Breast cancer (BC) is the most common neoplasm among women in Brazil and worldwide, excluding non-melanoma skin cancer.
It is essential to offer BC treatment in an adequate time since delays may decrease the chance of cure. A later diagnosis, with a more advanced disease, hinders the use of less aggressive treatments as less invasive axilla and breast surgeries, which may negatively impact patients' quality of life.
Time to first consultation in specialized BC centers depends on several factors including the country region, proximity to cities with healthcare services,
Identifying factors associated with starting oncological treatment after 60 days is essential to develop public policies towards most vulnerable patients. These actions could reduce barriers that prevent patients from having timely diagnosis and treatment. Therefore, the primary objective of this study was to assess whether low level of schooling is associated with the initiation of oncological treatment after 60 days.
This was a cross-sectional study including all female patients with BC between 2022 and 2023 registered in the Cancer Registry (CR) of Hospital de Clínicas de Porto Alegre (HCPA). All study participants received care through the SUS. Inclusion criteria required a histopathological diagnosis of invasive BC, with the first treatment occurring at HCPA in 2022 and 2023. Recurrence cases where the initial tumor was treated before 2022 and patients who did not receive antineoplastic treatment were excluded.
A sample size of 178 subjects was calculated based on retrospective data,
The project was approved by the HCPA Ethics in Research Committee under registration number 71160423.7.0000.5327 (CAAE). The study followed current guidelines and regulations on research involving human subjects, respecting bioethical principles such as autonomy and non-maleficence.
After identifying eligible patients, phone contact was made to invite them to participate in the study. Upon agreement, the informed consent form was read via phone and a questionnaire regarding sociodemographic characteristics and the patient's journey before the first consultation at HCPA was conducted. Additionally, an individual review of electronic medical records was performed.
The telephonic questionnaire was applied to all participants that answered the phone call from the research team. The questionnaire included questions regarding the date of suspicion and confirmation of BC as well as information related to family structure, ethnicity, marital status, and whether the participant had a paid employment at the time of diagnosis. The collected data was used exclusively for the analyses in this study, with precautions to minimize risks related to confidentiality as provided for in Resolution No. 466/2012 of the Brazilian National Health Council (Conselho Nacional de Saúde CNS). Prediagnosis data was obtained from the Health Department of the State of Rio Grande do Sul. Deceased participants, or those who did not answer the telephone call, as determined by the ethics committee, had their data obtained exclusively from electronic medical records.
Quantitative variables were described based on measures of central tendency and dispersion. Qualitative variables were described according to frequency and proportion. The variable time to first treatment was obtained from medical records or through direct contact with the patient. Considering the 60-day law, time to first treatment was dichotomized into “≤ 60 days” or “> 60 days” in order to establish associations with other variables. Prevalence ratio (PR), CIs, and significance values (p-values) were calculated to verify the relationship between time to treatment and variables of interest. Relative risk (RR) was estimated through the PR.
Univariate analyses were performed to correlate the time to first oncologic treatment with the participants' sociodemographic variables. Multivariable analysis was conducted using Poisson logistic regression, which is the most appropriate mathematical method for cross-sectional studies.
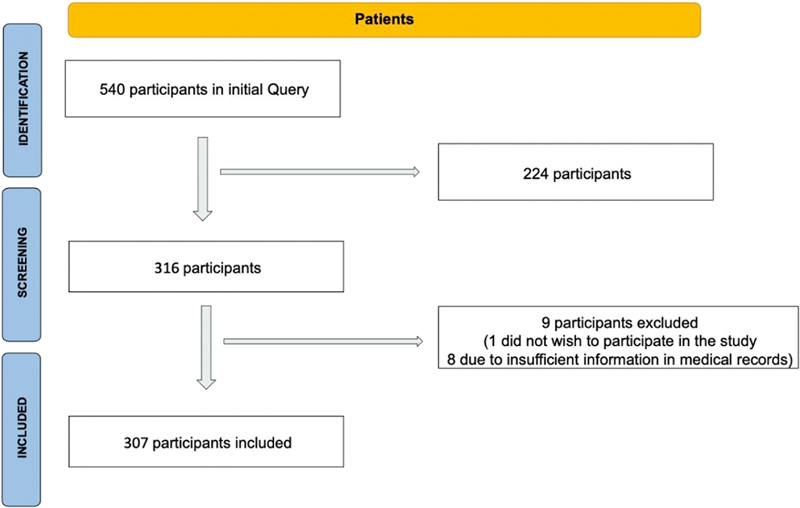
During the established period, 540 new patients were treated for BC at HCPA. Of these, 307 met the inclusion criteria and were included in the analysis (
Fig. 1 Inclusion of participants.
Prediagnosis data were available from 284 participants (92.25%) and were collected through the electronic system responsible for municipal consultation scheduling (GERCON). The median age was 63 (27–91) years; 20.20% of the patients were ≤ 49, 50.49% were 50 to 70, and 29.31% were > 70-years-old, with one missing value (0.32%).
Self-reported skin color was white in 80.46%, black in 10.75%, and pardo (mixed-race) in 8.47% of the participants, with one missing entry (0.32%). The data were collected by phone for 170 participants and from electronic records for the rest.
Regarding the level of schooling, 4.25% of the participants were illiterate, 38.23% had incomplete primary education, 13.73% had completed primary education, 5.23% had incomplete secondary education, 28.10% had completed secondary education, and 10.46% had higher education (
| Characteristic | n (%) |
|---|---|
| Age (median) | 63 years |
| Skin color/Ethnicity White Pardo Black Not identified |
247 (80.46) 26 (8.47) 33 (10.75) 1 (0.32) |
| Level of Schooling* Illiterate Incomplete primary education Complete primary education Incomplete secondary education Complete secondary education Higher education |
13 (4.25) 117 (38.23) 42 (13.73) 16 (5.23) 86 (28.10) 32 (10.46) |
| City of origin Porto Alegre (capital) Other cities in the state of Rio Grande do Sul |
115 (37.79) 192 (62.21) |
| Tumor subtype** Luminal A Luminal B Luminal-HER2 Triple-negative HER-2+ |
71 (23.36) 136 (44.74) 45 (14.80) 38 (12.5) 14 (4.6) |
| Clinical staging*** I II III IV |
84 (27.72) 126 (41.58) 64 (21.12) 29 (9.6) |
| Site of diagnosis* Hospital de Clínicas de Porto Alegre Other |
231 (75) 75 (25) |
Notes: *Missing data from one patient; **missing data from three patients; ***missing data from four patients.
The median time to initiate oncologic treatment, measured from the date of the anatomopathological (AP) examination result, was 47 (0–211) days. Furthermore, 90 participants (29.9%) exceeded 60 days to start their treatment.
To identify how the level of schooling influences the time to first treatment, a Poisson log-linear model with robust variance for multivariable analysis was used.
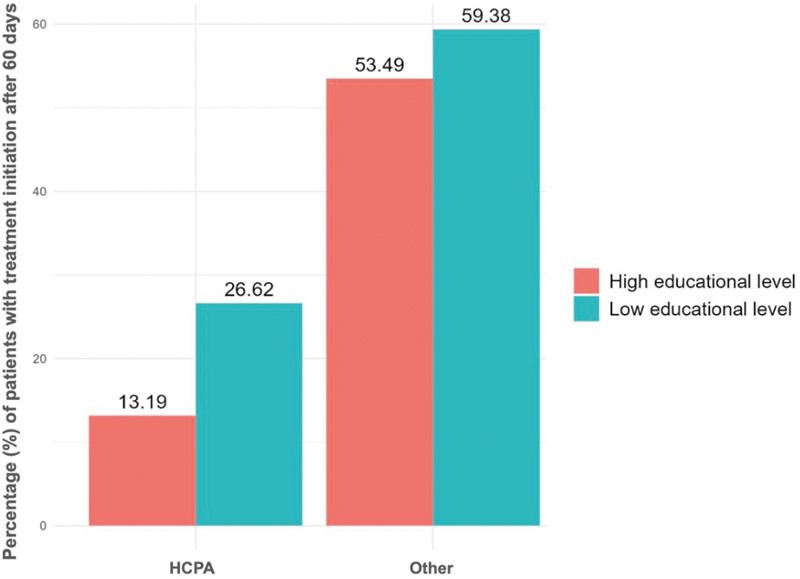
The multivariable model included all variables that modified the association effect by 10% or more. Among the variables tested, “biopsy location” was the only that met that criterion. Therefore, in this analysis model, level of schooling and biopsy location were included. We found that lower level of schooling led to a statistically significant 48% increased risk (RR = 1.48; 95%CI: 1.064–2.062) of delayed initiation of oncologic treatment beyond 60 days compared to participants with higher levels of schooling (
Fig. 2 Multivariable analyses regarding site of diagnostic biopsy and level of schooling.
As a secondary objective, univariable analyses were made evaluating the characteristics of participants that initiated their treatment within or after the established 60-days period (
| Parameter | Category | n (%) | Estimated relative risk | 95%CI | p-value |
|---|---|---|---|---|---|
| Age (years) | ≤ 49 | 64 (20.20) | 1 | − | − |
| 50–69 | 148 (50.49) | 0.713 | 0.430–1.184 | 0.191 | |
| ≥ 70 | 94 (29.31) | 0.968 | 0.634–1.477 | 0.879 | |
| Ethnicity | Other | 280 (91.50) | 1 | − | − |
| Pardo | 26 (8.50) | 1.636 | 1.038–2.579 | 0.034 | |
| Level of schooling | Low | 172 (56.00) | 1 | − | − |
| High | 134 (44.00) | 1.247 | 0.872–1.781 | 0.226 | |
| Site of initial biopsy | Hospital de Clínicas de Porto Alegre | 231 (75.00) | 1 | − | − |
| Other | 75 (25.00) | 2.640 | 1.918–3.633 | < 0.001 | |
| Clinical stage at diagnosis | I | 84 (27.7) | 1 | − | − |
| II | 126 (41.6) | 1.167 | 0.768–1.773 | 0.471 | |
| III | 64 (21.1) | 0.930 | 0.548–1.579 | 0.787 | |
| IV | 29 (9.6) | 0.845 | 0.408–1.750 | 0.650 |
Note: For the level of schooling, patients were divided into two groups: low (illiterate or with incomplete/complete primary education) or high (incomplete/complete secondary education or higher education).
There was a significantly higher risk of delayed treatment among those who underwent biopsy outside of HCPA compared to those who had the procedure performed within the institution, with a RR of 2.64 (95%CI = 1.918–3.633). Age, ethnicity, clinical stage, city of origin, modality of first oncological treatment, and having a relationship at the time of diagnosis did not show significant differences.
Regarding the modality of the first oncologic treatment, 168 participants started with surgery, with a median time of 44 days from diagnosis. In contrast, 101 participants began with chemotherapy with a median time of 51 days. For the subgroup of 32 participants who started with hormone therapy, the median time was 31.5 days. Finally, 5 patients started treatment with radiotherapy and data from 1 patient could not be obtained.
Because the referral time to the first cancer specialist consultation after diagnosis made at the primary health care level can be long, a sensitivity analysis was conducted including 231 participants (75%) that underwent their tumor biopsy at HCPA. Of these, 79.2% (n = 183) had their treatment begun within 60 days from diagnosis, with a median time of 42 days and mean of 45.7 (0–150) days. The influence of sociodemographic factors in this sample was also evaluated, and lower level of schooling remained a risk factor for starting treatment after 60 days, with an RR of 2.019 (95 CI: 1.113–3.660).
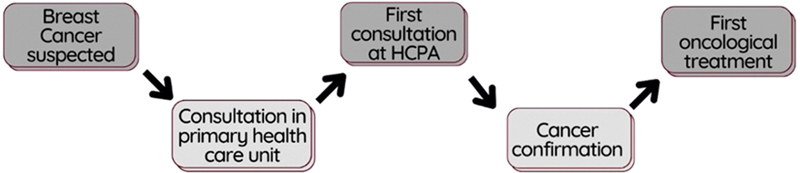
The questionnaire applied to participants was analyzed to describe their prediagnostic pathway to care at HCPA (
Fig. 3 Diagnostic pathway of participants.
Although the 60-days law determines that the AP result is the necessary exam to initiate oncological treatment, it is well established that the immunohistochemistry (IHC) test is currently essential to determine the most appropriate first-line treatment modality for BC.
In this sample, the median time for the IHC result was 16 (0–95) days from the date of the AP report. Among patients who underwent a biopsy at HCPA, this time was shorter, with a median of 7 (0–68) days.
The treatment of early-stage BC is initially conducted through four main modalities: chemotherapy, surgery, hormone therapy or radiotherapy. The decision regarding the sequence of these treatments should be made within a multidisciplinary team involving specialists from different fields.
Delays between diagnosis and surgery significantly affect survival.
Regarding time to initiation of chemotherapy, studies have indicated that starting this therapy within 45 days of diagnosis improves survival outcomes.
Evidence on the time required to obtain a confirmed BC diagnosis remains limited. During the prediagnostic period, multiple barriers hinder timely access to diagnostic centers, resulting in delayed care. The diagnostic process typically begins when a woman detects a breast abnormality or has an abnormal screening mammogram and seeks evaluation at a primary health center. Under Brazilian Law No. 13,896/2019), when malignancy is suspected, diagnostic tests must be completed within 30 days.
In the present study, both low level of schooling and pardo skin color had a significant impact in time to treatment initiation, leading to prolonged delays. This association remained significant even when analyzing only participants who received their diagnosis at HCPA indicating that social factors are determinants in the variable time to treatment initiation as previously described.
The long prediagnostic process also helps explain delays among patients whose diagnoses were confirmed outside HCPA. In this sample, 25% underwent biopsy before their UBS visit and thus already had a BC diagnosis at that consultation. Despite having a confirmed AP result, these patients must follow the same pathway as those without a diagnosis, including waiting for a UBS appointment and GERCON referral. Consequently, they face greater risk of delayed treatment initiation because, under the 60-day law, the countdown begins at diagnosis confirmation. Yet the SUS referral system does not prioritize these patients, which represents a weakness in the process.
Regarding the study's limitations, it is important to note that, as a cross-sectional study conducted at a single institution, caution should be taken when generalizing the reported findings, despite their alignment with the reviewed literature. While some variables showed an impact on the number of days to initiate oncological treatment, this difference did not reach statistical significance, which may reflect the limited sample size. Finally, it is worth emphasizing that, unlike studies based on cancer registry data from public institutions (which are often imprecise), the current study was conducted through an individual review of electronic medical records and, when possible, direct contact with the participants. This approach enhances the accuracy of the reported results.
The study was capable of identifying a large proportion of patients (70.01%) that began treatment within 60 days from diagnosis. When considering only those who underwent biopsy at HCPA, the percentage increased to 79.2%, which is significantly higher than the national average. Between 2016 and 2018, only 55.1% of BC patients in Brazil started treatment within 60 days.
This study identified the groups most vulnerable to treatment delays—patients with low level of schooling and pardo skin color—highlighting the need for individualized monitoring to reduce disparities. Implementing patient navigation programs may help address this inequity by guiding patients and families from the prediagnostic phase to treatment initiation. Law No. 14,758 incorporates this strategy into the National Cancer Prevention and Control Policy within the SUS, and evidence shows that patient navigators reduce both time to BC diagnosis
The treatment of BC is complex and depends on coordinated actions across healthcare services to ensure timely therapy. This study showed that low level of schooling is a significant risk factor for delayed treatment initiation, even among patients biopsied at the same institution where treatment began. Patients with pardo skin color were also associated with delays, although this finding requires further investigation due to the small sample size.
In relation to the 60-day law, identifying socially vulnerable groups is crucial to preventing treatment delays. The study also examined the prediagnostic period—an understudied topic in Brazilian guidelines—and found a median of 94 days from suspicion to diagnosis, exceeding the legally defined timeframe. Targeted government measures are needed, including the use of nurse navigators, which have proven effective in reducing time to treatment, and public educational initiatives to raise awareness of cancer warning signs and reduce prediagnostic delays.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Instituto Nacional de Câncer (INCA). Estimativa 2023: incidência de câncer no Brasil. INCA, 2022.
2. Souza, C B and Fustinoni, S M and Amorim, M HC and Zandonade, E and Matos, J C and Schirmer, J. Breast cancer: diagnosis-to-treatment waiting times for elderly women at a reference hospital of São Paulo, Brazil. Ciênc Saúde Colet [online]. 2015, vol. 20, p. 3805-3816. https://doi.org/10.1590/1413-812320152012.00422015 Ver referência
3. Costa, J B and Lima, MAGd and Neves, RdF. O retorno ao trabalho de mulheres após a experiência do câncer de mama: uma metassíntese. Rev Bras Saude Ocup [online]. 2020, vol. 45, p. e19. https://doi.org/10.1590/2317-6369000045018 Ver referência
4. Ng, E T and Ang, R Z and Tran, B X. Comparing Quality of Life in Breast Cancer Patients Who Underwent Mastectomy Versus Breast-Conserving Surgery: A Meta-Analysis. Int J Environ Res Public Health [online]. 2019, vol. 16, p. 4970. https://doi.org/10.3390/ijerph16244970 Ver referência
5. Abdel-Razeq, H and Mansour, A and Edaily, S and Dayyat, A. Delays in Initiating Anti-Cancer Therapy for Early-Stage Breast Cancer-How Slow Can We Go?. J Clin Med [online]. 2023, vol. 12, p. 4502. https://doi.org/10.3390/jcm12134502 Ver referência
6. Brazil. Presidência da República. Lei no 12.732, de 22 de novembro de 2012. Dispõe sobre o primeiro tratamento de paciente com neoplasia maligna comprovada e estabelece prazo para seu início. Diário Oficial da União, 2012.
7. Jomar, R T and Velasco, N S and Mendes, G LQ and Guimarães, R M and Fonseca, V AO and Meira, K C. Factors associated with time-to-treatment initiation of breast cancer. Cien Saude Colet [online]. 2023, vol. 28, p. 2155-2164.
8. Nogueira, M C and Atty, A TM and Tomazelli, J and Jardim, B C and Bustamante-Teixeira, M T and Silva, G AE. Frequency and factors associated with delay in breast cancer treatment in Brazil, according to data from the Oncology Panel, 2019-2020. Epidemiol Serv Saude [online]. 2023, vol. 32, p. e2022563. https://doi.org/10.1590/S2237-96222023000300004 Ver referência
9. Maschmann, R M and Jesus, RGd and Werutsky, G. Time interval between diagnosis to treatment of breast cancer and the impact of health insurance coverage: a sub analysis of the AMAZONA III Study (GBECAM 0115). Breast Cancer Res Treat [online]. 2023, vol. 198, p. 123-130. https://doi.org/10.1007/s10549-022-06809-8 Ver referência
10. Cabral, A LLV and Giatti, L and Casale, C and Cherchiglia, M L. Social vulnerability and breast cancer: differentials in the interval between diagnosis and treatment of women with different sociodemographic profiles. Ciênc Saúde Colet [online]. 2019, vol. 24, p. 613-622. https://doi.org/10.1590/1413-81232018242.31672016 Ver referência
11. Borges, R B and Mancuso, A CB and Camey, S A. Power and Sample Size for Health Researchers: uma ferramenta para cálculo de tamanho amostral e poder do teste voltado a pesquisadores da área da saúde. Clin Biomed Res [online]. 2020, vol. 40, p. 247-253. https://doi.org/10.22491/2357-9730.109542 Ver referência
12. Barros, A J and Hirakata, V N. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol [online]. 2003, vol. 3, p. 21. https://doi.org/10.1186/1471-2288-3-21 Ver referência
13. Waks, A G and Winer, E P. Breast Cancer Treatment: A Review. JAMA [online]. 2019, vol. 321, p. 288-300. https://doi.org/10.1001/jama.2018.19323 Ver referência
14. Richards, M A and Westcombe, A M and Love, S B and Littlejohns, P and Ramirez, A J. Influence of delay on survival in patients with breast cancer: a systematic review. [online]. , vol. 353, p. 1119-1126.
15. An, D and Choi, J and Lee, J. Time to surgery and survival in breast cancer. BMC Surg [online]. 2022, vol. 22, p. 388. https://doi.org/10.1186/s12893-022-01835-1 Ver referência
16. Ho, P J and Cook, A R and Ri, N KBM and Liu, J and Li, J and Hartman, M. Impact of delayed treatment in women diagnosed with breast cancer: A population-based study. Cancer Med [online]. 2020, vol. 9, p. 2435-2444. https://doi.org/10.1002/cam4.2830 Ver referência
17. Flores-Balcázar, C H and Flores-Luna, M L and Villarreal-Garza, C M and Bargalló-Rocha, J E. Provider delay in treatment initiation and its influence on survival outcomes in women with operable breast cancer. Rep Pract Oncol Radiother [online]. 2020, vol. 25, p. 271-275. https://doi.org/10.1016/j.rpor.2020.02.002 Ver referência
18. Brazil. Presidência da República. Lei no 13.896, de 30 de outubro de 2019. Altera a Lei n° 12.732, de 22 de novembro de 2012, para que os exames relacionados ao diagnóstico de neoplasia maligna sejam realizados no prazo de 30 (trinta) dias, no caso em que especifica [Internet]. Diário Oficial da União, 2019.
19. Barros, A F and Murta-Nascimento, C and Abdon, C H and Nogueira, D N and Lopes, E LC and Dias, A. Factors associated with time interval between the onset of symptoms and first medical visit in women with breast cancer. Cad Saude Publica [online]. 2020, vol. 36, p. e00011919. https://doi.org/10.1590/0102-311X00011919 Ver referência
20. Rivera-Franco, M M and Leon-Rodriguez, E. Delays in Breast Cancer Detection and Treatment in Developing Countries. Breast Cancer (Auckl) [online]. 2018, vol. 12, p. 1178223417752677. https://doi.org/10.1177/1178223417752677 Ver referência
21. Sousa, S MMT and Carvalho, MdGFdM and Santos, L A and Mariano, S BC. Acesso ao tratamento da mulher com câncer de mama. Saúde Debate [online]. 2019, vol. 43, p. 727-741. https://doi.org/10.1590/0103-1104201912206 Ver referência
22. Palmieri, F M and DePeri, E R and Mincey, B A. Comprehensive diagnostic program for medically underserved women with abnormal breast screening evaluations in an urban population. Mayo Clin Proc [online]. 2009, vol. 84, p. 317-322.
23. Zibrik, K and Laskin, J and Ho, C. Integration of a nurse navigator into the triage process for patients with non-small-cell lung cancer: creating systematic improvements in patient care. Curr Oncol [online]. 2016, vol. 23, p. e280-e283. https://doi.org/10.3747/co.23.2954 Ver referência
Dados de acesso insuficientes para visualização no mapa.