Lung cancer is the most common cancer in the world, with projected 2 million incident cases and 1.7 million deaths in 2016, according to the 2016 Global Burden of Disease Analysis (Tracheal, Bronchus, and Lung Cancer Group).[
The development of epidermal growth factor receptor (EGFR)-targeted tyrosine kinase inhibitors (TKI) resulted in significant clinical improvements for patients with EGFR mutations (EGFRm) - 10-15% of NSCLC patients in Western high-income countries and 30-40% in Asia.[
Even with high response rates among those patients (50-80% versus less than 30% with conventional chemotherapy), they eventually present acquired resistance with disease progression after 9-13 months.[
Osimertinib is an oral, potent, selective, irreversible inhibitor of both EGFR-TKI sensitizing and resistance mutations in NSCLC with a significant selectivity margin over wild-type EGFR. The efficacy and safety of osimertinib in advanced NSCLC patients previously treated with first-generation EGFR-TKI and with acquired EGFR T790M mutation was assessed in several clinical trials. In the phase I, dose-escalation
AURA trial,[
Thus, the primary objective of this study was to describe the efficacy and safety of single agent osimertinib in a real world setting in adult Brazilian patients with advanced or metastatic EGFR T790M mutation-positive NSCLC, who have progressed after prior EGFR-tyrosine kinase inhibitor (TKI) therapy.
ASTRIS (NCT02474355)[
Adult patients (aged 18 years or older) with locally advanced (stage IIIB) or metastatic (stage IV) NSCLC with confirmed T790M mutation on tissue or plasma samples, who have received prior EGFR-TKI therapy were enrolled. Other inclusion criteria included:
i) Provision of signed and dated written informed consent; ii) World Health Organization (WHO) performance status 0-2; iii) Adequate bone marrow reserve and organ function as demonstrated by complete blood count, biochemistry in blood and urine at baseline; iv) ECG recording at baseline showing absence of any cardiac abnormality; v) Female patients of childbearing potential must be using adequate contraceptive measures, must not be breast feeding, and must have a negative pregnancy test prior to start of dosing; or they must have evidence of non-childbearing potential; vi) Male patients must be willing to use barrier contraception. Exclusion criteria were:
i) Previous (within 6 months) or current treatment with osimertinib; ii) Patients currently receiving any treatment known to be potent inhibitors or inducers of cytochrome P450; iii) Any evidence of severe or uncontrolled systemic diseases, including uncontrolled hypertension, active bleeding diatheses, active infection including hepatitis B, hepatitis C and human immunodeficiency virus, or significantly impaired bone marrow reserve or organ function, including hepatic and renal impairment, which in the investigator's opinion would significantly alter the risk/benefit balance; iv) Patient with symptomatic central nervous system (CNS) metastases who is neurologically unstable or has required increasing doses of steroids to manage CNS symptoms within the 2 weeks prior to start study drug administration; v) Past medical history of Interstitial Lung Disease (ILD), drug-induced ILD, radiation pneumonitis requiring steroid treatment, or any evidence of clinically active ILD; vi) Any of the following cardiac criteria: mean resting corrected QT interval (QTcF) > 470ms using Fredericia's formula, any clinically important abnormalities in rhythm, conduction or morphology of resting ECG, any factors that increase the risk of QTc prolongation or risk of arrhythmic events; vii) Any unresolved toxicity from prior therapy CTCAE > grade 3 at the time of starting treatment; viii) History of hypersensitivity to excipients of osimertinib or to drugs with a similar chemical structure or class.
All patients signed informed consent form before any trial procedure and the trial was approved by local Ethics Committee of each participating site.
Data collected included demographics, variables related to eligibility criteria (medical history, past and current disease characteristics, and tumor EGFR mutational status), osimertinib exposure (starting dose, dose adjustments and discontinuations), investigator-reported efficacy (including tumor response and disease progression), overall survival (OS), and safety (including serious adverse events [SAEs] and adverse events leading to dose modification).
Data presented here refers to the subset of Brazilian patients (n=88) enrolled to participate in the ASTRIS trial. The cutoff was October 20th, 2017. Data was examined for the full Brazilian analysis set. Descriptive statistics was used for all variables, as appropriate. Continuous variables were summarized by the number of observations, mean, standard deviation, median, minimum and maximum. Categorical variables were summarized by frequency counts and percentages for each category. Progressionfree survival (PFS) was summarized using KaplanMeier estimates of the median time progression and quartiles together with their 95% confidence intervals.
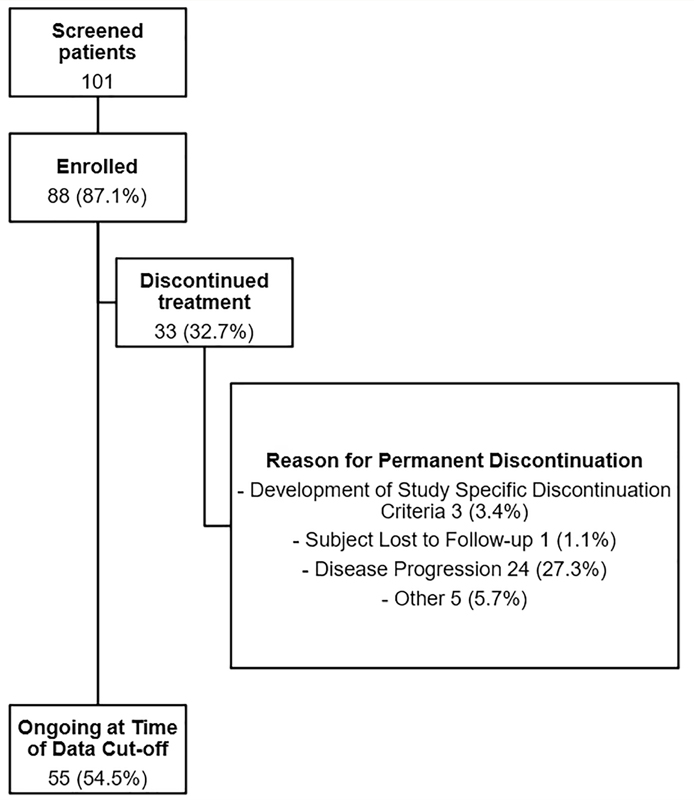
A total of 88 patients from 14 different Brazilian sites were included in this analysis. Patients' disposition is depicted in
Figure 1 Patient disposition flowchart.
| Characteristic | N (%) |
|---|---|
| Sex - female | 58 (65.9) |
| Age, years (mean [standard deviation]) | 63.6 [11.6] |
| Self-reported ethnicity White | 69 (78.4) |
| Black | 7 (8.0) |
| Asian | 7 (8.0) |
| Other | 5 (5.7) |
| WHO Performance Status 0 - Normal Activity | 22 (25.0) |
| 1 - Restricted Activity | 55 (62.5) |
| 2 - In Bed Less Than or Equal to 50% of the Time | 11 (12.5) |
| 3 - In Bed More Than 50% of the Time | 0 (0.0) |
| 4 - 100% Bedridden | 0 (0.0) |
| ECG results Normal | 56 (63.6) |
| Abnormal | 32 (36.4) |
| Clinically relevant (n=32) | 1 (3.1) |
| Receptor status (positivity)† T790M | 88 (100.0) |
| G719X | 2 (2.3) |
| EXON 19 Deletion | 55 (62.5) |
| S768I | 3 (3.4) |
| EXON 20 Insertion | 2 (2.3) |
| L858R | 24 (27.3) |
| Known Brain and Leptomeningeal Metastasis Any lesion present | 25 (31.8) |
| Brain Metastases Only (n=25) | 22 (25.0) |
| Leptomeningeal Disease Only (n=25) | 1 (1.1) |
| Both Brain and Leptomeningeal (n=25) | 2 (2.3) |
| Previous EGFR-TKI Erlotinib | 54 (61.4) |
| Gefitinib | 42 (47.7) |
| Afatinib | 3 (3.4) |
Type of sample tested: Tissue (35.2%), Blood (63.6%), and FNA/Cytology (1.1%); WHO: World Health Organization.
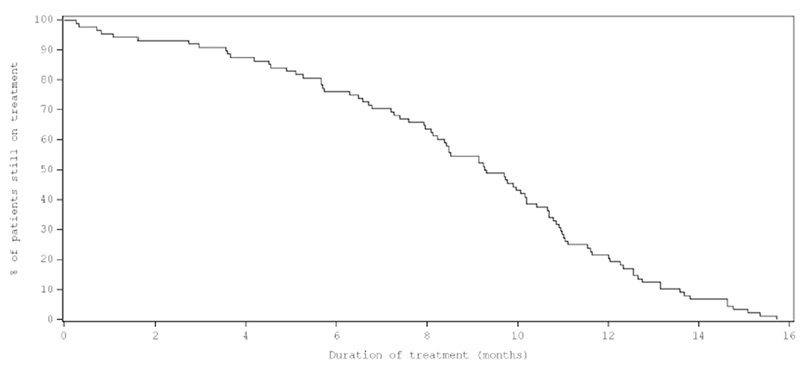
The median duration of total exposure to osimertinib in the sample was 9.3 months (range 0-16).
Figure 2 Exposure plot (percentage of patients still on treatment against time).
Overall response rate (ORR) was assessed for the full Brazilian analysis set (n=88) and also for the subgroup of patients with brain and/or leptomeningeal metastases (n=25). As shown in
| Endpoint | N (%) |
|---|---|
| Total Sample (n=88) |
|
| Overall response rate (n=79) (% [95% CI]) | 58.2 [46.6; 69.2] |
| Best overall response (n=88) |
|
| Responding | 46 (52.3) |
| Stable Disease | 25 (28.4) |
| Progressing | 8 (9.1) |
| Unknown | 9 (10.2) |
| Brain/Leptomeningeal Metastases Present (n=25) |
|
| Overall response rate (n=22) (% [95% CI]) | 59.1 [36.4; 79.3] |
| Best overall response (n=25) |
|
| Responding | 13 (52.0) |
| Stable Disease | 5 (20.0) |
| Progressing | 4 (16.0) |
| Unknown | 3 (12.0) |
Patients with no assessment were recorded as ‘Unknown’.
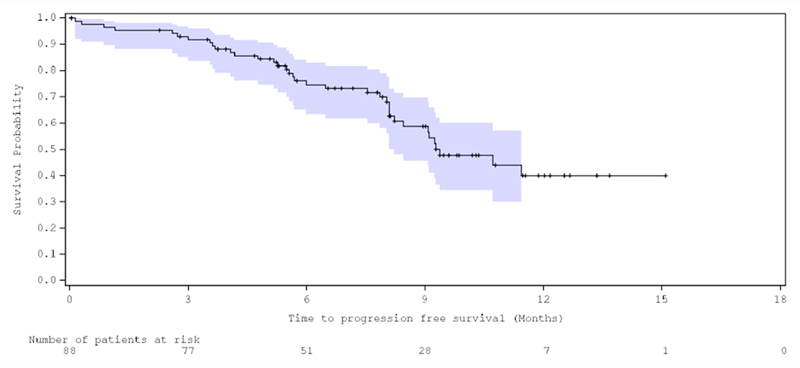
Patients had a median PFS of 9.4 months (95% Confidence Interval [CI] 8.2-not reached] (
Figure 3 Kaplan Meier plot of time to progression free survival.
Osimertinib was generally well tolerated and only 5.7% of patients discontinued treatment due to adverse events (AEs) (
| Endpoint | N (%) |
|---|---|
| Number of patients with at least one: Adverse Event | 30 (34.1) |
| Adverse Event Leading to Dose Modification | 14(15.9) |
| Adverse Event Leading to Discontinuation | 5 (5.7) |
| Adverse Event of Special Interest | 3 (3.4) |
| Serious Adverse Event | 19(21.6) |
| Adverse events in > 2% of patients |
|
| Pneumonia | 5 (5.7) |
| Diarrhea | 3 (3.4) |
| Neutropenia | 2 (2.3) |
| Thrombocytopenia | 2 (2.3) |
| Blepharitis | 2 (2.3) |
| Vomiting | 2 (2.3) |
| Electrocardiogram QT prolonged | 2 (2.3) |
| Deep vein thrombosis | 2 (2.3) |
| Death | 3(3.4) |
The PFS, OR and tolerability profile results confirm the efficacy of osimertinib in patients with advanced T790M-positive NSCLC who progressed after receiving an EGFR-TKI. These findings are particularly relevant considering the real-world approach, indicating that even outside the context of clinical trial patients achieve clinically sound benefits. Estimated median PFS of 9.4 months are in line with those observed in osimertinib AURA clinical trials program[
ORR was also similar to the ones reported in clinical trials, for all patients and particularly for those with CNS metastasis. CNS metastasis are life-threatening complications of NSCLC present in approximately 2040% of patients.[
Osimertinib demonstrated and adequate toxicity profile with 5.7% of discontinuations due to AEs. A total of 21.6% of all patients had dose modifications (interruption or reduction) due to AE, similar to the rates reported by AURA2[
Limitations of our study can be related to the reduced sample size and the single-arm design. Despite these limitations, this is the first Brazilian study assessing efficacy and safety of osimertinib in this particular subgroup of lung cancer patients with acquired resistance to a previous line of EGFR-TKIs. These patients faced unmet needs with the previous available therapeutic options in the Brazilian healthcare system and local data may help guide prescribers and policy decision-makers to better address these needs. Phase IV real-world study also provides a more pragmatic overview of the treatment effects without the controlled environment and cointerventions typical of clinical trials, thus allowing care providers to understand how their patients can respond to therapy in real life.
More recently, osimertinib was tested as front-line therapy for advanced T790M- positive NSCLC in the FLAURA trial[
In a real-world setting, osimertinib constitutes a safe and effective therapeutic option for Brazilian patients with advanced T790M-positive NSCLC after progression on a prior EGFR-TKI, including those patients with central nervous system metastasis. Our findings support previous observations and add valuable information regarding osimertinib effectiveness in Brazilian patients.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.