Tuberculosis (TB) and Lung Cancer (LC) are two important causes of incidence and morbidity and mortality in developing countries. Estimates in the year of 2017 point to about 10 million people affected by TB and about 1,3 million deaths worldwide.
In relation to LC, the World Health Organization (WHO) pointed to the year of 2016 approximately 1,7 million cases diagnosed in the world and in Brazil, for the same period, the estimate was approximately 17,4 thousand new cases in males and 11 thousand in females.
Both TB and LC have clinical presentations that course with consumptive symptoms and radiological findings of pulmonary nodules. Thus, these pathologies constitute important differential diagnoses.
Although the joint occurrence of these two pathologies is rare, about 2%,
Thus, this work describes the case of a patient with epidermoid squamous cell carcinoma developed in tuberculosis infection scar.
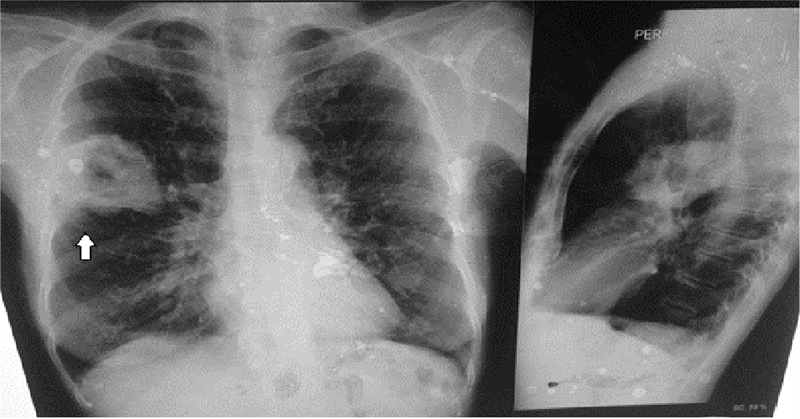
Female of 64-year-old, rural worker, with history of secretive cough for 3 years, associated with unverified fever, especially in the afternoon/night period, of sporadic character and significant weight loss (she could not tell how much). History of active smoking and high smoking burden, using hand-rolled tobacco (1 pack of straw cigarette every two days) for about 45 years. After 2 years with the symptomatology, sought medical attention at the Primary Health Unit, where laboratory tests were requested, which showed no significant changes, bacilloscopy, positive in 3rd sample and chest X-ray with image suggestive of pulmonary tuberculosis (
Figure 1 PA and lateral chest X-ray - Heterogeneous opacity with cavitation in right upper middle lobe (arrow).
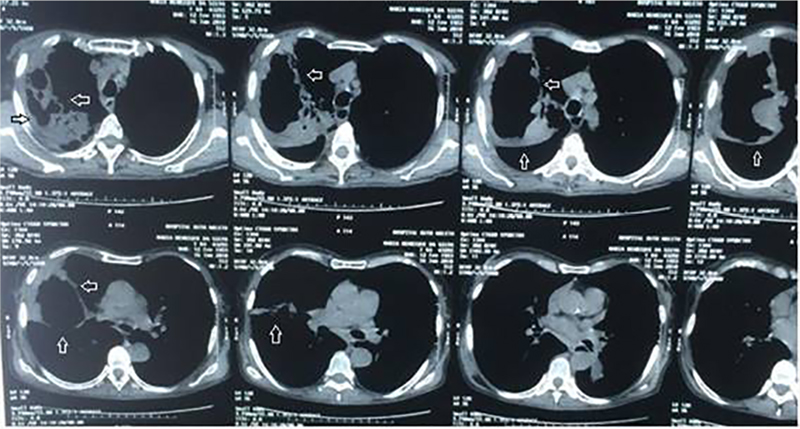
About 1 year later she sought hospital care complaining of chest pain, associated with coughing episodes with elimination of mucosanguinolent discharge and intense adynamia. After symptomatic control and realization of new control chest X-ray and Computed Tomography (CT) of the chest (
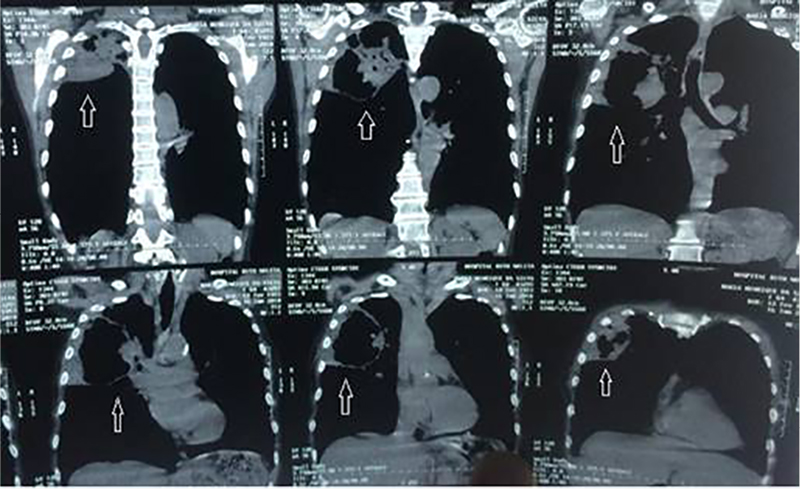
Figure 2A Chest CT coronal view - Large cavity lesion approximately 12cm in diameter, thick and irregular walls, adherent to the right chest wall, with extensive pleural infiltration and liquid content inside, doing hydro level (arrow).
Figure 2B Chest CT transverse - Large cavity lesion approximately 12cm in diameter, thick and irregular walls, adherent to the right chest wall, with extensive pleural infiltration and liquid content inside, doing hydro level (arrow).
Lung cancer is the leading cause of cancer death in Brazil and worldwide, with about 1,3 million deaths a year. Tuberculosis is also an important cause of morbidity and mortality, especially in developing countries.
The explanation for the development of lung cancer in patients with TB is commented by several authors, which state that some reactive oxygen or nitrogen species when released by activated neutrophils, can bind to DNA, inducing genetic damage and, finally, neoplastic transformation.
Silva et al, demonstrated in their study that the moment of diagnosis can be defined in three phases: simultaneous TB and LC, 41,7%; TB before LC, 58,3%; and LC before TB, none case.
The clinical diagnosis of simultaneous occurrence can be difficult, considering that the symptoms and the lesions of TB may mask the diagnosis of lung cancer, thus delaying the diagnosis.
Already radiological diagnosis has been a widely used method to evaluate both TB and LC patients. The chest X-ray is the initial method and CT is the followup method. A benign lesion may present with image of concentric or laminar calcification, diffuse or uniform, central and in “popcorn”. Other types of calcification (eccentric and dotted), when identified, should be considered potentially malignant. When assessing the morphology of nodular lesions, it is observed that most of those, larger than 2cm, constitute malignant nodules. In addition, malignant lesions are often illdefined, irregular and with spiky edges.
Some authors suggest periodic follow-up with chest X-ray, bronchoscopy with biopsy and sputum cytology in patients recently diagnosed with tuberculosis to allow an early diagnosis of lung cancer.
In most of the studies observed, there was a greater association between TB and adenocarcinoma, something different from that reported above, which showed an association with squamous cell carcinoma. Another important factor to highlight is the history of smoking (active or in the past), whereas even after practice control there is still a 2,5-fold increased risk of cancer in TB patients.
From this analysis, it highlights the importance of health actions regarding the orientation of patients diagnosed with tuberculosis regarding exposure to pulmonary carcinoid substances, such as smoking, as well as the adequate treatment of infection with the objective of increasing their overall survival and decrease the impact on public health.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.