Jemal, A and Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin [online]. 2021, vol. 71, p. 209-249. https://doi.org/10.3322/caac.21660 Ver referência
2. Relatório Anual [online]. Available from: <https://antigo.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//dados_e_numeros_colo_22marco2023.pdf>.
3. Bhatla, N and Berek, J S and Fredes, M C and Denny, L A and Grenman, S and Karunaratne, K. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet [online]. 2019, vol. 145, p. 129-135. https://doi.org/10.1002/ijgo.12749 Ver referência
4. Capítulo 1: Câncer de colo uterino. S.d [online]. Available from: <https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/seminario-radioterapia-capitulo-um-cancer-de-colo-uterino.pdf>.
5. Saleh, M and Virarkar, M and Javadi, S and Elsherif, S B and Faria, SdC and Bhosale, P. Cervical Cancer: 2018 Revised International Federation of Gynecology and Obstetrics Staging System and the Role of Imaging. AJR Am J Roentgenol [online]. 2020, vol. 214, p. 1182-1195. https://doi.org/10.2214/AJR.19.21819 Ver referência
6. Hill, E K. Updates in Cervical Cancer Treatment. Clin Obstet Gynecol [online]. 2020, vol. 63, p. 3-11. https://doi.org/10.1097/GRF.0000000000000507 Ver referência
7. ESMO Guidelines Committee. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol [online]. 2017, vol. 28, p. iv72-iv83. https://doi.org/10.1093/annonc/mdx220 Ver referência
8. NCCN Clinical Practice Guidelines in Oncology. Cervical Cancer - Version 4. 2024 [online]. Available from: <https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf>.
9. Sociedade Brasileira de Oncologia Clínica (SBOC). Cancer treatment guidelines - Cervix. SBOC Conduct Guide. 2023 [online]. Available from: <https://sboc.org.br/images/Diretrizes-2023/pdf/Diretrizes-SBOC-2023—Colo-do-utero-v20-FINAL.pdf>.
10. Peters, W A and Liu, P Y and Barrett, R J and Stock, R J and Monk, B J and Berek, J S. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J Clin Oncol [online]. 2000, vol. 18, p. 1606-1613. https://doi.org/10.1200/JCO.2000.18.8.1606 Ver referência
11. Neves, A P and Vargas, M D. Platinum (II) Complexes in Cancer Therapy. Rev Virtual Quim [online]. 2011, vol. 3, p. 196-209. https://doi.org/10.5935/1984-6835.20110023 Ver referência
12. Gupta, S and Maheshwari, A and Parab, P and Mahantshetty, U and Hawaldar, R and Chopra, S S. Neoadjuvant Chemotherapy Followed by Radical Surgery Versus Concomitant Chemotherapy and Radiotherapy in Patients With Stage IB2, IIA, or IIB Squamous Cervical Cancer: A Randomized Controlled Trial. J Clin Oncol [online]. 2018, vol. 36, p. 1548-1555.
13. Kim, Y S and Shin, S S and Nam, J H and Kim, Y-T and Kim, Y-M and Kim, J H and Choi, E K. Prospective randomized comparison of monthly fluorouracil and cisplatin versus weekly cisplatin concurrent with pelvic radiotherapy and high-dose rate brachytherapy for locally advanced cervical cancer. Gynecol Oncol [online]. 2008, vol. 108, p. 195-200. https://doi.org/10.1016/j.ygyno.2007.09.022 Ver referência
14. Costa, SCSd and Bonadio, R C and Gabrielli, F CG and Aranha, A S and Genta, M LND and Miranda, V C. Neoadjuvant Chemotherapy With Cisplatin and Gemcitabine Followed by Chemoradiation Versus Chemoradiation for Locally Advanced Cervical Cancer: A Randomized Phase II Trial. J Clin Oncol [online]. 2019, vol. 37, p. 3124-3131. https://doi.org/10.1200/JCO.19.00674 Ver referência
15. Dueňas-González, A and Orlando, M and Zhou, Y and Quinlivan, M and Barraclough, H. Efficacy in high burden locally advanced cervical cancer with concurrent gemcitabine and cisplatin chemoradiotherapy plus adjuvant gemcitabine and cisplatin: prognostic and predictive factors and the impact of disease stage on outcomes from a prospective randomized phase III trial. Gynecol Oncol [online]. 2012, vol. 126, p. 334-340. https://doi.org/10.1016/j.ygyno.2012.06.011 Ver referência
16. Hashemi, F A and Akbari, E H and Kalaghchi, B and Esmati, E. Concurrent chemoradiation with weekly gemcitabine and cisplatin for locally advanced cervical cancer. Asian Pac J Cancer Prev [online]. 2013, vol. 14, p. 5385-5389. https://doi.org/10.7314/apjcp.2013.14.9.5385 Ver referência
17. Li, F and Mei, F and Yin, S and Du, Y and Hu, L and Hong, W and Li, J. Improving the efficacy and safety of concurrent chemoradiotherapy by neoadjuvant chemotherapy: a randomized controlled study of locally advanced cervical cancer with a large tumor. J Gynecol Oncol [online]. 2024, vol. 35, p. e10. https://doi.org/10.3802/jgo.2024.35.e10 Ver referência
18. Mell, L K and Xu, R and Yashar, C M and McHale, M T and Einck, J P and Mayadev, J. Phase 1 Trial of Concurrent Gemcitabine and Cisplatin with Image Guided Intensity Modulated Radiation Therapy for Locoregionally Advanced Cervical Carcinoma. Int J Radiat Oncol Biol Phys [online]. 2020, vol. 107, p. 964-973. https://doi.org/10.1016/j.ijrobp.2020.04.019 Ver referência
19. Wang, C C and Chou, H H and Yang, L Y and Lin, H and Liou, W-S and Tseng, C-W. A randomized trial comparing concurrent chemoradiotherapy with single-agent cisplatin versus cisplatin plus gemcitabine in patients with advanced cervical cancer: An Asian Gynecologic Oncology Group study. Gynecol Oncol [online]. 2015, vol. 137, p. 462-467. https://doi.org/10.1016/j.ygyno.2015.03.046 Ver referência
20. GETICS (Grupo de Estudio, Tratamiento e Investigación del Cáncer del Sur) Argentina. A phase I-II study of weekly cisplatin and gemcitabine with concurrent radiotherapy in locally advanced cervical carcinoma. Ann Oncol [online]. 2003, vol. 14, p. 1285-1290. https://doi.org/10.1093/annonc/mdg345 Ver referência
21. Mini, E and Nobili, S and Caciagli, B and Landini, I and Mazzei, T. Cellular pharmacology of gemcitabine. Ann Oncol [online]. 2006, vol. 17, p. v7-v12.
22. U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE). Version 5.0. 2017 [online]. Available from: <https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5×7.pdf>.
23. Análise de sobrevida das pacientes portadoras de câncer de colo uterino localmente avançado, tratadas com radioquimioterapia definitiva com esquema cisplatina/gencitabina versus cisplatina semanal. [thesis (Master's in Sciences).]. São Paulo: Fundação Antônio Prudente; 2020 [online]. Available from: <https://accamargo.phlnet.com.br/MESTRADO/2020/FMAlencar/FMAlencar.pdf>.
Dados de acesso insuficientes para visualização no mapa.