Spinal metastases, a relatively common and severe complication of systemic malignancies, significantly impact patients' quality of life and survival. Over the past decades, substantial progress has been made in understanding, diagnosing, and treating this condition. Chemotherapeutic medications for primary cancer control, radiotherapy, and advancements in surgical techniques remain the primary therapeutic modalities.
The prevalence of spinal metastases necessitates a robust diagnostic framework. Sciubba et al.
Surgical intervention remains a cornerstone in managing spinal metastases, particularly in cases of spinal cord compression. A landmark randomized clinical trial by Patchell et al.
Bilsky et al.
More recently, en bloc resection has been better understood. This technique involves the removal of the tumor in a single piece and, while technically demanding, it offers the potential for complete tumor removal, reducing local recurrence rates and improving long-term outcomes.
Radiotherapy is a fundamental modality in managing spinal metastases, particularly for patients who are not surgical candidates. Rades and Abrahm
Prognostic determination is crucial for treatment planning in spinal metastases. Rades et al.
The Neurological, Oncological, Mechanical, and Systemic (NOMS)
The present study aims to evaluate the epidemiological characteristics of patients who underwent surgery for spinal metastases and their functional status up to 90 days postoperatively, to understand and implement the best neurosurgical treatment possible.
This observational and retrospective study was approved by the Ethics Committee of the State University of Londrina under approval number 7.382.258. Medical records of patients treated between March 1, 2022, and August 30, 2024, at the A.C. Camargo Cancer Center were analyzed. The study included patients who underwent surgery for spinal metastases, regardless of age, and examined their clinical status up to 90 days postsurgery. Patients with primary spinal tumors or incomplete medical records were excluded.
The independent variables analyzed were age, sex, histological type of the primary tumor, preoperative functional status evaluated by the Eastern Cooperative Oncology Group (ECOG) scale, American Spinal Injury Association (ASIA) scale for neurological deficits, metastasis location (cervical, thoracic, or lumbar), and type of surgery performed (decompression, decompression with arthrodesis, arthrodesis). Outcome variables assessed based on medical records up to 90 days postoperatively included: ECOG, ASIA, neurological sequelae, neurological improvement, and mortality.
The data were analyzed using the Stata 13 (StataCorp LLC.) software, employing the Chi-squared tests for categorical variables and the Student's t-test for numerical variables.
The final analysis, after applying exclusion criteria, included 35 patients (20 males and 15 females). The mean patient age was 57 ± 13 years (
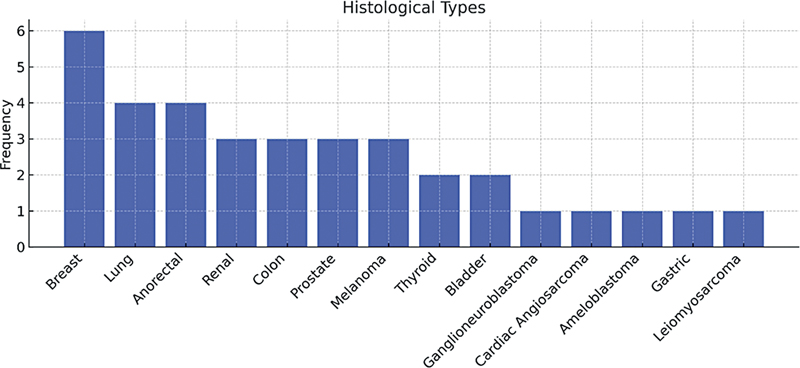
Fig. 1 Primary histological types of spinal metastases analyzed.
| Variable | N (%) |
|---|---|
| Age, years | 57 ± 13 |
| Sex | |
| Male | 20 (57) |
| Female | 15 (43) |
| Histological type | |
| Breast | 6 (17) |
| Lung | 4 (11) |
| Anorectal | 4 (11) |
| Melanoma | 3 (8.5) |
| Renal | 3 (8.5) |
| Colon | 3 (8.5) |
| Surgical procedure | |
| Decompression | 1 (2.86) |
| Percutaneous arthrodesis | 1 (2.86) |
| Decompression and arthrodesis | 33 (94.29) |
| Outcome | |
| Death | 8 (22.86) |
| Sequelae | 6 (17.14) |
| Neurological improvement | 21 (60) |
| Cause of death | |
| Sepsis | 6 (75) |
| Thromboembolism | 1 (12.5) |
| Hemorrhagic shock | 1 (12.5) |
Most patients (94.2%) underwent extensive spinal canal decompression followed by fixation via arthrodesis (anterior, posterior, or combined approach), as shown in
| Operated level | N (%) | |
|---|---|---|
| Cervical | 6 (17.4) | |
| Thoracic | 18 (51.4) | |
| Lumbar | 7 (20.00) | |
| Multiple levels | 4 (11.43) |
A mortality rate of 22% was observed among the patients evaluated at 90 days after surgery, with sepsis being the leading cause of death. Other immediate causes of death included pulmonary thromboembolism and hemorrhagic shock, though at lower proportions. Regarding outcomes, 60% of patients showed some degree of neurological improvement, while 17% maintained their preoperative neurological sequelae (
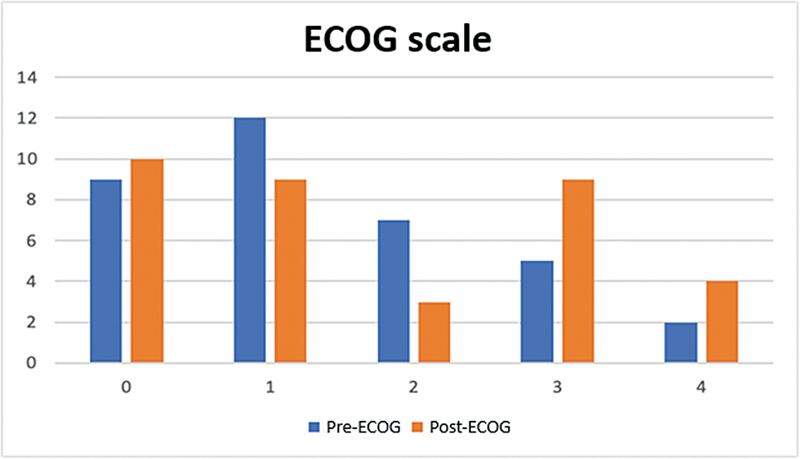
The 90-day postoperative mortality rate was of 22.86%, with sepsis as the leading cause of death (75%). Neurological improvement was observed in 60% of patients, whereas 17% maintained preoperative neurological deficits. Despite neurological recovery, ECOG scores (
Fig. 2 Pre- and postoperative ECOG classification: 0 - Fully preserved functionality; 1 - Symptoms of the disease present, but ambulatory and capable of self-care; 2 - Out of bed for more than 50% of the time; 3 - Confined to bed for more than 50% of the time and requires assistance with daily activities; 4 - Completely bedridden, requiring continuous assistance.
The data obtained from the analysis of 35 patients who underwent surgery for spinal metastases provide important insights into the neurosurgical management of this condition, as well as its outcomes. The mean patient age of 57 years, with a predominance of males (57%), is consistent with the literature, which indicates a higher prevalence of metastases in middle-aged to elderly patients, reflecting the increased incidence of primary neoplasms in this age group.
The primary histological types of metastases, notably breast (17%), lung (11%), and anorectal (11%) cancer, align with other studies that identify them as the most common sources of vertebral metastases.
The widespread use of decompression combined with arthrodesis (94.2%) reflects the standardization of a surgical approach aimed at restoring spinal stability and alleviating spinal cord compression.
Despite the complexity of the procedure, the 90-day mortality rate was 22.86%, with sepsis being the leading cause of death (75%). This underscores the importance of rigorous postoperative infection management, as well as careful screening to identify patients at higher risk for systemic complications.
Neurological outcomes showed significant improvement in most cases, with 60% of patients progressing on the ASIA scale,
While the results are encouraging, the lack of statistical significance (p > 0.05) in the evaluated parameters limits more robust conclusions. A small sample size and heterogeneity of the group may have contributed to this limitation. Future studies with larger cohorts and longer follow-ups are needed to validate these findings and explore additional prognostic factors, such as the impact of adjuvant therapies on surgical outcomes. Despite the limitations of this research, future studies with more robust approaches can complement our findings.
Significant advances have been made in understanding and treating spinal metastases, driven by improved diagnostics and therapeutic strategies. Multidisciplinary approaches, early diagnosis, and ongoing research are critical to optimizing patient outcomes. Decompression and arthrodesis surgery remain the gold standard, for most cases, to enhance neurological prognosis. However, functional deterioration due to underlying disease progression remains a significant challenge.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Sciubba, D M and Gokaslan, Z L. Diagnosis and management of metastatic spine disease. Surg Oncol [online]. 2006, vol. 15, p. 141-151. https://doi.org/10.1016/j.suronc.2006.11.002 Ver referência
2. Patchell, R A and Tibbs, P A and Regine, W F and Payne, R and Saris, S and Kryscio, R J. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet [online]. 2005, vol. 366, p. 643-648. https://doi.org/10.1016/S0140-6736(05)66954-1 Ver referência
3. Bilsky, M H and Boakye, M and Collignon, F and Kraus, D and Boland, P. Operative management of metastatic and malignant primary subaxial cervical tumors. J Neurosurg Spine [online]. 2005, vol. 2, p. 256-264. https://doi.org/10.3171/spi.2005.2.3.0256 Ver referência
4. Fourney, D R. En bloc resection of primary and metastatic tumors of the cervical spine: classification, technique, and outcomes. Spine [online]. 2003, vol. 28, p. E375-E387.
5. Rades, D and Abrahm, J L. The role of radiotherapy for metastatic epidural spinal cord compression. Nat Rev Clin Oncol [online]. 2010, vol. 7, p. 590-598. https://doi.org/10.1038/nrclinonc.2010.137 Ver referência
6. Rades, D and Dunst, J and Schild, S E. The first score predicting overall survival in patients with metastatic spinal cord compression. Cancer [online]. 2008, vol. 112, p. 157-161. https://doi.org/10.1002/cncr.23150 Ver referência
7. Laufer, I and Rubin, D G and Lis, E and Cox, B W and Stubblefield, M D and Yamada, Y and Bilsky, M H. The NOMS framework: approach to the treatment of spinal metastatic tumors. Oncologist [online]. 2013, vol. 18, p. 744-751. https://doi.org/10.1634/theoncologist.2012-0293 Ver referência
8. Cole, J S and Patchell, R A. Metastatic epidural spinal cord compression. Lancet Neurol [online]. 2008, vol. 7, p. 459-466. https://doi.org/10.1016/S1474-4422(08)70089-9 Ver referência
9. Araujo, J LV and Veiga, J CE and Figueiredo, E G and Barboza, V R and Daniel, J W and Panagopoulos, A T. Management of metastatic spinal column neoplasms - an update [Manejo das neoplasias metastáticas da coluna vertebral - uma atualização]. Rev Col Bras Cir [online]. 2013, vol. 40, p. 508-513. https://doi.org/10.1590/S0100-69912013000600015 Ver referência
10. Van den Brande, R and Cornips, E MJ and Peeters, M and Ost, P and Billiet, C and Van de Kelft, E. Epidemiology of spinal metastases, metastatic epidural spinal cord compression and pathologic vertebral compression fractures in patients with solid tumors: A systematic review. J Bone Oncol [online]. 2022, vol. 35, p. 100446. https://doi.org/10.1016/j.jbo.2022.100446 Ver referência
11. Jaipanya, P and Lertudomphonwanit, T and Chanplakorn, P and Pichyangkul, P and Kraiwattanapong, C and Keorochana, G and Leelapattana, P. Predictive factors for respiratory failure and in-hospital mortality after surgery for spinal metastasis. Eur Spine J [online]. 2023, vol. 32, p. 1729-1740. https://doi.org/10.1007/s00586-023-07638-z Ver referência
12. International Standards Committee of ASIA and ISCoS. Updates of the International Standards for Neurologic Classification of Spinal Cord Injury: 2015 and 2019. Phys Med Rehabil Clin N Am [online]. 2020, vol. 31, p. 319-330. https://doi.org/10.1016/j.pmr.2020.03.005 Ver referência
13. Rodrigues, L M and Valesin Filho, E S and Ueno, F H and Fujiki, E N and Milani, C. Quality of life of patients submitted to decompression for metastatic vertebral lesion [Qualidade de vida de pacientes submetidos à descompressão por lesão vertebral metastática]. Acta Ortop Bras [online]. 2011, vol. 19, p. 149-153. https://doi.org/10.1590/S1413-78522011000300007 Ver referência
Dados de acesso insuficientes para visualização no mapa.