Endometrial cancer (EC) is the sixth most prevalent cancer in women worldwide.
The treatment recommendations for EC are typically driven by the grade and stage of the disease.
The standard of care during the study period regarding the first-line therapy (1L) for advanced/relapsed EC was platinum-based therapy (PBT); however, the prognosis is poor, with limited duration of the benefits.
There is a scarcity of real-world data regarding patient characteristics, treatment patterns, and clinical outcomes in women with EC, especially in Latin America.
Therefore, the Endometrial Cancer Health and Clinical Outcomes Study in Brazil (ECHOS-B) was conducted to describe real-world treatment patterns and outcomes in women with EC in Brazil who had received 1L with PBT in the private healthcare system.
The ECHOS-B was a retrospective, longitudinal study based on Brazilian administrative claims from the private healthcare setting (extracted from the Orizon database). The Orizon database covers around 20% of the private healthcare system in Brazil.
We collected data on privately-insured female patients aged ≥ 18 years (at the index date, that is, the proxy for EC diagnosis), who had received an International Classification of Diseases, 10th revision (ICD-10) diagnostic code (C54: malignant neoplasm of corpus uteri) for EC ≥ 2 times (
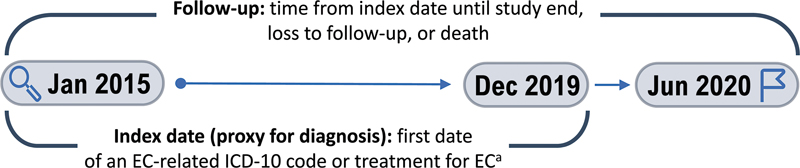
Fig. 1 Study design. Abbreviations: EC, endometrial cancer; HT, hormone therapy; ICD-10, International Classification of Diseases, 10th revision; IT, immunotherapy. Notes: aAn image examination, hospitalization, emergency visit, biopsy, surgery, radiotherapy, or systemic therapy (chemotherapy, HT, or IT) related to EC management.
The study objectives were to describe real-world treatment patterns in Brazil for women with EC who had received 1L with PBT, alone or in combination with another treatment. The sample included patients receiving initial PBT chemotherapy in either adjuvant or neoadjuvant therapy. Additional objectives were to describe the demographic and clinical characteristics (duration of follow-up, time from index date to 1L with PBT, duration of 1L with PBT, and time until the next treatment [TTNT]). Estimated real-world progression-free survival (rwPFS) and real-world OS (rwOS) after 1L with PBT were also evaluated.
The first claim for a systemic therapy was identified as the initiation of 1L. A regimen was considered as including all systemic therapies administered concomitantly, or within a maximum gap of 30 days. All systemic therapies of interest related to EC treatment were based on the National Comprehensive Cancer Network Clinical Practice Guidelines.
The end of 1L with PBT was defined as the date of the last drug administration: 1) preceding an interval of more than 120 days between drugs; or 2) preceding the addition of a new drug different from the initial regimen. If the final drug in the LOT was an oral treatment and continued for up to 30 days, overlapping with the initiation of a new drug, then the date immediately preceding the start of the new drug was considered. The 120-day gap started on the first day after the last day of administration of the therapy regimen.
Accordingly, the start of the second-line therapy (2L) was defined as the date of the start of a new systemic therapy that was not part of the previous LOT, or the time of resumption of the same treatment regimen (that is, retreatment, after an interval of > 120 days).
Eligible patients receiving any systemic therapy had the first two LOTs identified for regimen and duration; thus the population of interest was classified as patients receiving 1L with PBT. The follow-up (in months) of these patients was calculated from the index date until the final period of the study (June 30, 2020), until a loss to follow-up was identified, or until death, whichever occurred first.
In the same LOT, a patient may have received more than one therapeutic class (PBT, non-PBT, HT, IT). The patients could only be allocated to one combination group.
A frequency distribution was generated to report all unique combinations in the treatment regimens received by the patients included in the final analysis.
The results were interpreted descriptively; no country-level generalizations were made. For the continuous variables, descriptive statistics of central tendency (mean or median values) and dispersion (standard deviation or interquartile range [IQR] values) are presented. The analysis included only patients with data available and who met the inclusion criteria. The duration of 1L with PBT (in months) was defined as the time from the first to the last dates of drug administration in the LOT. The TTNT was defined as the time from the start of the first platinum-based drug to the start of 2L. The rwPFS was estimated from the date of the first drug administration in the 1L with PBT to progression (new regimen of systemic therapy or death).
The estimated rwPFS and rwOS were evaluated through the Kaplan–Meier non-parametric statistical analysis, and the cumulative risk per year of follow-up was calculated.
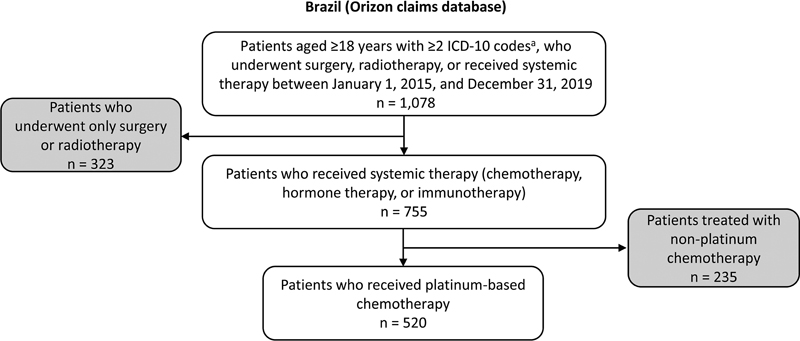
A total of 1,078 patients diagnosed with EC in the study period were treated with surgery, radiotherapy, and/or any systemic therapy (
Fig. 2 Flowchart of the study population. Abbreviation: ICD-10, International Classification of Diseases, 10th revision. Notes: aC54, malignant neoplasm of corpus uteri.
| Therapy | 1L (n = 755) | 2L (n = 279) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Therapeutic class | ||||
| Chemotherapy (PBT) | 520 | 68.9 | 129 | 46.2 |
| Chemotherapy (non-PBT) | 590 | 78.1 | 199 | 71.3 |
| IT | 105 | 13.9 | 66 | 23.7 |
| HT | 73 | 9.7 | 44 | 15.8 |
| Therapeutic class combination | ||||
| PBT | 46 | 6.1 | 16 | 5.7 |
| PBT + IT | 3 | 0.4 | – | – |
| PBT + HT | 1 | 0.1 | 1 | 0.4 |
| PBT + non-PBT | 433 | 57.4 | 88 | 31.5 |
| PBT + non-PBT + IT | 33 | 4.4 | 18 | 6.5 |
| PBT + non-PBT + HT | 4 | 0.5 | 4 | 1.4 |
| PBT + non-PBT + IT + HT | – | – | 2 | 0.7 |
| Non-PBT | 105 | 13.9 | 74 | 26.5 |
| Non-PBT + IT | 8 | 1.1 | 10 | 3.6 |
| Non-PBT + HT | 3 | 0.4 | 3 | 1.1 |
| Non-PBT + IT + HT | 3 | 0.4 | – | – |
| IT + HT | 5 | 0.7 | 7 | 2.5 |
| HT | 57 | 7.5 | 27 | 9.7 |
| IT | 53 | 7.0 | 29 | 10.4 |
Abbreviations: 1L, first-line therapy; 2L, second-line therapy; HT, hormone therapy; IT, immunotherapy; PBT, platinum-based therapy.
Notes:aPatients could receive more than one therapeutic class in the same line of therapy. bPatients could only appear in one combination group.
For the subgroup of patients who received 1L with PBT (n = 520), the mean treatment duration was 3.1 ± 2.5 months (
| Age group on the index date | n (%) |
|---|---|
| 18–39 years | 14 (6.8) |
| 40–49 years | 25 (12.2) |
| 50–59 years | 47 (22.9) |
| 60–69 years | 74 (36.1) |
| ≥ 70 years | 45 (22.0) |
| Missing data | 315 (60.6) |
| Mean age on the index date (years) | 61.0 ± 12.3 |
|
| |
| Index year | n (%) |
| 2015 | 161 (31.0) |
| 2016 | 98 (18.8) |
| 2017 | 97 (18.7) |
| 2018 | 78 (15.0) |
| 2019 | 86 (16.5) |
| Duration of follow-up (months) | |
| Mean | 22.8 ± 16.3 |
| Median (IQR) | 17.2 (21.8) |
| Time from index date to 1L with PBT (months) | |
| Mean | 4.8 ± 6.3 |
| Median (IQR) | 3.4 (4.3) |
| Duration of 1L with PBT (months) | |
| Mean | 3.1 ± 2.5 |
| Median (IQR) | 3.4 (2.5) |
| Time in months until next treatment from 1L to 2L (PBT or non-PBT) | |
| Mean | 9.4 ± 7.3 |
| Median (IQR) | 7.9 (8.2) |
| Geographical region for the service claim | n (%) |
| Midwest | 43 (8.3) |
| North | 11 (2.1) |
| Northeast | 67 (13.0) |
| South | 19 (3.7) |
| Southeast | 376 (72.9) |
| Missing data | 4 (0.8) |
Abbreviations: 1L, first-line therapy; 2L, second-line therapy; IQR, interquartile range; PBT, platinum-based therapy.
For patients treated with surgery, radiotherapy, and/or any systemic therapy (n = 1,078), the mean time from the index date to the first treatment was 2.5 ± 5.4 months. The mean time from the index date to 1L with PBT was 4.8 ± 6.3 months. The mean TTNT was 9.4 ± 7.3 months, based on the 173 patients who progressed to 2L.
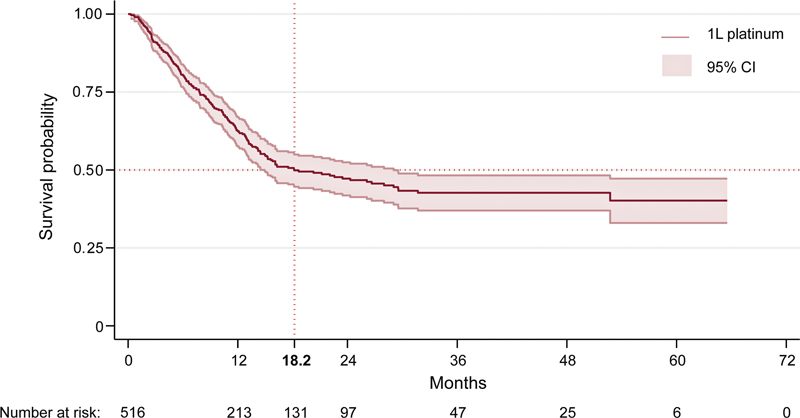
Overall, the median adjusted rwPFS among those submitted to 1L with PBT was 18.2 months (
Fig. 3 Kaplan–Meier curve for the estimated real-world progression-free survival after 1L with PBT (Orizon database; January 1, 2015–June 30, 2020). Abbreviations: 1L, first-line therapy; CI, confidence interval; PBT, platinum-based therapy. Notes: Death was included as progression. Four patients who progressed on the same day as 1L completion were not included in this analysis.
| Year | n | Patients who progressed (n) | Patients lost to follow-up (n) | Percentage of cumulative risk (95% CI) |
|---|---|---|---|---|
| 0–1 | 520 | 162 | 145 | 36.2 (31.9–40.8) |
| 1–2 | 213 | 44 | 72 | 52.1 (46.9–57.4) |
| 2–3 | 97 | 8 | 42 | 57.1 (51.4–62.9) |
| 3–4 | 47 | 0 | 22 | 57.1 (51.4–62.9) |
| 4–5 | 25 | 1 | 18 | 59.8 (52.5–67.2) |
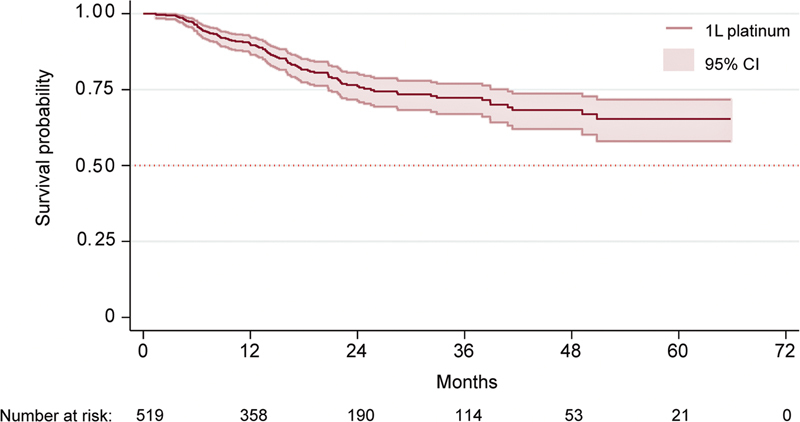
| Year | n | Patients who died (n) | Patients lost to follow-up (n) | Percentage of cumulative risk (95% CI) |
| 0–1 | 520 | 48 | 114 | 10.4 (7.9–13.5) |
| 1–2 | 358 | 44 | 124 | 23.7 (19.7–28.4) |
| 2–3 | 190 | 8 | 68 | 27.6 (23.1–32.8) |
| 3–4 | 114 | 5 | 56 | 31.8 (26.4–38.0) |
| 4–5 | 53 | 2 | 30 | 35.4 (28.6–43.3) |
Abbreviations: CI, confidence interval; 1L, first-line therapy; PBT, platinum-based therapy.
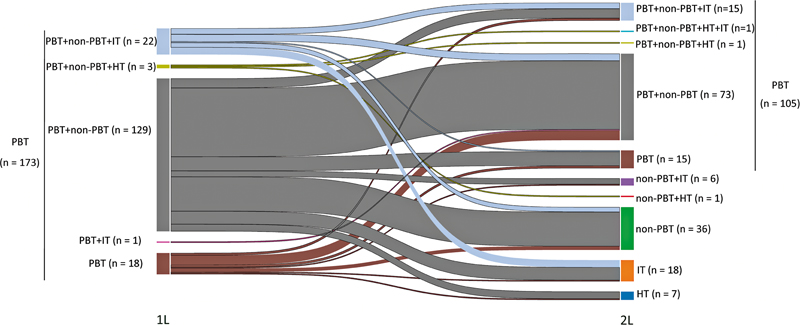
Progression after 1L with PBT occurred in 41.3% of the patients (n = 215/520; 58.7% [n = 305/520] were lost to follow-up). Of these, 80.5% (n = 173/215) received another systemic treatment regimen, and 19.5% (n = 42/215) died.
Among the 173 patients who received another systemic treatment regimen, 60.7% (n = 105/173) continued to be treated with PBT. The Sankey diagram (
Fig. 4 Sankey plot from 1L to 2L among patients with endometrial cancer who received 1L with PBT (Orizon database; January 1, 2015–June 30, 2020). Abbreviations: 1L, first-line therapy; 2L, second-line therapy; HT, hormone therapy; IT, immunotherapy; PBT, platinum-based therapy.
A total of 107 deaths (20.6%) were registered during the study, with a mean time from the index date to death of 14.9 ± 10.2 months (median: 13.4; IQR: 14.1). The Kaplan–Meier rwOS estimates in patients treated with 1L with PBT are shown in
Fig. 5 Kaplan–Meier curve for real-world overall survival after 1L with PBT (Orizon database; January 1, 2015–June 30, 2020). Abbreviations: 1L, first-line therapy; CI, confidence interval; PBT, platinum-based therapy. Notes: Death was included as progression. One patient who contributed with zero person-time was not included in this analysis.
Real-world data are lacking for patients with EC, especially in Latin American countries.
In the present study, we analyzed data from 1,078 Brazilian women with private health insurance between 2015 and 2020. Most patients (70.0%) received 1L, more than 2/3 of whom (68.9%) received 1L with PBT. Almost 60% of the women treated with 1L with PBT were aged ≥ 60 years, which is indicative of a demographic considered at a high risk of developing EC.
All Brazilians are covered by public health insurance; in 2022, 25% of the population was also covered by private health insurance, which is considered to provide easier access to certain services or professionals.
The prognosis of patients with EC has been shown to be correlated with delays in diagnosis and treatment initiation.
Due to the paucity of real-world data on treatment patterns and outcomes for EC, comparisons of the patients submitted to 1L with PBT herein described with other real-world studies are challenging. Nonetheless, in the present study, the cumulative rwOS rates after 1L with PBT decreased over time, which was broadly consistent with trends observed in other real-world studies—albeit in patients with advanced/recurrent EC who received prior chemotherapy.
Currently, the treatment options for women with EC progressing after 1L are limited.
In the current study, a large proportion (60.7%) of patients who experienced progression received rechallenge with PBT. While there is no globally-accepted standard of care in the 2L, our data are consistent with those of other real-world studies,
The EC treatment setting has altered markedly in recent years, and immune-oncology and chemotherapy-based combination regimens are recommended as 1L options for advanced/recurrent disease.
In line with the EC treatment landscape during the study period, in the current study, chemotherapy dominated the treatment choice in the 1L and 2L settings. Furthermore, the use of immunotherapy was low in 1L, with more than 10% of the patients receiving immunotherapy treatment, a rate that increased to more than 20% in 2L. The approval of dostarlimab in Brazil, in 2022 for 2L for patients with advanced/recurrent MMRd/MSI-H EC, and more recently in 2024 for 1L in combination with chemotherapy, is bringing patients in this region closer to accessing novel therapies. Consequently, we may observe a shift in treatment patterns.
The ECHOS-B used data from the private healthcare system, which suggests that patients have access to optimal care; however, some potential limitations should be considered. The findings should be interpreted considering the specific population that the Orizon database represents. As patients at any stage of the disease could be included in our dataset, there are limitations to the interpretation and evaluation of the treatment patterns herein reported regarding disease severity. The subset of patients receiving PBT in 1L likely reflects those with advanced disease, either undergoing adjuvant or neoadjuvant therapy, and the study is limited in terms of distinguishing them. Due to this, the longer-than-expected rw PFS observed in the study may reflect this limitation, although, in our dataset, the number of patients treated with surgery and drugs was small (lower than 4%; data not shown). Treatments or hospitalizations that ultimately occur in the public healthcare system are not captured by the Orizon database; therefore, the results cannot be generalized to the population with lower socioeconomic status, or to the public healthcare system, to which all Brazilians have access.
Other limitations include those traditionally associated with retrospective analyses, such as problems with the quality of data recording in the local clinical practice and the availability of clinical information. In addition, analyses of data on administrative claims depend on correct coding for diagnoses, procedures, and drugs, such that any coding inaccuracies may lead to case misidentification.
The ECHOS-B provides valuable insight into real-world treatment patterns and outcomes for patients with EC in Brazil. Our findings demonstrate that PBT is frequently (∼ 70%) used in 1L, with high rates of progression and with most progression events occurring within 2 years. These findings enhance EC awareness and clarify current and emerging treatment options, particularly as clinicians gain experience with novel immunotherapies. Recent developments and approvals of novel immune-oncology therapies for advanced/recurrent EC will undoubtedly lead to improvements in patient outcomes both in Brazil and worldwide.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. [cited 2024 October 17] [online]. Available from: <https://www.wcrf.org/cancer-trends/endometrial-cancer-statistics/>.
2. [cited 2024 October 17] [online]. Available from: <https://gco.iarc.who.int/media/globocan/factsheets/cancers/24-corpus-uteri-fact-sheet.pdf>.
3. [cited 2024 October 17] [online]. Available from: <https://gco.iarc.who.int/media/globocan/factsheets/populations/76-brazil-fact-sheet.pdf>.
4. [cited 2024 October 17] [online]. Available from: <https://gco.iarc.fr/tomorrow/en/dataviz/bars?cancers=24&key=percent&show_bar_mode_prop=0&sexes=2&populations=76_900&years=2050>.
5. ESMO-ESGO-ESTRO Endometrial Consensus Conference Working Group. ESMO-ESGO-ESTRO consensus conference on endometrial cancer: diagnosis, treatment and follow-up. Int J Gynecol Cancer [online]. 2016, vol. 26, p. 2-30. https://doi.org/10.1097/IGC.0000000000000609 Ver referência
6. Abu-Rustum, N R and Yashar, C M and Bradley, K and Campos, S M and Chino, J and Chon, H S. NCCN Guidelines® Insights: Uterine Neoplasms, Version 3.2021. J Natl Compr Canc Netw [online]. 2021, vol. 19, p. 888-895. https://doi.org/10.6004/jnccn.2021.0038 Ver referência
7. ESMO Guidelines Committee.. Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol [online]. 2022, vol. 33, p. 860-877. https://doi.org/10.1016/j.annonc.2022.05.009 Ver referência
8. Ades, F. Access to oncology drugs in Brazil: juggling innovation and sustainability in developing countries. Med Access @. Point Care [online]. 2017, vol. 1, p. e10-e15. https://doi.org/10.5301/maapoc.0000004 Ver referência
9. Andrade, DAPd and Guimarães, A PG and Melo, ACd and Nogueira-Rodrigues, A and Gomes, L M and Scaranti, M. Management of patients with recurrent/metastatic endometrial cancer: Consensus recommendations from an expert panel from Brazil. Front Oncol [online]. 2023, vol. 13, p. 1133277. https://doi.org/10.3389/fonc.2023.1133277 Ver referência
10. Blanco, A and Nogueira-Rodrigues, A and Carvalho, F M and Giornelli, G and Mirza, M R. Management of endometrial cancer in Latin America: raising the standard of care and optimizing outcomes. Int J Gynecol Cancer [online]. 2024, vol. 34, p. 1263-1272. https://doi.org/10.1136/ijgc-2023-005017 Ver referência
11. [cited 2024 October 17] [online]. Available from: <https://oncologiabrasil.com.br/anvisa-aprova-dostarlimabe-em-monoterapia-para-o-tratamento-do-carcinoma-de-endometrio/>.
12. Paulino, E and Melo, A C. Clinical characteristics and outcomes of a high-grade endometrial cancer cohort treated at Instituto Nacional de Câncer, Brazil. Rev Bras Ginecol Obstet [online]. 2023, vol. 45, p. e401-e408. https://doi.org/10.1055/s-0043-1772177 Ver referência
13. Brüggmann, D and Ouassou, K and Klingelhöfer, D and Bohlmann, M K and Jaque, J and Groneberg, D A. Endometrial cancer: mapping the global landscape of research. J Transl Med [online]. 2020, vol. 18, p. 386. https://doi.org/10.1186/s12967-020-02554-y Ver referência
14. [cited 2024 October 17] [online]. Available from: <https://www.orizonbrasil.com.br/sobre-a-orizon.html>.
15. . [cited 2024 October 17] [online]. Available from: <https://www.gov.br/anvisa/pt-br/english>.
16. Friends of Cancer Research. Establishing a Framework to Evaluate Real-World Endpoints. Friends of Cancer Research, 2018.
17. Sousa, FGd and Prates, A BC and Leal, A NA and Xavier, L B and Andrade, DAPd and Nogueira-Rodrigues, A. Identifying areas at risk of endometrial cancer increase in Latin America: development of a geospatial model. Lancet Oncol [online]. 2022, vol. 23, p. S41. https://doi.org/10.1016/S1470-2045(22)00440-5 Ver referência
18. Soares, C and Abreu, G and Queiroz, J and Silva, T LNd and Menezes, P and Carrizo, M. Endometrial cancer treatment and outcomes in Argentina: ECHOS-A real-world study. Gynecol Oncol Rep [online]. 2024, vol. 54, p. 101457. https://doi.org/10.1016/j.gore.2024.101457 Ver referência
19. Monk, B J and Smith, G and Lima, J and Long, G H and Alam, N and Nakamura, H. Real-world outcomes in patients with advanced endometrial cancer: A retrospective cohort study of US electronic health records. Gynecol Oncol [online]. 2022, vol. 164, p. 325-332. https://doi.org/10.1016/j.ygyno.2021.12.008 Ver referência
20. Heffernan, K and Nikitas, F S and Shukla, U and Camejo, H S and Knott, C. Previously treated recurrent or advanced endometrial cancer in England: A real-world observational analysis. Gynecol Oncol [online]. 2022, vol. 166, p. 317-325. https://doi.org/10.1016/j.ygyno.2022.06.011 Ver referência
21. Akada, K and Koyama, N and Miura, T and Fukunaga, E and Miura, Y and Aoshima, K and Fujiwara, K. Real-world database analysis of the characteristics and treatment patterns of patients with endometrial cancer in Japan. Curr Med Res Opin [online]. 2021, vol. 37, p. 1171-1178. https://doi.org/10.1080/03007995.2021.1903847 Ver referência
22. Prabhu, V S and Kelkar, S S and Zhang, J and Ogando, Y M and Miles, N and Marth, C. 2022-RA-702-ESGO real-world treatment patterns and outcomes in recurrent or advanced endometrial cancer patients initiating 1st-line systemic therapy in Europe: a retrospective chart review study. Int J Gynecol Cancer [online]. 2022, vol. 32, p. A104-A105. https://doi.org/10.1136/ijgc-2022-ESGO.227 Ver referência
23. Silva, B and Hens, N and Gusso, G and Lagaert, S and Macinko, J and Willems, S. Dual use of public and private health care services in Brazil. Int J Environ Res Public Health [online]. 2022, vol. 19, p. 1829. https://doi.org/10.3390/ijerph19031829 Ver referência
24. Anton, C and Kleine, R T and Mayerhoff, E and Diz, M dPE and Freitas, D d and Carvalho, H dA. Ten years of experience with endometrial cancer treatment in a single Brazilian institution: Patient characteristics and outcomes. PLoS One [online]. 2020, vol. 15, p. e0229543. https://doi.org/10.1371/journal.pone.0229543 Ver referência
25. Paulino, E and de Melo, A C and Nogueira-Rodrigues, A and Thuler, L CS. Gynecologic cancer in Brazil and the law of sixty days. J Gynecol Oncol [online]. 2018, vol. 29, p. e44. https://doi.org/10.3802/jgo.2018.29.e44 Ver referência
26. Gioia, S and Brigagao, L and Rocha, M and Goss, P. Patient navigation: fighting for the rights of breast cancer patients in Brazil. Mastology [online]. 2021, vol. 31, p. e20200068. https://doi.org/10.29289/2594539420200068 Ver referência
27. Paulino, E and de Melo, A C and Silva-Filho, A L and Maciel, L dF and Thuler, L CS and Goss, P and Nogueira-Rodrigues, A. Panorama of gynecologic cancer in Brazil. JCO Glob Oncol [online]. 2020, vol. 6, p. 1617-1630. https://doi.org/10.1200/GO.20.00099 Ver referência
28. Candido, E C and Veiga Junior, N N and Minari, M P and Toledo, M CS and Yela, D A and Teixeira, J C. Malignant uterine neoplasms attended at a Brazilian regional hospital: 16-years profile and time elapsed for diagnosis and treatment. Rev Bras Ginecol Obstet [online]. 2021, vol. 43, p. 137-144. https://doi.org/10.1055/s-0040-1718434 Ver referência
29. Liu, J and Emond, B and Maiese, E M and Lafeuille, M-H and Lefebvre, P and Ghelerter, I. Real-world utilization and outcomes of systemic therapy among patients with advanced or recurrent endometrial cancer in the United States. Curr Med Res Opin [online]. 2022, vol. 38, p. 1935-1945. https://doi.org/10.1080/03007995.2022.2112872 Ver referência
30. Huijgens, A N and Mertens, H J. Factors predicting recurrent endometrial cancer. Facts Views Vis ObGyn [online]. 2013, vol. 5, p. 179-186.
31. Abu-Rustum, N and Yashar, C and Arend, R and Barber, E and Bradley, K and Brooks, R. Uterine Neoplasms, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw [online]. 2023, vol. 21, p. 181-209. https://doi.org/10.6004/jnccn.2023.0006 Ver referência
32. Brooks, R A and Fleming, G F and Lastra, R R and Lee, N K and Moroney, J W and Son, C H. Current recommendations and recent progress in endometrial cancer. CA Cancer J Clin [online]. 2019, vol. 69, p. 258-279. https://doi.org/10.3322/caac.21561 Ver referência
33. Di Tucci, C and Capone, C and Galati, G and Iacobelli, V and Schiavi, M C and Di Donato, V. Immunotherapy in endometrial cancer: new scenarios on the horizon. J Gynecol Oncol [online]. 2019, vol. 30, p. e46. https://doi.org/10.3802/jgo.2019.30.e46 Ver referência
34. Post, C CB and Westermann, A M and Bosse, T and Creutzberg, C L and Kroep, J R. PARP and PD-1/PD-L1 checkpoint inhibition in recurrent or metastatic endometrial cancer. Crit Rev Oncol Hematol [online]. 2020, vol. 152, p. 102973. https://doi.org/10.1016/j.critrevonc.2020.102973 Ver referência
35. Rubinstein, M and Shen, S and Monk, B J and Tan, D SP and Nogueira-Rodrigues, A and Aoki, D. Looking beyond carboplatin and paclitaxel for the treatment of advanced/recurrent endometrial cancer. Gynecol Oncol [online]. 2022, vol. 167, p. 540-546. https://doi.org/10.1016/j.ygyno.2022.10.012 Ver referência
36. Martins, D and O'Sullivan, D E and Boyne, D J and Cheung, W Y and Allonby, O and Habash, M. Understanding characteristics, treatment patterns, and clinical outcomes for individuals with advanced or recurrent endometrial cancer in Alberta, Canada: a retrospective, population-based cohort study. Curr Oncol [online]. 2023, vol. 30, p. 2277-2289. https://doi.org/10.3390/curroncol30020176 Ver referência
37. Rubinstein, M and Halpenny, D and Makker, V and Grisham, R N and Aghajanian, C and Cadoo, K. Retreatment with carboplatin and paclitaxel for recurrent endometrial cancer: A retrospective study of the Memorial Sloan Kettering Cancer Center experience. Gynecol Oncol Rep [online]. 2019, vol. 28, p. 120-123. https://doi.org/10.1016/j.gore.2019.04.002 Ver referência
38. [cited 2024 October 17] [online]. Available from: <https://www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf>.
39. [cited 2024 October 17] [online]. Available from: <https://www.ema.europa.eu/en/medicines/human/EPAR/keytruda>.
40. [cited 2024 October 17] [online]. Available from: <https://gskpro.com/content/dam/global/hcpportal/en_US/Prescribing_Information/Jemperli/pdf/JEMPERLI-PI-MG.PDF>.
41. [cited 2024 October 17] [online]. Available from: <https://www.ema.europa.eu/en/medicines/human/EPAR/jemperli>.
42. Powell, M A and Bjørge, L and Willmott, L and Novák, Z and Black, D and Gilbert, L. Overall survival in patients with endometrial cancer treated with dostarlimab plus carboplatin-paclitaxel in the randomized ENGOT-EN6/GOG-3031/RUBY trial. Ann Oncol [online]. 2024, vol. 35, p. 728-738. https://doi.org/10.1016/j.annonc.2024.05.546 Ver referência
43. [cited 2024 October 17] [online]. Available from: <https://www.gov.br/anvisa/pt-br/assuntos/medicamentos/novos-medicamentos-e-indicacoes/jemperli-dostarlimabe-nova-indicacao>.
Dados de acesso insuficientes para visualização no mapa.