Gastric cancer (GC) is a heterogeneous disease characterized by high recurrence rates and unfavorable prognosis, ranking fifth in both incidence and cancer-related deaths worldwide.
Precision medicine was recently developed; it is innovative for this neoplasm, and it aims to adjust the clinical decision to the specific characteristics of individuals, such as the person's genetic characteristics and/or the genetic profile of the tumor. In the past few decades, the management of advanced GC has evolved largely due to therapeutic development tailored to actionable molecular abnormalities. A significant progress in the efficacy of systemic therapy has been observed with the clinical applicability of precision medicine (
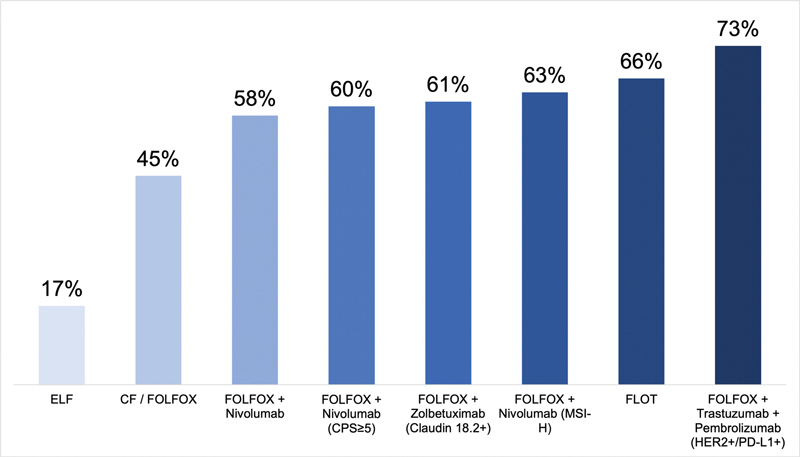
Fig. 1 Overall response rates of the therapeutic regimens used in advanced gastric cancer. Abbreviations: ELF, etoposide, leucovorin, 5-fluorouracil; CF, cisplatin, 5-fluorouracil; FOLFOX, 5-fluorouracil and leucovorin combined with oxaliplatin; CPS, combined positive score; MSI-H, high-frequency microsatellite instability; FLOT, 5-fluorouracil, leucovorin, oxaliplatin, docetaxel; HER2, human epidermal receptor 2; PD-L1, programmed cell death-ligand 1.
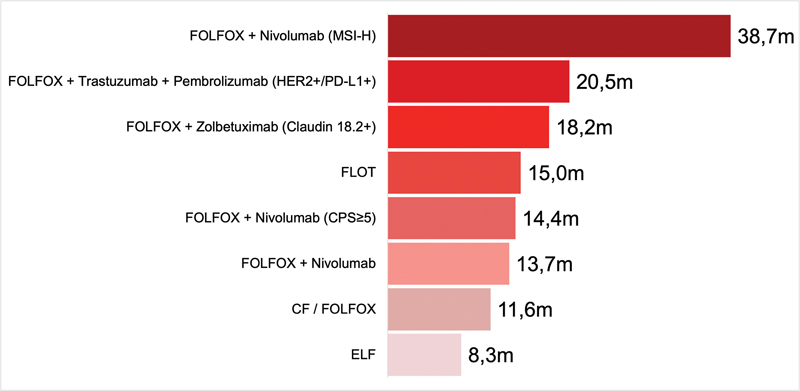
Fig. 2 Overall survival associated with the therapeutic regimens used in advanced gastric cancer. Abbreviations: ELF, etoposide, leucovorin, 5-fluorouracil; CF, cisplatin, 5-fluorouracil; FOLFOX, 5-fluorouracil and leucovorin combined with oxaliplatin; CPS, combined positive score; MSI-H, high-frequency microsatellite instability; FLOT, 5-fluorouracil, leucovorin, oxaliplatin, docetaxel; HER2, human epidermal receptor 2; PD-L1, programmed cell death-ligand 1.
Advanced GC portends a dismal prognosis, and the first therapeutic regimens used in the systemic therapy of the disease were characterized by poor efficacy and high toxicity.
We searched for articles in the PubMed database using the following search strategy and Medical Subject Headings (MeSH): gastric cancer AND treatment AND molecular AND precision medicine. The latest publications and meeting proceedings related to the topic were also reviewed.
A new classification based on the main molecular abnormalities was recently proposed by The Cancer Genome Atlas (TCGA) project
| Molecular subtype | Frequency | Characteristics |
|---|---|---|
| Chromosomal instability (CIN) | 50% | • The incidence is increased in esophagogastric tumors; • Usually present intestinal-type histology; • TP53 mutations, and HER2 and KRAS amplifications. |
| High-frequency microsatellite instability (MSI-H) | 22% | • The incidence is higher in elderly patients; • Characterized by a high tumor mutational burden; • Frequent silencing of MLH1. |
| Genomically stable (GS) | 20% | • Typically diagnosed at an earlier age; • Diffuse-type histology usually present; • Tends to be located at the distal portions of the stomach; • CDH1, ARID1A, and RHOA mutations. |
| Epstein-Barr virus (EBV) | 9% | • Frequently located at the fundus and gastric body; • Lower rate of nodal metastases; • Better survival rates; • PIK3CA mutations and silencing of the CDKN2A promoter. |
In the current clinical practice, the molecular evaluation of GC must involve the test for overexpression/amplification of the human epidermal growth factor receptor 2 (HER2), high-frequency microsatellite instability (MSI-H), programmed cell death-ligand 1 (PD-L1) expression, and, more recently, claudin 18.2 expression. Such findings influence the decision-making process and therapy for metastatic disease.
Approximately 10 to 20% of GCs present amplification of the HER2 gene, which results in the overexpression of HER2, a receptor tyrosine kinase member of the epidermal growth factor receptor (EGFR) family commonly found in the chromosomal-instability subtype.
Expression of PD-L1 and deficient DNA mismatch repair (dMMR) mechanism are also important predictive biomarkers in GC.
The standard of care for unresectable locally-advanced or metastatic GC is the combination of fluoropyrimidines and platins. The addition of monoclonal antibodies will be based on the expression of biomarkers in the tumor tissue.
Expression of PD-L1 may be measured by the number of PD-L1-stained tumor cells divided by the total number of viable tumor cells and multiplied by 100, which is called tumor proportion score (TPS), or as the total number of lymphocytes, macrophages, and PD-L1-stained tumor cells divided by the total number of viable tumor cells and multiplied by 100, which is called combined positive score (CPS).
Pembrolizumab associated with oxaliplatin-based chemotherapy is another initial treatment option. In the phase-III KEYNOTE-859 study, with 1,579 HER2-negative patients, the addition of pembrolizumab to chemotherapy improved the median OS (12.9 months versus 11.5 months; HR: 0.78; 95%CI: 0.70–0.87) and PFS (6.9 months versus 5.6 months; HR: 0.76; 95%CI: 0.67–0.85) compared to the arm which received placebo associated with chemotherapy.
The addition of trastuzumab to chemotherapy is considered in patients with HER2-positive tumors, which are defined by 3+ immunohistochemistry (IHC) staining or 2+ and positive fluorescent in-situ hybridization (FISH). The addition of pembrolizumab to trastuzumab is also suggested, based on the phase-III KEYNOTE-811 study.
The benefit of trastuzumab in advanced HER2-positive GC was addressed in the phase-III ToGA trial,
The efficacy and safety of trastuzumab deruxtecan (T-Dxd), an antibody-drug conjugate, were evaluated in patients with HER2-positive GC whose disease progressed after the initial trastuzumab-based therapy.
Regarding bispecific antibodies, zanidatamab, which targets 2 distinct HER2 epitopes, was evaluated in a phase-I study,
| Clinical setting | Study number (and/or name) | Intervention/Treatment |
|---|---|---|
| | ||
| First line | NCT05152147 (HERIZON-GEA-01) | Trastuzumab, zanidatamab, tislelizumab, chemotherapy |
| Second line | NCT05427383 | KN026, chemotherapy |
| Second line | NCT05002127 (ASPEN-06) | Evorpacept (ALX148), trastuzumab, ramucirumab, chemotherapy |
| Second line | NCT04704934 (DESTINY-Gastric04) | Trastuzumab deruxtecan, ramucirumab, chemotherapy |
| | ||
| First line | NCT05919381 | Gentuximab, chemotherapy |
| Second line | NCT03081143 (RAMIRIS) | Ramucirumab, chemotherapy |
| Third line | NCT04879368 (INTEGRATE IIb) | Regorafenib, nivolumab, chemotherapy |
| | ||
| First line | NCT05052801 (FORTITUDE-101) | Bemarituzumab, chemotherapy |
| First line | NCT05111626 (FORTITUDE-102) | Bemarituzumab, nivolumab, chemotherapy |
| | ||
| First line | NCT05918094 | Sintilimab, chemotherapy |
| First line | NCT05008783 | AK104, chemotherapy |
| First line | NCT05677490 | Nivolumab, chemotherapy |
| First line | NCT05568095 (STAR-221) | Domvanalimab, zimberelimab, nivolumab, chemotherapy |
| | ||
| First line | NCT03801668 | Chemotherapy (albumin-bound paclitaxel, oxaliplatin, S-1) |
Abbreviations: FGFR2, fibroblast growth factor receptor 2; HER2, human epidermal receptor 2; NCT, National Clinical Trial; PD-1, programmed cell death-1; PD-L1, programmed cell death-ligand 1; VEGFR, vascular endothelial growth factor receptor.
In cases of dMMR/MSI-H GEA identified through immunohistochemistry, it is highly recommended that the patients receive immune checkpoint inhibition. The greater benefit of the combination therapy was suggested in a subgroup analysis of the CheckMate 649 trial,
As with the first-line therapy, the second-line therapy also aims to control symptoms and increase survival. For patients with dMMR/MSI-H GEA, pembrolizumab remains as an option if it has not been administered as the first-line therapy. It has been subsequently established
Between 5% and 19% of gastric adenocarcinomas have high levels of TMB, which represents the number of mutations per megabase (mut/Mb) harbored by tumor cells.
New diagnostic techniques have contributed to the characterization of the genetic profile of GC and to the identification of new potential molecular targets. Claudin 18.2, a component of intercellular junctions, is commonly expressed in multiple cancers, including GC, and is not expressed in any healthy tissues, apart from the gastric mucosa. Zolbetuximab, an experimental monoclonal antibody that targets claudin 18.2, was evaluated in combination with oxaliplatin-based chemotherapy in the SPOTLIGHT
Inhibition of the vascular endothelial growth factor (VEGF) receptor (VEGFR) reduces tumor growth and vascularization.
Ramucirumab is a recombinant monoclonal antibody that binds to VEGF receptor 2 (VEGFR2), blocking receptor activation. At least two trials, REGARD
Different types of agents targeting fibroblast growth factor receptors (FGFRs) have been explored, however, without robust clinical evidence. Bemarituzumab has shown some promising results as the first-line treatment for metastatic GC. The phase-II FIGHT study
Activation of the MET proto-oncogene pathway is associated with tumor invasiveness and poor disease prognosis. The anti-MET monoclonal antibody onartuzumab was studied in combination with FOLFOX versus placebo plus FOLFOX in metastatic HER2-negative GEA patients, and the addition of anti-MET did not improve the outcomes in the general population or in MET-positive patients identified by through immunohistochemistry.
The phase-III STAR-221 trial
Neurotrophic tropomyosin-related kinase (NTRK) gene fusions (NTRK1, NTRK2, and NTRK3) lead to the expression of constitutively-active chimeric tropomyosin receptor kinase (TRK) proteins (TRKA, TRKB, and TRKC), which act as potential oncogenic drivers across various types of tumors. In GC, NTRK fusions are exceedingly rare, but they may indicate an aggressive phenotype. Larotrectinib and entrectinib, both TRK inhibitors, have shown remarkable efficacy against NTRK fusion-positive tumors, regardless of tumor type (“tumor-agnostic”).
Substantial advances have been made in the treatment of GC; however, more research is needed to optimize treatment strategies. For patients with gastric adenocarcinoma who do not overexpress HER2 and are not candidates for immunotherapy (CPS < 5–low or absent PD-L1 expression), the choice should be a dual classic combination containing platinum and fluoropyrimidine (such as FOLFOX or CapOX).
Phase-III studies on second-line metastatic therapy showed that paclitaxel, docetaxel, and irinotecan increase OS in relation to clinical support, with similar results. One of these studies
The combination of trifluridine and tipiracil hydrochloride forms TAS-102, an oral agent that is an option for third-line or subsequent therapy in patients who maintain good performance status after undergoing treatment with two or more agents. The effectiveness of the regimen was suggested in the TAGS trial.
Gastric cancer is a markedly heterogeneous disease whose epidemiological, histological and molecular characteristics must be comprehensively understood for a successful therapeutic development. Novel therapeutic targets have been identified in the past few years, with several ongoing studies evaluating targeted therapies (
Precision medicine has gradually evolved, following advances in genomics, molecular biology and diagnostic technologies. It aims to offer more efficient and personalized treatment for patients, seeking to identify the therapeutic target and perform prognostic and predictive stratifications to achieve better survival results with minimal toxicity.
The fact that GC presents genetic variations among different patients and/or in the same patient during the course of the disease should drive investigations into the molecular characteristics present in the tumor tissue and evaluations of the use of circulating biomarkers to predict and monitor disease progression, as well as the response to treatment. Targeted therapies are considered one of the key points in new effective antitumor drug development, and they should be available to patient subgroups that could benefit from them.
Despite the advances in personalized medicine, Brazil still has many obstacles to the application of personalized treatment, such as difficulty in accessing laboratory tests and medications, as well as poor infrastructure. In summary, we expected that extensive research combined with clinical trials will lead to advances in the diagnosis and treatment of such a complex disease, hopefully, with significant improvements in the access of the population to the innovations that aim to increase survival and improve quality of life with minimal toxicity burden.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Bray, F and Laversanne, M and Sung, H. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin [online]. 2024, vol. 74, p. 229-263. https://doi.org/10.3322/caac.21834 Ver referência
2. Rev Bras Cancerol ;69(1) [online]. Available from: <>.
3. ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol [online]. 2022, vol. 33, p. 1005-1020.
4. Murad, A M and Santiago, F F and Petroianu, A and Rocha, P R and Rodrigues, M A and Rausch, M. Modified therapy with 5-fluorouracil, doxorubicin, and methotrexate in advanced gastric cancer. Cancer [online]. 1993, vol. 72, p. 37-41. https://doi.org/10.1002/1097-0142(19930701)72:13.0.co;2-p Ver referência
5. Moehler, M and Eimermacher, A and Siebler, J. Randomised phase II evaluation of irinotecan plus high-dose 5-fluorouracil and leucovorin (ILF) vs 5-fluorouracil, leucovorin, and etoposide (ELF) in untreated metastatic gastric cancer. Br J Cancer [online]. 2005, vol. 92, p. 2122-2128. https://doi.org/10.1038/sj.bjc.6602649 Ver referência
6. Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature [online]. 2014, vol. 513, p. 202-209. https://doi.org/10.1038/nature13480 Ver referência
7. ToGA Trial Investigators. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet [online]. 2010, vol. 376, p. 687-697.
8. Janjigian, Y Y and Shitara, K and Moehler, M. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet [online]. 2021, vol. 398, p. 27-40.
9. KEYNOTE-859 investigators. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for HER2-negative advanced gastric cancer (KEYNOTE-859): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol [online]. 2023, vol. 24, p. 1181-1195. https://doi.org/10.1016/S1470-2045(23)00515-6 Ver referência
10. Marabelle, A and Le, D T and Ascierto, P A. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J Clin Oncol [online]. 2020, vol. 38, p. 1-10. https://doi.org/10.1200/JCO.19.02105 Ver referência
11. CheckMate 648 Trial Investigators. Nivolumab Combination Therapy in Advanced Esophageal Squamous-Cell Carcinoma. N Engl J Med [online]. 2022, vol. 386, p. 449-462. https://doi.org/10.1056/NEJMoa2111380 Ver referência
12. Shah, M A and Kennedy, E B and Alarcon-Rozas, A E. Immunotherapy and Targeted Therapy for Advanced Gastroesophageal Cancer: ASCO Guideline. J Clin Oncol [online]. 2023, vol. 41, p. 1470-1491. https://doi.org/10.1200/JCO.22.02331 Ver referência
13. Shitara, K and Van Cutsem, E and Bang, Y-J. Efficacy and safety of pembrolizumab or pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric cancer: the KEYNOTE-062 phase 3 randomized clinical trial. JAMA Oncol [online]. 2020, vol. 6, p. 1571-1580.
14. Janjigian, Y Y and Kawazoe, A and Yañez, P. The KEYNOTE-811 trial of dual PD-1 and HER2 blockade in HER2-positive gastric cancer. Nature [online]. 2021, vol. 600, p. 727-730. https://doi.org/10.1038/s41586-021-04161-3 Ver referência
15. DESTINY-Gastric01 Investigators. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Gastric Cancer. N Engl J Med [online]. 2020, vol. 382, p. 2419-2430. https://doi.org/10.1056/NEJMoa2004413 Ver referência
16. Van Cutsem, E and di Bartolomeo, M and Smyth, E. Trastuzumab deruxtecan in patients in the USA and Europe with HER2-positive advanced gastric or gastroesophageal junction cancer with disease progression on or after a trastuzumab-containing regimen (DESTINY-Gastric02): primary and updated analyses from a single-arm, phase 2 study. Lancet Oncol [online]. 2023, vol. 24, p. 744-756. https://doi.org/10.1016/S1470-2045(23)00215-2 Ver referência
17. Meric-Bernstam, F and Hamilton, E P and Beeram, M. Zanidatamab (ZW25) in HER2-expressing gastroesophageal adenocarcinoma (GEA): Results from a phase I study. J Clin Oncol [online]. 2021, vol. 39, p. 164.
18. Elimova, E and Ajani, J A and Burris, H A. Zanidatamab+ chemotherapy as first-line treatment for HER2-expressing metastatic gastroesophageal adenocarcinoma (mGEA). American Society of Clinical Oncology, 2023.
19. Shitara, K and Lordick, F and Bang, Y-J. Zolbetuximab plus mFOLFOX6 in patients with CLDN18.2-positive, HER2-negative, untreated, locally advanced unresectable or metastatic gastric or gastro-oesophageal junction adenocarcinoma (SPOTLIGHT): a multicentre, randomised, double-blind, phase 3 trial. Lancet [online]. 2023, vol. 401, p. 1655-1668.
20. Shah, M A and Shitara, K and Ajani, J A. Zolbetuximab plus CAPOX in CLDN18.2-positive gastric or gastroesophageal junction adenocarcinoma: the randomized, phase 3 GLOW trial. Nat Med [online]. 2023, vol. 29, p. 2133-2141.
21. Lieto, E and Ferraraccio, F and Orditura, M. Expression of vascular endothelial growth factor (VEGF) and epidermal growth factor receptor (EGFR) is an independent prognostic indicator of worse outcome in gastric cancer patients. Ann Surg Oncol [online]. 2008, vol. 15, p. 69-79. https://doi.org/10.1245/s10434-007-9596-0 Ver referência
22. Ohtsu, A and Shah, M A and Van Cutsem, E. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: a randomized, double-blind, placebo-controlled phase III study. J Clin Oncol [online]. 2011, vol. 29, p. 3968-3976. https://doi.org/10.1200/JCO.2011.36.2236 Ver referência
23. REGARD Trial Investigators. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet [online]. 2014, vol. 383, p. 31-39. https://doi.org/10.1016/S0140-6736(13)61719-5 Ver referência
24. RAINBOW Study Group. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol [online]. 2014, vol. 15, p. 1224-1235. https://doi.org/10.1016/S1470-2045(14)70420-6 Ver referência
25. Lorenzen, S and Thuss-Patience, P and Pauligk, C. FOLFIRI plus ramucirumab versus paclitaxel plus ramucirumab as second-line therapy for patients with advanced or metastatic gastroesophageal adenocarcinoma with or without prior docetaxel - results from the phase II RAMIRIS Study of the German Gastric Cancer Study Group at AIO. Eur J Cancer [online]. 2022, vol. 165, p. 48-57.
26. Pavlakis, N and Shitara, K and Sjoquist, K M. INTEGRATE IIa: A randomised, double-blind, phase III study of regorafenib versus placebo in refractory advanced gastro-oesophageal cancer (AGOC)—A study led by the Australasian Gastro-intestinal Trials Group (AGITG). American Society of Clinical Oncology, 2023.
27. Wainberg, Z A and Enzinger, P C and Kang, Y-K. Bemarituzumab in patients with FGFR2b-selected gastric or gastro-oesophageal junction adenocarcinoma (FIGHT): a randomised, double-blind, placebo-controlled, phase 2 study. Lancet Oncol [online]. 2022, vol. 23, p. 1430-1440.
28. Shah, M A and Cho, J-Y and Tan, I B. A randomized phase II study of FOLFOX with or without the MET inhibitor onartuzumab in advanced adenocarcinoma of the stomach and gastroesophageal junction. Oncologist [online]. 2016, vol. 21, p. 1085-1090.
29. Iveson, T and Donehower, R C and Davidenko, I. Rilotumumab in combination with epirubicin, cisplatin, and capecitabine as first-line treatment for gastric or oesophagogastric junction adenocarcinoma: an open-label, dose de-escalation phase 1b study and a double-blind, randomised phase 2 study. Lancet Oncol [online]. 2014, vol. 15, p. 1007-1018. https://doi.org/10.1016/S1470-2045(14)70023-3 Ver referência
30. Malka, D and François, E and Penault-Llorca, F. FOLFOX alone or combined with rilotumumab or panitumumab as first-line treatment for patients with advanced gastroesophageal adenocarcinoma (PRODIGE 17-ACCORD 20-MEGA): a randomised, open-label, three-arm phase II trial. Eur J Cancer [online]. 2019, vol. 115, p. 97-106.
31. Catenacci, D VT and Tebbutt, N C and Davidenko, I. Rilotumumab plus epirubicin, cisplatin, and capecitabine as first-line therapy in advanced MET-positive gastric or gastro-oesophageal junction cancer (RILOMET-1): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol [online]. 2017, vol. 18, p. 1467-1482.
32. Klempner, S J and Shitara, K and Sison, A. STAR-221: A randomized, open-label, multicenter, phase 3 trial of domvanalimab, zimberelimab, and chemotherapy versus nivolumab and chemotherapy in previously untreated, locally advanced, unresectable or metastatic gastric, gastroesophageal junction, and esophageal adenocarcinoma. American Society of Clinical Oncology, 2023.
33. Kim, M and Seo, A N. Molecular Pathology of Gastric Cancer. J Gastric Cancer [online]. 2022, vol. 22, p. 273-305. https://doi.org/10.5230/jgc.2022.22.e35 Ver referência
34. Drilon, A and Laetsch, T W and Kummar, S. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N Engl J Med [online]. 2018, vol. 378, p. 731-739.
35. trial investigators. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1-2 trials. Lancet Oncol [online]. 2020, vol. 21, p. 271-282.
36. Kang, J H and Lee, S I and Lim, D H. Salvage chemotherapy for pretreated gastric cancer: a randomized phase III trial comparing chemotherapy plus best supportive care with best supportive care alone. J Clin Oncol [online]. 2012, vol. 30, p. 1513-1518. https://doi.org/10.1200/JCO.2011.39.4585 Ver referência
37. Shitara, K and Doi, T and Dvorkin, M. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol [online]. 2018, vol. 19, p. 1437-1448.
38. Janjigian, Y Y. “Pembrolizumab plus trastuzumab and chemotherapy for HER2-positive gastric or gastro-oesophageal junction adenocarcinoma: interim analyses from the phase 3 KEYNOTE-811 randomised placebo-controlled trial.”. Lancet (London, England) [online]. , p. 2197-2208. https://doi.org/10.1016/S0140-6736(23)02033-0 Ver referência
39. Tabernero, J. “HERIZON-GEA-01: Zanidatamab + chemo ± tislelizumab for 1L treatment of HER2-positive gastroesophageal adenocarcinoma.”. Future oncology (London, England) [online]. , p. 3255-3266. https://doi.org/10.2217/fon-2022-0595 Ver referência
40. Janjigian, Y Y. EDGE-Gastric Arm A1: Phase 2 study of domvanalimab, zimberelimab, and FOLFOX in first-line (1L) advanced gastroesophageal cancer. JCO [online]. . https://doi.org/10.1200/JCO.2023.41.36_suppl.433248 Ver referência
Dados de acesso insuficientes para visualização no mapa.