Breast cancer is a major health problem for women, due to its high incidence rate.
Physical exercise has been associated with a reduced risk of recurrence of certain neoplasms (breast cancer and colorectal cancer).
In Brazil, a manual of physical activity recommendations has been developed, aiming to help health professionals to facilitate the population in the prevention and control of cancer. Since this habit needs to be included in the treatment guidelines,
This study has been carried out in the Clinical Outcomes Program at the Hospital Moinhos de Vento (HMV) in Porto Alegre. The program aims to evaluate the health outcomes of patients diagnosed with breast cancer inside HMV, a private and philanthropic institution in Porto Alegre, in southern Brazil, that is recognized for its excellent service for oncological needs.
This article has been written based on the criteria established by the protocol STrengthening the Reporting of OBservational studies in Epidemiology (STROBE).
This is a cohort, longitudinal, observational and prospective study, aiming to evaluate the impact of physical exercise in the oncological treatment of patients with breast cancer. The recruitment of participants for the study has been carried out by convenience, with the target population being patients participating in the Clinical Outcomes Program from HMV. The inclusion criteria for the present study were: women over 18 years old, with a confirmed diagnosis of breast cancer, without previous treatment and who started their cancer treatment at the institution of interest, which may be surgical, chemotherapy, radiotherapy or hormone therapy. There was no restriction on participation in the study by type of breast cancer, staging or type of treatment, as the clinical profile of patients treated at the hospital's oncology service is very heterogeneous and each patient receives an individualized treatment plan according to their needs and demands. In addition to that, it has been required for those patients to answer the questionnaire during the period of diagnosis, ongoing treatment and after 6 months of treatment. Foreign patients, patients who had already started treatment, relapses and rare tumors were excluded from the study.
The data collection period has been carried out between November 2018 and July 2022. Every time a patient meeting the inclusion and exclusion criteria was included in the Clinical Outcomes Program, a member of the assessment team was responsible for contacting them in order to verify their interest in participating in the study. The initial contact was carried out through telephone calls with the help of research assistants, and also in face-to-face appointments at the Nucleo Mama, by a nursing professional. If the patient manifests interest in participating in the study, the term of free and informed consent was provided, and the main study objectives and procedures were presented and discussed in detail. After signing the term, a trained member of the research team conducted the interview for data collection, the survey forms followed the International Consortium for Health Outcomes Measurement (ICHOM) methodology. All data was collected and stored by using the Research Electronic Data Capture (RedCap) software database.
The main data for the present study was collected through a semi-structured questionnaire, which has been validated using the ICHOM methodology.
Sociodemographic data, including age, sex, level of education, and marital status;
Physical exercise questions, containing the type of physical activity performed (if any), weekly frequency of practices, and duration of physical exercise in minutes;
Assessment of QoL, clinical outcomes (pain, fatigue, physical and emotional consequences derived from cancer treatment) treatment side effects. These three contexts were evaluated through the application of EORTC-QLQ-C30/EORTC-QLQ-BR2 scale. This instrument was originally created by the European Organization Research and Treatment of Cancer (EORTC) and is widely used to measure QoL and related aspects among people with cancer. The questionnaire presents 47 questions that evaluate 12 clinical outcomes domains: daily activities functioning, physical functioning, emotional functioning, cognitive functioning, social functioning, total score of functioning, pain, fatigue, symptoms, treatment side effects, global health score, and total QoL score.
Six months after starting treatment, all included participants received a telephone call in order to reapply the same questionnaire. The follow-up times for each patient were described as T0 (data collected right after diagnosis of breast cancer) and T180 (data collected 6 months after initiation of treatment).
The study protocol has been approved by the Ethics Committee (CEP) and all patients have had a free and informed consent form signed. The data collected from each patient has been used only for research purposes.
Initially, the data were dozwnloaded in Excel format, and submitted into SAV format, in order to carry out the statistical analyses using the SPSS software version 21.0 (IBM SPSS Statistics). The QoL questionnaire has been divided into scores for physical, emotional, social, cognitive, pain, fatigue, and cancer symptoms, creating scores for each health condition.
Qualitative variables have been described using absolute and relative frequencies. The distribution of continuous quantitative variables has been analyzed using the Shapiro-Wilk test, where all of them have shown an asymmetrical distribution. Therefore, these variables were described by median and interquartile range (IQ). For the general analyses, the study participants were divided into two groups: those without physical exercise after six months of treatment and those with physical exercise after six months of treatment. It has verified the difference in intragroup and intergroup scores at times of T0 and T180. Therefore, the comparison of clinical and QoL scores at T0 and T180 has been performed using the Wilcoxon test. The comparison of scores between the group that has been performing physical exercise and the group that has not been performing physical exercise after six months of treatment was performed using the Mann-Whitney test. Afterwards, in order to identify factors associated with changes in the practice of physical exercise during cancer treatment, the participants have been divided into four groups: never exercised, stopped exercising during treatment, started exercising during treatment and always exercised. The comparison of scale scores between the four groups has been performed using the Kruskal-Walys test.
The correlation between the weekly physical exercise performed by the participants and the clinical scores, as well as QoL has been evaluated using Spearman's correlation test.
Finally, a multiple linear regression analysis has been performed in order to evaluate the association between average factors (age, instructional level, presence of comorbidities), practice of physical exercise and treatment systemic side effects as well as the outcome variables (scales functioning, fatigue and QoL).
All the analysis considered a significance level of 5%.
A total of 196 people agreed to participate in the study. As the research was being carried out, 150 answered the form when they were diagnosed (T0) and also 6-months after starting their treatment (T180). One patient was excluded from the study because he was male. Therefore, a total of 149 participants were included in this study, all female (100.0%), with an average age of 58.0 years old [IQ: 44-68], with the majority of white ethnicity (99.3%). In this regard, 51.7% of the participants had at least one comorbidity and 56.4% reported being in the postmenopausal period. Regarding the histological type of breast cancer, the most prevalent was invasive ductal carcinoma (n=108; 72.5%), and most women were in stage I of the tumor (TNM) (n=93; 62.4%). There was a wide combination of different treatments in the sample; however, the vast majority of participants underwent surgery (n=129; 86.6%), with the surgery being the only treatment resource used in 62 participants. A smaller group of participants received chemotherapy (34.2%) and radiotherapy (24.2%). This smaller group has also had other treatment strategies combined. The details of the other sociodemographic and clinical characteristics of the sample are presented in
| Categorical variables | n=149 | % |
|---|---|---|
| Gender | ||
| Female | 149 | 100.0 |
| Level of Education | ||
| Complete Elementary complete | 6 | 4.0 |
| Intermediate incomplete | 4 | |
| Intermediate complete | 22 | 14.8 |
| Higher incomplete | 13 | 8.7 |
| Higher complete | 101 | 67.7 |
| Unknown | 3 | 2.0 |
| Marital Status | ||
| Single | 22 | 14.8 |
| Married and/or Common-law partner | 93 | 62.4 |
| Separated and/or Divorced | 15 | 10.1 |
| Widowed | 19 | 12,8 |
| Menopause | ||
| Premenopausal | 28 | 18.8 |
| Postmenopausal | 84 | 56.4 |
| Medication-induced amenorrhea | 37 | 24.8 |
| Presence of at least one comorbidity | ||
| No | 72 | 48.3 |
| Yes | 77 | 51.7 |
| Breast cancer staging in T0 | ||
| 0 (In situ) | 1 | 0.7 |
| I | 93 | 62.4 |
| II | 19 | 12.8 |
| III | 7 | 4.7 |
| IV | 3 | 2.0 |
| Unknown in T0 | 26 | 17.4 |
| Carcinoma histotype classification in T0 | ||
| In situ ductal carcinoma | 14 | 9.4 |
| Invasive ductal carcinoma | 108 | 72.5 |
| Invasive lobular carcinoma | 24 | 16.1 |
| Invasive ductal and lobular carcinoma | 3 | 2.0 |
| Type of treatment | ||
| Surgery | 129 | 86.6 |
| Radiotherapy | 36 | 24.2 |
| Chemotherapy | 51 | 34.2 |
| Hormone therapy | 23 | 15.4 |
| Combination of treatments | ||
| Only surgery | 63 | 42.3 |
| Surgery and other treatment types | 66 | 44.3 |
| One treatment type other than surgery | 10 | 6.7 |
| Two treatment types other than surgery | 9 | 6.0 |
| Numerical variables | Median | IQ |
| Age | 58.0 | [44.0 - 68.0] |
Regarding physical exercise, considering 149 patients included in the study, 54.4% reported not doing any type of exercises in the period they were diagnosed (T0). After six months of treatment, it has been found that 78 (52.3%) participants were practicing physical exercises and 71 (47.7%) participants did not exercise at all (
Graph 1 Relation of physical exercise practice among women with breast cancer six months after starting treatment.
It was also collected, through direct information, the type of exercise practiced during this period, and 14.7% reported taking more walks. In the average time of practice of physical exercise, we can observe that the practice of running and tennis exercises were performed in an average time of 240 minutes (
| Type of physical exercise | n=149 | % | Weakly time mean of exercise practice (minutes) |
|---|---|---|---|
| Walking | 22 | 14.7 | 116.2 |
| Running | 2 | 0.7 | 240.0 |
| Strength training (weight training, crossfit) | 18 | 12.1 | 221.3 |
| Aerobic exercise plus strength training | 21 | 14.1 | 182.5 |
| Gym classes (bike, zumba) | 10 | 6.7 | 112.5 |
| Tennis | 2 | 1.3 | 240.0 |
| Swimming | 2 | 1.3 | 120.0 |
| None | 71 | 47.7 | 0 |
2 subjects with the type of exercise missing.
When intragroup differences were found in QoL scores and clinical outcomes at T0 and T180, it has been observed that the group that were not exercising after six months of treatment presented worse results (T180) for physical performance scores, pain and treatment side effects (
| QoL scores | Without exercise (n=71) | With exercise (n=78) | Without exercise vs with exercise | ||||
|---|---|---|---|---|---|---|---|
| QoL scores | |||||||
| (T180) | |||||||
| T0 [IQ] | T180 [IQ] | p-value | T0 [IQ] | T180 [IQ] | p | value | |
| Physical functioning | 100.0 [93.3-100.0] | 93 ,3[80.0-100.0] | <0.001 | 100.0 [100.0-100.0] | 100.0 [100.0-100.0] | 0.946 | <0.001 |
| Daily tasks | 100.0 [100.0 -100.0] | 100.0 [83.3-100.0] | 0.190 | 100.0 [100.0-100.0] | 100.0[100.0 100.0] | 0.468 | <0.001 |
| Emotional functioning | 66.7 [50.0-83.3] | 91.7 [666.7-100.0] | <0.001 | 75.0 [50.0-83.3] | 100.0 [83.3-100.0] | <0.001 | 0.008 |
| Cognitive functioning | 100.0 [66.7-100.0] | 100.0 [100.0-100.0] | 0.027 | 100.0 [83.3-100.0] | 100.0 [100.0-100.0] | 0.269 | 0.808 |
| Social functioning | 100.0 [100.0-100.0] | 100.0 [83.3-100.0] | 0.532 | 100.0 [83.3-100.0] | 100.0 [100.0-100.0] | 0.0331 | 0.161 |
| Function score | 85.0 [78 .3-93.3] | 90.7 [80.0-98.7] | 0.024 | 90.8 [83.3-96.7] | 98.7 [89.6-100.0] | <0.001 | 0.002 |
| Fatigue | 0 [0-22.2] | 0 [0-22.2] | 0.237 | 0 [0-11.1] | 0 [0-2.8] | 0.475 | 0.002 |
| Pain | 0 [0-16.7] | 16.7 [2-33.3] | 0.003 | 0 [0-4.2] | 0 [0-16.7] | 0.2 | 0.006 |
| Symptoms | 1.2 [1.1-1.4] | 1.2 [1.1-1.4] | 0.567 | 1.1 [1 ,0-1.3] | 1.1 [1.0-1.23] | 0.016 | <0.001 |
| Overall health status | 83.3 [66.7-91.7] | 83.3 [66.7-91.7] | 0.03 | 83.3 [66.7-100.0] | 83.3[79.2-116.7] | 0.003 | 0.028 |
| Final sum QVQ | 89.7 [66.7-96.1] | 91.8 [86.7-97.3] | 0.09 | 92.3 [87.8-92.3] | 96.1[90.9-100.0] | <0.001 | 0.002 |
| Side effects of treatment | 9.5 [0-19.0] | 14.3 [4.8-28.6] | 0.015 | 4.8 [0-9.5] | 9.5 [0-14.3] | 0.349 | 0.003 |
Caption: T0: data collected after diagnosis and initiation of treatment. T180: data collected six months after starting treatment.
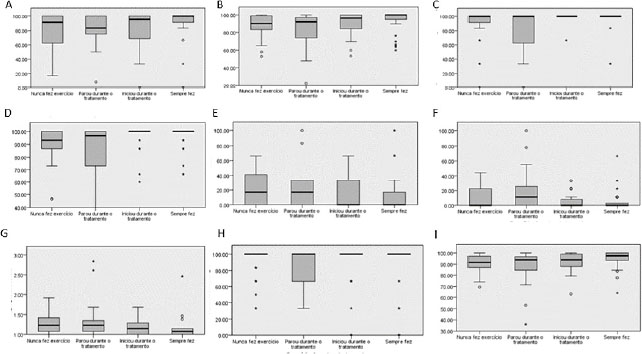
To verify the impact of changes in physical exercise behavior during treatment on clinical outcomes, the two groups were subdivided into four groups, namely: never exercised (n=49), stopped exercising during treatment (n=22), started exercising during treatment (n=32) and always did physical exercise (n=46). Comparison between groups for each of the QoL domains are presented in
Figure 1 Association of quality of life scores and clinical outcomes in the evaluated groups. Caption: A: Emotional functioning (p=0.012); B: Functional functioning (p=0.003); C: Daily tasks (p=0.001); D: Physical functioning (p=0.001); E: Pain (p=0.039); F: Fatigue (p=0.013); G: Symptoms (p=0.001); H: Social functioning (p=0.021); I: Total sum of quality of life scores (p=0.003). Comparisons performed using the Kruskal-Wallys test.
The scores for physical, social, emotional performance, daily tasks and the sum of the scores showed that those who have always exercised had better results, followed by those who had started exercises during treatment, those who never exercised and finally those who stopped exercising during the treatment. The scores for pain, fatigue and cancer symptoms showed that adverse reactions were higher in those who stopped physical activities during treatment, followed by those who never started any type of physical activities, those who started it during treatment and finally those who had regular physical activities.
The time of weekly physical exercise after six months of treatment showed a significant direct correlation with physical performance (ρ=0.288, p<0.001), daily tasks (ρ=0.288, p<0.001), emotional performance (ρ=0.206, p=0.012), performance score (ρ=0.213, p=0.009), global health status (ρ=0.209, p=0.011) and the sum of QoL scores (ρ=0.219, p=0.007), as shown in
| Scores | Correlation(p) | p-value |
|---|---|---|
| Physical functioning | 0,288 | <0,001 |
| Daily tasks | 0,288 | <0,001 |
| Emotional functioning | 0,206 | 0,012 |
| Cognitive functioning | 0,001 | 0,987 |
| Social functioning | 0,059 | 0,475 |
| Function score | 0,213 | 0,009 |
| Fatigue | -0,241 | 0,003 |
| Pain | -0,205 | 0,012 |
| Symptoms | -0,275 | <0,001 |
| Global health status | 0,209 | 0,011 |
| Sum QoV | 0,219 | 0,007 |
Through linear regression analysis, the association of sociodemographic variables, physical exercise practice, presence of comorbidities and systemic side effects was evaluated for treatment with the domains of physical performance, fatigue, daily tasks and the total QoL score, according to
| Physical functioning | Fatigue | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | B | CI95% | B standard | P | B | CI95% | B standard | P |
| Constant | 99.348 | 87.678; 111.019 | - | <0.001 | 5.399 | -9.356; 20.153 | - | <0.001 |
| Age | -0.123 | -0.272; -0.027 | -0.130 | 0.106 | 0.006 | -0.182; 0.195 | 0.006 | 0.946 |
| Level of education (high school) | 5.722 | -1.936; 13.379 | 0.183 | 0.142 | 0.454 | -9.227; 10.135 | 0.012 | 0.926 |
| Level of education (higher education) | -4.235 | ; 9.809 | 0.099 | 0.434 | 0.503 | -8.374; 9.381 | 0.014 | 0.911 |
| Presence of comorbidity | -2.831 | -6.918;0.173 | 1.257-0.108 | 0.223 | -4.945 | ; 5.391 | 0.007 | 0.932 |
| Practice of physical exercise | 5.306 | 1.305; 9.306 | 0.201 | 0.010 | -5.346 | -10.403; -0.288 | -0.165 | 0.038 |
| Systemic side effects of treatment | -0.287 | -0.399; -0.176 | -0.389 | <0.001 | 0.358 | 0.217; 0.499 | 0.393 | <0.001 |
| Daily tasks | Total Quality of Life score | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | B | 95% CI | B standard | P | B | 95% CI | B standar d | P |
| Constant | 83.895 | 66.419; 101.370 | - | <0.001 | 92.846 | 85.352; 100.341 | - | <0.001 |
| Age | 0.112 | -0.111; 0.335 | 0.083 | 0.323 | 0.02 | -0.076; 0.116 | 0.028 | 0.681 |
| Level of education (high school) | 8.723 | -2.743; 20.190 | 0.194 | 0.135 | -2.526 | ; 7.309 | 0.103 | 0.338 |
| Level of education (higher education) | 5.076 | -5.439; 15.590 | 0.125 | 0.342 | 3.036 | -1.473; 7.545 | 0.145 | 0.185 |
| Presence of comorbidity | -4.894 | -11.015; 1.227 | -0.129 | 0.116 | -0.486 | -3.111; 2.140 | -0.025 | 0.715 |
| Practice of physical exercise | 8.218 | 2.227; 14.208 | 0.217 | 0.008 | 1.281 | -1.288; 3.850 | 0.066 | 0.326 |
| Systemic side effects of treatment | -0.316 | -0.483; -0.149 | -0.297 | <0.001 | -0.348 | -0.419; 0.276 | -0.635 | <0.001 |
All models presented satisfactory parameters. The regression models performed for physical performance, fatigue, and daily tasks were able to explain 25.1%, 21.2%, and 17.2% of the outcome variance, respectively. In these three models, the significant variables for predicting the outcomes were the practice of physical exercise and systemic side effects of the treatment. As a result, it has been observed that the practice of physical exercise increases an average of 5.5 points in the physical performance scores (p=0.01), and also increases an average of 8.2 points in the daily tasks scores (p=0.008) and decreases an average of 5.3 points in fatigue scores (p=0.038). In the model for QoL scores, physical exercise lost significance. On the other hand, treatment side effects showed significance (p<0.001) in all regression models presented.
This study aimed to evaluate the impact of physical exercise on patients that are treating breast cancer. Through the results, it has been found that women who were practicing physical exercise after six months of treatment for breast cancer had better scores for several clinical and QoL domains. Furthermore, it has been possible to observe that the practice of physical exercise is positively associated with the participant's physical performance, daily tasks and fatigue, regardless of age, level of education, presence of comorbidity and treatment side effects.
This study’s findings are aligned with other studies, suggesting that the practice of physical exercises on a regular basis in patients with cancer is beneficial, and can be considered an adjuvant intervention to the treatment for breast cancer.
Fatigue is a common symptom in cancer patients
A study carried out with 28 patients doing chemotherapy and radiotherapy, showed that the intensity and interference of pain in their daily lives decreased after 12 weeks of exercise training. In addition to decreasing pain, the study observed that the amount of oxygen, flexibility and strength increased, showing that physical training is very important and effective during this disease treatment.
In regard to the QoL, pain and fatigue outcomes, it is important to consider the impact of cancer side effects and its treatment, which are quite common in patients with breast cancer.
It is important to consider that the present study has some limitations, including the fact that the sample was selected for convenience in a private hospital, with the study participants having a medium/high socioeconomic level. Other important factors to consider include losses during the treatment and the large number of confounding variables that can impact QoL scores and clinical outcomes, such as cancer staging and the choice of the appropriate treatment plan. For example, it is expected that patients who underwent invasive surgery procedures plus chemotherapy would present a longer recovery than those who underwent hormone therapy only; thus, this can influence QoL. Unfortunately, it has not been possible to control the analyses for these factors, given the wide oncological heterogeneity and treatment combinations (which are planned according to each patient's needs and demands) observed in the sample. On the other hand, this present study has the belief to have minimized the effect of these variables when including the scores of systemic treatment side effects in the analyses. Still, it is important to point out that some parameters, such as pain and fatigue, are subjective to the patient, and as they are a predictive factor. It has been considered the importance of comparing the evolution of parameters in the same patient, at the beginning and after six months of treatment, also relating to the different groups of physical exercise. Another important point to be highlighted is that most correlations found between time of exercise practice and clinical outcomes are weak correlations, although these variables are known as important factors for explaining the quality of life rate. As a strength, the present study has had a significant sample size, the use of international protocols for the outcome evaluation and the prospective design, which allows evaluating the temporality of the factors and outcomes studies herein.
As this is a cohort study where patients were followed up for a period of six months, it can be observed that women who practiced physical exercise during six months after starting treatment for breast cancer, including those who have started exercising after the treatment began, have had better health results. Women who have not done physical exercises and the ones who have stopped exercises during treatment have had the worst results, which may be associated with a higher impact of treatment systemic side effects in this specific group. This present study has found that physical exercise could directly impact both the performance of a healthy routine and aspects of physical performance, daily activities, and fatigue. Also, the longer the duration of physical exercises, the greater the benefits seem to be in the domains of quality of life. This study aims to emphasize the importance of physical exercises as an adjuvant treatment in breast cancer cases. The study suggests a guided practice by a multidisciplinary team always considering the needs and limitations of each patient.
| NMP | Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient |
| JNS | Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing |
| MAF | Collection and assembly of data, Conception and design, Final approval of manuscript, Manuscript writing, Provision of study materials or patient |
| AAC | Collection and assembly of data, Provision of study materials or patient |
| JGM | Hospital Moinhos de Vento, - - Porto Alegre - Rio Grande do Sul-Brazil |
| LAN | Provision of study materials or patient |
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Rev Bras Cancerol. 2022;68 [online]. Available from: <>.
2. Estimativa 2020 - Incidência de câncer no Brasil. Saúde Prevenção e Controle de Câncer. Ministério da Saúde/INCA, 2019.
3. Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA). Câncer de pulmão [Internet]. NCA, 2022.
4. Idorn, M and Straten, PT. Exercise and cancer: from “healthy” to “therapeutic”?. Cancer Immunol Immunother [online]. 2017, vol. 66, p. 667.
5. Matoso, LBBM. Relationship of fatigue with depressive symptoms and level of physical activity in women with breast cancer diagnosis. Rev Bras Cineantr Desemp Hum [online]. 2020, vol. 22, p. 1-14.
6. Binotto, M and Daltoé, T and Formolo, F and Spada, P. Atividade física e seus benefícios na qualidade de vida de mulheres com câncer de mama: um estudo transversal em Caxias do Sul - RS. Rev Bras Atividade Física Saúde [online]. 2016, vol. 21, p. 154.
7. Deminice, R. Physical activity recommendations for cancer prevention and control: a Brazilian consortium. Braz J Oncol [online]. 2022, vol. 18, p. 1-21.
8. Bower, JE. Screening, assessment, and management of fatigue in adult survivors of cancer: an American Society of Clinical Oncology clinical practice guideline adaptation. J Clin Oncol [online]. 2014, vol. 32, p. 1840-50.
9. Ong, WL. A standard set of value-based patient-centered outcomes for breast cancer: The International Consortium for Health Outcomes Measurement (ICHOM) initiative. JAMA Oncol [online]. 2017, vol. 3, p. 677-85.
10. Wirtz, P and Baumann, FT. Physical activity, exercise and breast cancer-what is the evidence for rehabilitation, aftercare, and survival? A review. Breast Care [online]. 2018, vol. 13, p. 93-101.
11. Integr Cancer Ther. 2019;18 [online]. Available from: <>.
12. Eyigor, S and Kanyilmaz, S. Exercise in patients coping with breast cancer: an overview. World J Clin Oncol [online]. 2014, vol. 5, p. 406-11.
13. Chan, RJ and Yates, P and McCarthy, AL. Fatigue self-management behaviors in patients with advanced cancer: a prospective longitudinal survey. Oncol Nurs Forum [online]. 2016, vol. 43, p. 762-71. https://doi.org/10.1188/16.ONF.762-771 Ver referência
14. van Vulpen, JK and Peeters, PHM and Velthuis, MJ and van der Wall, E and May, AM. Effects of physical exercise during adjuvant breast cancer treatment on physical and psychosocial dimensions of cancer-related fatigue: a meta-analysis. Maturitas [online]. 2019, vol. 85, p. 104-11.
15. Köse, E and Aydin, M and Köse, O and Aksu, G and Sekban, G. The efficiency of a mixed exercise program on quality of life and fatigue levels in patients with breast cancer. Rev Assoc Med Bras [online]. 2021, vol. 67, p. 1279-85.
16. Reis, AD. Effect of exercise on pain and functional capacity in breast cancer patients [online]. Available from: <>. Ver referência
17. Aydin, M. The effect of exercise on life quality and depression levels of breast cancer patients. Asian Pacific J Cancer Prev [online]. 2021, vol. 22, p. 725-32.
18. Dieli-Conwright, CM and Orozco, BZ and Dieli, CM. Exercise after breast cancer treatment: current perspectives [online]. Available from: <>. Ver referência
Dados de acesso insuficientes para visualização no mapa.