Severe acute respiratory syndrome coronavirus-2 (SARS-COV-2) is a novel coronavirus identified in December 2019 in Wuhan, China
There is limited data on coronavirus disease-2019 (COVID-19) in patients with solid and hematologic malignancies, and the incidence of SARS-COV-2 in cancer patients with respiratory symptoms is not characterized
We retrospectively reviewed medical records of 24 patients with a diagnosis of solid cancer and hematologic malignancies who presented to the ED with respiratory symptoms at the Centro de Oncologia e Hematologia Einstein Familia Dayan-Daycoval (São Paulo, Brazil) from March 13 to March, 29, 2020. We recorded demographic, clinical and treatment data. All patients underwent COVID-19 diagnostic testing by RT-PCR, and 20 also collected a multiplex panel for 15 respiratory viruses in upper respiratory tract specimens.
The study was approved by the ethics comittee of Hospital Israelita Albert Einstein (Protocol 30978820.0.0000.0071)
Eleven patients (46%) had solid cancer, and the remaining 13 (54%) had hematologic malignancies (
| Patient characteristics - N = 24 | N (%) / mean (range) |
|---|---|
| Age | 61 (33 - 95) |
| Primary diagnosis Solid Tumors | 11 (46%) |
| GI cancers | 3 |
| Breast | 3 |
| Lung | 2 |
| Ovary | 2 |
| Head and neck | 1 |
| Hematologic Malignancies | 13 (54%) |
| Multiple Myeloma | 5 |
| Acute leukemia | 3 |
| CLL | 2 |
| Lymphoma | 3 |
| SARS-COV-2 RT-PCR Positive | 3 (12%) |
| Multiple Myeloma | 1 |
| CLL | 1 |
| Lymphoma | 1 |
| LGL | 1 |
One patient had a diagnosis of Multiple myeloma and LGL
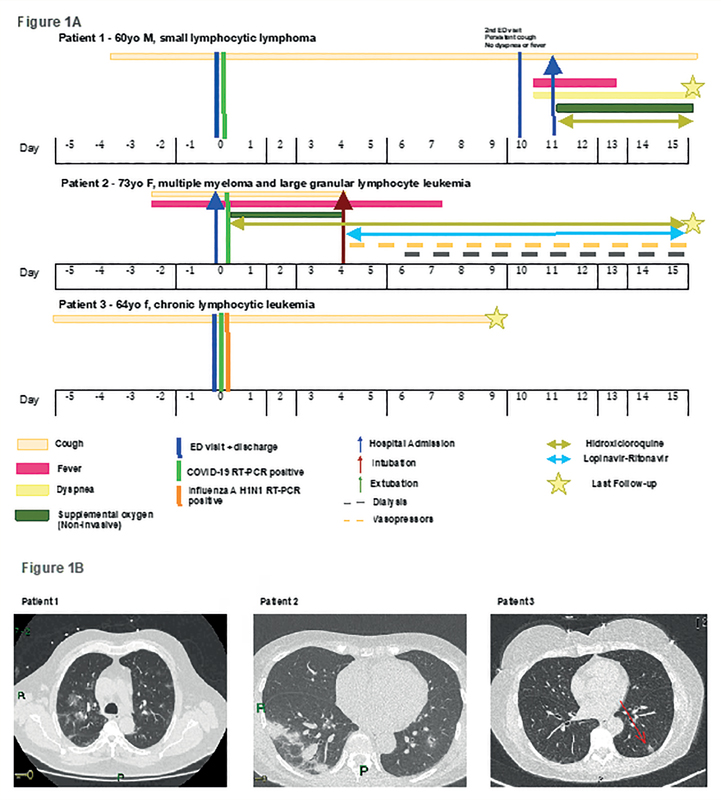
All 3 cases of COVID-19 occured in patients with hematologic malignancies (
Figure 1 Clinical and radiologic characteristics of COVID-19 in 3 patients with hematologic malignancy.
SARS-CoV-2 is an emerging pathogen, and early data suggest higher morbimortality for patients with cancer
Further, we describe the clinical course a case of influenza A H1N1 coinfection with COVID-19 in a patient with hematologic malignancy. Viral coinfection has been described in 5.8% of COVID-19 patients, and could potentially be more common in immunocompromised hosts
Ongoing studies are needed to assess the likelihood of SARS-CoV-2 infection in patients with solid and hematologic malignancies presenting with respiratory symptoms, as this will unequivocally evolve with the dynamic landscape of the pandemic. Moreover, additional data is central to determine patients at risk of readmission, to allow for the development of safe guidelines establishing factors that define need for hospitalization specifically for cancer patients.
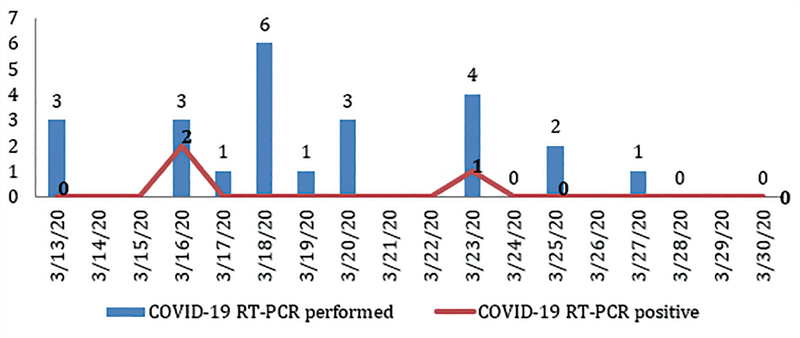
Supplementary Figure 1 Number of COVID-19 RT-PCR tests performed each day.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.