Pancreatic cancer is responsible for about 2% of all cancers diagnosed and 4% of all deaths in Brazil due to this pathology. Among all subtypes of pancreatic tumors, the most prevalent is adenocarcinoma (originating in glandular tissue), corresponding to 90% of the cases diagnosed.[
As a result of its difficult early detection, associated with the aggressive behavior of such a tumor, pancreatic cancer presents a significant mortality rate, with a five-year survival rate of about 2% to 9%,[
The main risk factors identified for pancreatic cancer are, in addition to advanced age, male sex, afro-descendant ethnicity, smoking, obesity, long-standing diabetes, pancreatitis and excessive alcohol use. Also, several genetic syndromes are associated with an increased risk of developing pancreatic neoplasia, such as hereditary pancreatitis, hereditary non-polypoid colorectal cancer (HNPCC), hereditary breast and ovary cancer (associated with BRCA2 mutations), familial atypical multiple melanoma syndrome, Peutz-Jeghers syndrome, ataxia-telangiectasia and von Hippel-Lindau syndrome.[
Considering the prevalence and aggressiveness of this disease, the present study intends to evaluate the epidemiology of pancreatic cancer in a tertiary hospital in the northwest of Rio Grande do Sul, Brazil. It is expected that with the analysis of these data mechanisms of intervention may be created, aiming both prevention and early diagnosis of this pathology, enabling patients to be properly identified and treated when affected.
This article aims to analyze the evolution of the analytical and non-analytical cases of pancreatic cancer registered in epidemiological surveillance of neoplasms system of a tertiary hospital in the northern state of Rio Grande do Sul, in a time frame of ten years. Also, it aims to describe the prevalence of pancreatic cancer in this decade, as well as to characterize the cases according to the demoGraphic and clinical profile of the patients. Furthermore, verify which variables related to diagnosis, treatment and staging are associated with the cases, and identify the main risk factors associated with the reported cases.
A retrospective cross-sectional, predominantly descriptive study was carried out using data provided by medical records and a hospital registry of patients identified as having pancreatic cancer at São Vicente de Paulo Hospital (HSVP), among the years of 2007 and 2017.
HSVP is located in the interior of the state of Rio Grande do Sul and is a highly complex tertiary hospital with more than 700 hospital beds. The municipality contains approximately 200,000 inhabitants and is a regional health reference for the states that make up the southern region of the country.
After ethic approval issued by both the Ethics Committee of the HSVP and the Ethics Committee of the University of Passo Fundo, registered as protocol number 3,095,106, information based on medical records and the hospital registry for pancreatic cancer was consulted, and later on, used to elaborate a database.
The inclusion criteria of the study were analytical cases of malignant pancreatic neoplasia (CID 10 - C25) included in the HSVP registers from January 2007 to December 2017. The analytical cases represented patients with malignant neoplasia, whose planning and treatment of the tumor followed the indication of hospital guidelines or were executed, as well as its follow-up, according to its guidelines. Therefore, those patients were considered appropriate for later on analysis of the quality of care provided by the hospital.
Cases excluded from the study included benign analytical cases, analytical cases that had a pending or incomplete diagnostic status, multiple records.
The variables analyzed by the study were sex, age, ethnicity, family history, history of smoking and alcohol consumption, previous diagnoses of neoplasia, diagnosis base, primary tumor location, initial clinical staging, TNM staging, metastasis location, first treatment performed in the hospital, staging at the end of the first treatment, presence of more than one tumor and time of survival.
Statistical analysis was performed using the statistical software IBM Statistical Package for Social Sciences (SPSS), version 18.0, (SPSS Inc, Chicago, IL, USA), in a descriptive and inferential manner for the study variables.
For qualitative variables, the chi-square test was applied and, for the quantitative, the T-student test. To verify the independence between the variables that were associated or not to the outcome, a non-parametric test with a significance level of 5% was used.
Among the 445 medical records analyzed, the results were categorized into the following variables: risk factors associated with the development of pancreatic neoplasia (gender, age, ethnicity, family history, smoking and alcoholism), evaluation at diagnosis (diagnosis, or previous treatments, presence of other primary tumors, TNM classification and initial staging of the disease), the treatment used (first hospital treatment) and the evolution of the pathology (localization of distant metastases), state of the patient after the first phase of treatment, survival time, deaths occurred).
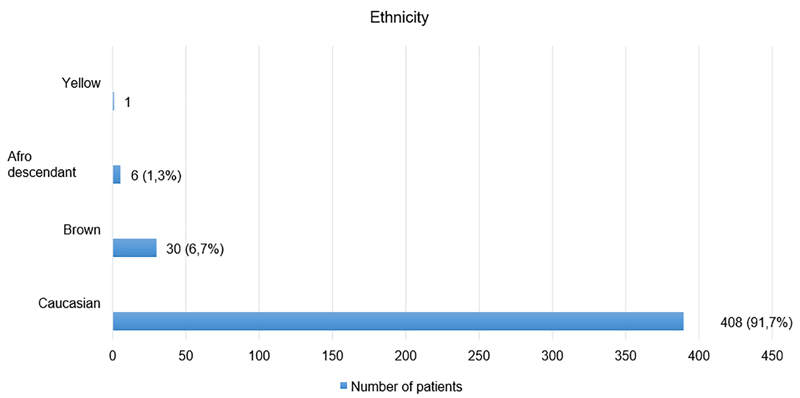
Regarding associated risk factors, 228 patients were males (51.2% of the total sample), remaining 217 (48.8%) of the female sex. Mean age and ethnicity can be verified in
Graph 1 Ethnicity. *The prevalent ethnicity in the study was caucasian.
| Age | Total Of Patients | Percentage (%) |
|---|---|---|
| 13 | 1 | 0,2 |
| 13 TO 45 | 19 | 4 |
| 46 TO 55 | 62 | 13,9 |
| 56 TO 65 | 130 | 29,2 |
| 66 TO 80 | 187 | 41,9 |
| 81 TO 96 | 47 | 10,5 |
| 96 | 1 | 0,2 |
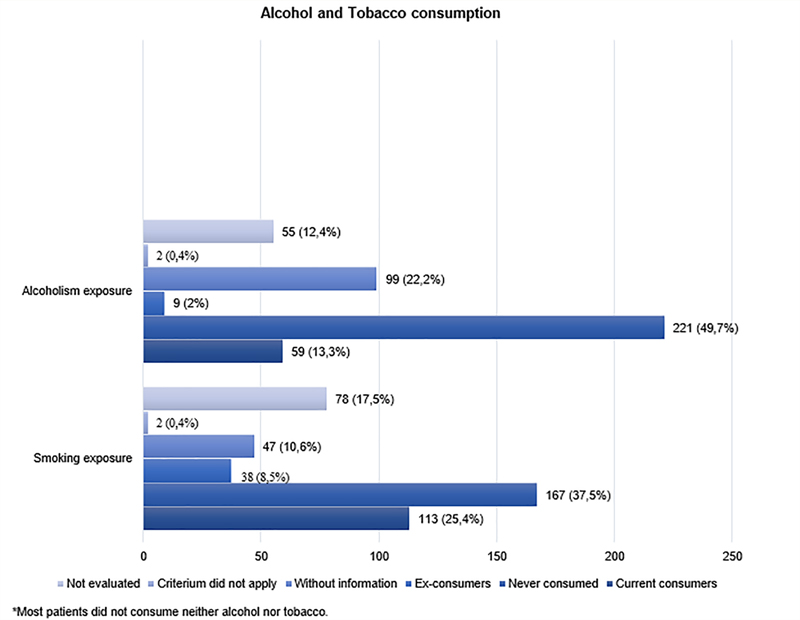
Information regarding the existence of a family history of pancreatic neoplasia was present in only 202 of them (45.4% of the sample). Of those, only 63 (14.2%) had a positive family history, while 139 (31.2%) had a negative family history. As other risk factors, data concerning smoking and alcohol exposure can be seen in
Graph 2 Alcohol and tobacco consumption. *Most patients did not consume neither alcohol nor tobacco.
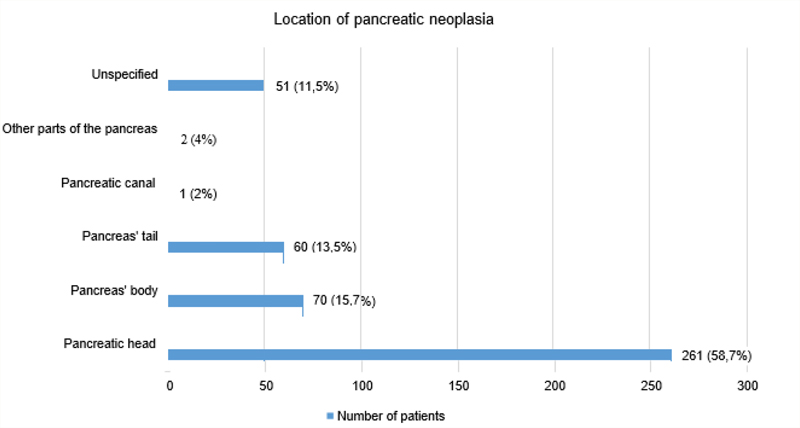
The main sites of tumor location in the pancreas can be seen in
Graph 3 Location of pancreatic neoplasia. *Pancreatic head was the most common site of the tumor.
Regarding the methodology used for the diagnosis, 238, that is, 53.5% of the patients had their diagnosis through histology of the primary tumor; 109 (24.5%) through histology of metastasis; and 88 (19.8%) employing image examination. The other diagnostic methods (tumor markers, cytology, clinical research and clinical diagnosis) obtained, together, 2.2%. However, of the 445 patient charts analyzed, 337 patients (75.7%) had no previous diagnosis and did not have any treatment, and a sample of 89 patients (20.0%) were already diagnosed, but without previous treatment. Only 19 patients (4.3%) had a previous diagnosis and treatment.
Regarding the occurrence of more than one primary tumor, 405 (91%) had no more than one tumor and 40 (9%) had another associated tumor.
Initial staging of the neoplasia can be verified at
| Inicial Cancer Staging | Number Of Cases | Total Percentage (%) |
|---|---|---|
| IA | 11 | 2,5 |
| IB | 21 | 4,7 |
| IIA | 16 | 3,6 |
| IIB | 10 | 2,2 |
| III | 46 | 10,3 |
| IV | 200 | 44,9 |
| No data | 141 | 31.7 |
| Total | 445 | 100,0 |
Regarding the first hospital treatment used in such cases of pancreatic neoplasia, data can be observed in
| First Hospital Treatment | Total Of Patients | Percentual (%) |
|---|---|---|
| Any one | 82 | 18,4 |
| Surgery alone | 153 | 34,4 |
| Surgery plus radiotherapy | 1 | 0,2 |
| Surgery plus radiotherapy plus chemotherapy | 2 | 0,4 |
| Surgery plus Chemotherapy | 47 | 10,6 |
| Surgery plus Chemotherapy and other treatments | 5 | 1,1 |
| Surgery and other treatments | 13 | 2,9 |
| Surgery back surgery and other treatments | 2 | 0,4 |
| Surgery plus Chemotherapy and other treatments | 2 | 0,4 |
| Complementary treatments | Total of patients | Percentual (%) |
|---|---|---|
| Surgery and then other treatments | 1 | 0,2 |
| Only radiotherapy | 7 | 1,6 |
| Radiotherapy and chemotherapy | 2 | 0,4 |
| Radiotherapy plus chemotherapy and other treatments | 1 | 0,2 |
| Only chemotherapy | 49 | 11 |
| Chemotherapy and radiotherapy | 2 | 0,4 |
| Surgery plus radiotherapy and other treatments | 1 | 0,2 |
| Chemotherapy and other treatments | 14 | 3,1 |
| Only hormone therapy | 1 | 0,2 |
| Hormone therapy and chemotherapy | 1 | 0,2 |
| Only alternative sources of treatment | 50 | 11,2 |
| Alternative sources of treatment and chemotherapy | 6 | 1,3 |
| Alternative sources of treatment plus chemotherapy and other treatments | 2 | 0,4 |
| Alternative sources of treatment plus other treatments and then chemotherapy | 1 | 0,2 |
Regarding the main sites of distant metastasis, 215 (48.3%) of the 445 patients were evaluated. The other 230 patients did not develop metastases or these were not shown in their medical records. According to our study, the organ most likely to receive pancreatic metastasis was the liver, corresponding to 134 (62.3%). Out of the 134 patients, 84 of these (39%) had metastasis located only in the liver. The other 50 patients had metastasis in at least one other site, the main ones being: peritoneum, with 32 cases (14.9%), and lungs with 11 cases (5.1%).
Excluding the liver, the other main sites of metastasis were the peritoneum, with 82 cases (38.1%), of which only 45 (20.9%) were found in the peritoneum alone; and the lungs, with 25 cases (11.6%). Only 10 (4.6%) were strictly located in the lungs. Other organs affected by pancreatic metastasis were: stomach, small intestine, colon, biliary tract, mediastinum, bones, skin, brain, adrenals and lymph nodes.
Regarding the number of affected sites, 156 (72.5%) patients had only one site of metastasis, 49 (22.8%) had 2 sites, 9 (4.2%) had 3 sites and 1 (0.5 %) patients had 4 sites affected.
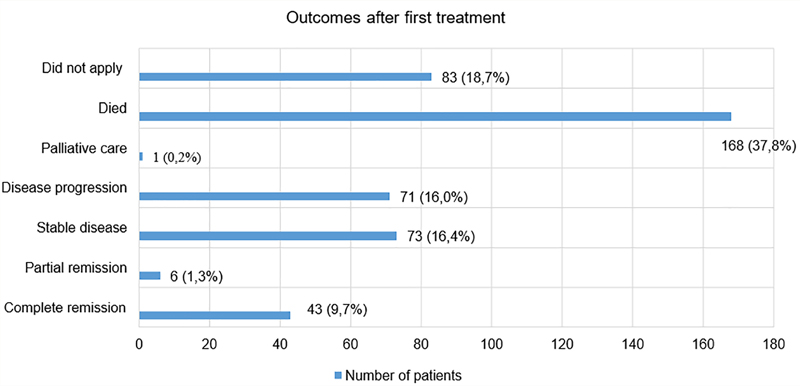
After undergoing first treatment for pancreatic cancer, 43 (9.7%) were in complete remission, and 168 (37.8%) died. More results obtained after undergoing fist treatment for pancreatic cancer can be observed in
Graph 4 Outcomes after first treatment. *Most patients showed poor outcomes after first treatment.
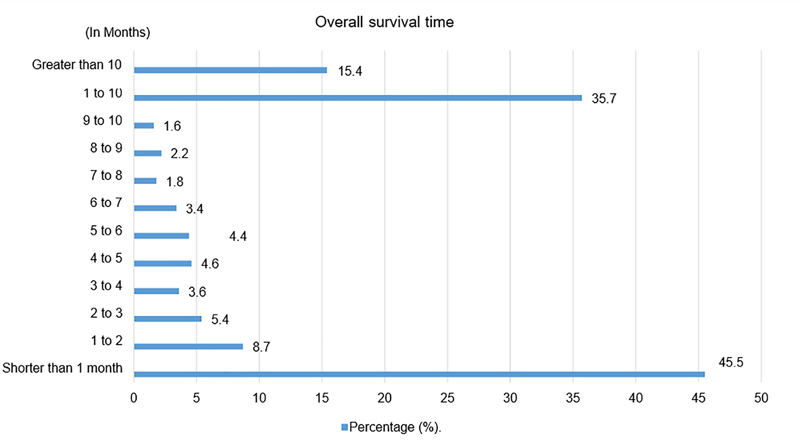
Regarding overall survival time, among the 445 files analyzed, 45.50% of the patients had a survival shorter than 1 month, as verified in
Graph 5 Overall survival. *Most patients died in a period shorter than a month.
The present study shows results that need to be discussed to better understand the factors that permeate and influence the aggressive behavior and unfavorable prognosis that pancreatic cancer presents.
When a family history of pancreatic neoplasia is assessed, it is made by analyzing the involvement of two first-degree relatives. The study, however, considered as family history any pancreatic neoplasia that has occurred in a first-degree relative. Several literature[
The research, unlike data proposed by previous studies,[
Advanced age is an important non-modifiable risk factor for pancreatic cancer. In Brazil, pancreatic cancer is a rare entity when diagnosed before the age of 30 years, and it is more common to be diagnosed after the age of 60 years. Globally, about 90% of pancreatic cancer cases are diagnosed after age 55, varying in some countries. In the United States, the disease is more prevalent at 60 years of age and, in India, it becomes more frequent after 50 years of age.[
The prevalence of pancreatic cancer varies according to ethnicity. Previous epidemiological data indicate that a higher percentage of this diagnosis occurs in African Americans, rather than in caucasian individuals (15.8 vs 12.0 per 100,000).[
However, this statement is not the only that applies, since there is also evidence of genetic association and underlying environmental gene alterations to explain at least some of the observed differences in incidence and prevalence among ethical groups.[
Another non-modifiable risk factor is gender, with pancreatic cancer being more common in men than in women.[
In comparison, Brazil has the following incidence rates: 5.3 per 100.00 for men and 4.1 per 100,000 for women. Worldwide, the incidence for men is 5.5 per 100,000 and 4.0 per 100,000 for women. Hence, it is observed that the Brazilian incidence rates of pancreatic cancer follow a worldwide trend and are consistent with the country's demoGraphic situation,[
Finally, there are studies that try to explain the numbers as mentioned earlier; however, it is suspected that the risks for pancreatic cancer are slightly increased in men due to environmental factors such as tobacco.[
As for alcoholism, the information collected showed a low rate of heavy drinkers, and it can be inferred that there is no well stablished correlation between the development of the disease and alcoholism. This information is well provided by the International Agency for Research on Cancer, whose conclusion is that there is no evidence to state that the risk of consumption can lead to the appearance of a pancreatic neoplasm.[
Currently, population screening for pancreatic cancer is not recommended in Brazil because there is no scientific evidence to prove benefit in tracking the disease. In populations with higher risk for the development of pancreatic cancer, as carriers of syndromes, it is possible to adopt screening strategies in investigative protocols. Besides, the vast majority of patients with pancreatic cancer only present signs and symptoms of the disease in more advanced stages, at which point they have their first diagnosis.[
Because many are asymptomatic, and those with clinical symptoms usually present them as nonspecific, early diagnosis is a challenging subject regardingp ancreatic cancer. More specific symptoms include weight loss, jaundice, malabsorption, pain, dyspepsia and nausea.[
Nevertheless, magnetic resonance imaging (MRI) is reserved for cases in which CT is inconclusive, such as presentation of isodense tumors.[
When evaluating tumor markers, CA-19-9 is the most widely used and best validated marker for pancreatic cancer. However, it should be used with caution since it is nonspecific, and can be altered in other benign conditions.[
In the present study, the methods that provided the greatest number of diagnoses among the charts were histology of primary tumor and metastasis, and imaging methods. Tumor marker, cytology, clinical, and clinical research scored only 2.2% of the diagnosis, being the least used for that purpose. The percentage of use of these diagnostic methods corroborate with rates described in previous studies.
Moreover, the study estimated that 9% of patients had more than one primary tumor. It is estimated that the frequency of more than one primary tumor ranges from 2 to 17%,[41] without necessarily being related to the pancreatic neoplasm. This can be explained because many habits and substances that are risk factors for pancreatic cancer are also present as risk factors in different types of tumors. Also, genetic syndromes may imply on that percentage, since they are often associated with more than a single tumor.
The pancreas is an organ that is placed in the upper portion of the abdomen. It is anatomically divided into parts called head, body and tail[
Regarding the anatomical location of the primary tumor, approximately 60-70% are found in the head of the pancreas, the rest being found in the body and tail, respectively.[
The TNM system is a tool for the staging in different types of cancer. This staging tool determines that T is assigned for tumor, N for lymph nodes and M for metastasis. The literature focuses on tumor staging, which uses TNM to be constructed, and can range from 80 to 85% of the tumors as locally advanced or metastatic[
Once a tumor is diagnosed, the patient's assessment begins by defining the stage the patient is in and planning their treatment. Because pancreatic tumors usually take time to manifest symptoms and are difficult to diagnose, the vast majority are only diagnosed in stages III or IV. That is, tumors with large local or metastatic invasion.[
In addition, the present study showed that 15.1% of patients were diagnosed in stage III and 65.8% in stage IV. This leads us to think that perhaps the diagnosis of pancreatic tumors in this particular center is taking longer than in other medical centers previous studies were conducted, causing the tumors to be diagnosed at more advanced stages. This can occur for several reasons, some of them being: the search for late medical care by the patient, less access to high-tech diagnostic equipment and accuracy, or even delays in the referral of the universal health system from the beginning of the investigation of the symptoms until its diagnosis.
The investigation of the existence of distant metastases after the diagnosis of a neoplasm always consists in procedures of extreme importance, since its presence already places the patient automatically in stage IV of the TNM, which affects the conducts and treatments that can be offered to that patient. When we refer to pancreatic cancer, the main sites to be investigated, as they are the most prevalent to present metastases, are: liver, peritoneum and lungs.[
The survival rate of pancreatic cancer is still low and the prognosis of this disease is reserved. According to consulted data, the 5-year overall survival rate is between 5%[
Treatment of pancreatic cancer varies according to its histological type, staging and general evaluation of the patient. It is usually subdivided into three groups. The first would be for patients with potentially resecTable, localized cancer. The second group includes the unresecTable patients and the third group, the metastatic patients. This way, several treatments can be performed.[
Even so, surgical resection is the only treatment that offers a potential cure for pancreatic cancer.[
Other treatment modalities include radiation therapy, chemotherapy and immunotherapy. Studies have shown that adjuvant chemotherapy combined with radiotherapy have demonstrated greater survival rates over isolated chemotherapy. Isolated radiotherapy is used as a treatment, most of the time, to alleviate symptoms and prolong the survival of patients whose tumors cannot be resected. Another modalities available for treatment of pancreatic cancer are hormone therapy or immunotherapy, but no significant tumor benefits have been demonstrated.[
After the approach of first treatment for pancreatic cancer, our study showed that 43 patients, (9.7%), were in complete remission; 6 (1.3%) were in partial remission, 73 (16%) in sTable disease, 71 (16.0%) in progressing disease, 1 (0.2%) in cancer support therapy, 168 (37.8%) died and 83 (18.7%) did not apply for the criteria. Generally, no data is available in this section regarding pancreatic neoplasms. There are some reports arranged according to this categorization, but they include all forms of cancer. Thus, these results could not match basis for comparison.
Pancreatic cancer is recognized as a neoplasm with a high mortality rate, which represents 4% of cancer deaths in Brazil, although it represents only 2% of diagnosed cancers.[
Based on the data obtained, the epidemiological surveillance of pancreatic cancer in the north region of the State of Rio Grande do Sul demonstrated a higher prevalence of pancreatic cancer in caucasian men, especially older than 56-years-old. The most common primarily location of the tumors was the pancreatic head, and, the main sites of metastasis were the liver, peritoneum and lungs.
Prognosis regarding the sample was not favorable, since most patients were diagnosed with metastatic tumors (stage IV). Most of the patients underwent surgery, followed or not by other treatments, and a high lethality rate was later observed.
Therefore, the results obtained with the present study can conclude that pancreatic cancer, in the north region of Rio Grande do Sul has similar epidemiological features as those already observed in international literature, with the exception of ethnicity. Late diagnosis contributes to the aggressive behavior of this disease, and to low overall survival rates.
These findings suggest the need for further studies concerning pancreatic neoplasm, that may be relevant for future adoption of preventive and diagnostic measures and which could modify perspectives regarding prognosis of the disease.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.