Gastric cancer is recognized as a worldwide common neoplasm and commonly associated with a large number of cancer deaths.
Chondrosarcomas are the second most frequent bone neoplasms and usually disseminates to the lungs.
A 79-years-old female patient sought medical attention due to a complaint of intermittent, burning epigastralgia, which gets worse during feeding for 2 months. The epigastralgia started 2 months before presentation associated with postprandial nausea, progressive asthenia, and anorexia, in addition to two cases of melena in the period, with significant and unintentional weight loss (>10% in two months).
She was previously submitted to an excision of a chondrosarcoma in the thigh 13 years before presentation, and an excision of a moderately differentiated chondrosarcoma of the ribs associated with a left lung lobectomy 6 years before the beginning of epigastralgia. The patient denied any family history of neoplasms.
On physical examination, the patient presented with an axillary temperature of 36,9°C, a heart bitrate of 81 BPM, respiratory rate of 19 BPM and arterial blood pressure of 100×50 mmHg. On examination, she was pale, with pain on deep palpation in the left upper quadrant of the abdomen, with no signs of peritoneal irritation. There were no palpable masses or lymph node enlargement.
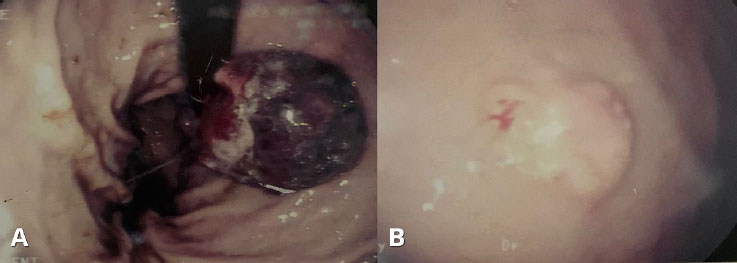
Through the hospitalization for investigation of the condition, she presented severe anemia (hemoglobin at the admission of 4.8g/dl), requiring blood transfusion. Upper gastrointestinal endoscopy (UGE) was requested to investigate upper gastrointestinal bleeding, which revealed a polypoid lesion with a diameter of approximately 5cm in the gastric body, and an ulcerative-infiltrative gastric lesion in the lesser curvature, in the juxtacardial region, approximately 2cm in diameter, with an area of necrosis on the surface. Polypectomy and biopsies were performed to histopathological analysis of the polypoid and ulcerative-infiltrative lesions, respectively, which showed a spindle-cell proliferation consistent with gastrointestinal stromal tumor (GIST), with high malignancy potential, requiring immunohistochemical profile to confirm (
Figure 1 Gastric lesions at the upper gastrointestinal endoscopy. A. Polypoid lesion with a diameter of approximately 5cm in the gastric body; B. Ulcerative-infiltrative gastric lesion in the lesser curvature, with approximately 2cm in diameter and an area of necrosis on the surface.
Contrast-enhanced computed tomography (CT) of the abdomen was performed to stage the lesion, which revealed an expansive solid lesion, with enhancement in the topography of the hepatic hilum, in addition to a heterogeneous solid nodule with contrast uptake located in the tail of the pancreas.
Because of the severe gastrointestinal bleeding associated with the lesion, surgical treatment with abdominal exploration was proposed before the result of immunohistochemical analysis, during which a lesion in the small curvature and a lymph node block in the splenic hilum in contact with the tail of the pancreas were observed. Considering the histological aspect of a GIST with high malignant potential, a D2 total gastrectomy, with a Roux-en-Y reconstruction, in addition to caudal pancreatectomy with splenectomy were performed, without perioperative complications.
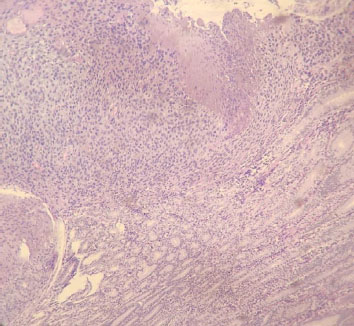
The histopathological evaluation of the surgical specimen revealed an undifferentiated, ulcerated, sarcomatoid gastric neoplasm with osteoclast-like giant cells and formation of embryologically mature and immature tissues (
Figure 2 Histopathological findings. The microscopic aspect of the gastric lesion, showing atypical cell proliferation, with some giant multinucleated cells osteoclasts-like, in addition to osteoid, cartilage and bone formation.
Immunohistochemical analysis of the surgical specimen was also requested, which showed the following immunohistochemical profile: negative for S100, desmin, DOG1, cytokeratin, CD 117, CD 57, CD 34, and smooth muscle actin; and positive for vimentin, which, associated with the patient's personal history, is compatible with a metastatic chondrosarcoma implant (
| ANTIBODY | CLONE | RESULT |
|---|---|---|
| Alpha-smooth muscle actin | 1 to 4 | Negative |
| CD 34 | QBEnd 10 | Negative |
| CD 57 | TB01 | Negative |
| CD 117 | Polyclonal | Negative |
| Cytokeratin | AE1/AE3 | Negative |
| DOG1 | SP31 | Negative |
| Desmin | D33 | Negative |
| S100 | Polyclonal | Negative |
| Vimentin | V9 | Positive |
After the surgery, the patient maintained a follow-up with the oncological surgery team. A year after the gastrectomy, contrast-enhanced chest and abdomen CT scans were requested, which showed a contrast-enhanced pulmonary nodule in the right lower lobe and a solid nodule on the antimesenteric border of the ascending colon. She was referred to the clinical oncology service to evaluate systemic therapy, which was contraindicated.
The patient lost follow-up with the department, returning 5 years after the gastrectomy with a contrast-enhanced chest CT showing grouped and peripheral, hypocaptating lung masses, located in the posterosuperior portion of the left lung, in close contact with the adjacent pleura and descending aorta, in addition to non-calcified, subpleural nodules, compatible with secondary neoplastic implants.
Six years after the gastrectomy, the patient is alive, but with loss of performance status due to the secondary neoplastic implants, in treatment with the clinical oncology department.
Chondrosarcoma is a group of primary bone neoplasms that share the capacity of producing hyaline cartilaginous tissue in its matrix.
In this patient with a prior history of a chondrosarcoma, the immunohistochemical profile was compatible with a secondary metastatic implant of a bone tumor. The remaining 10% of conventional type cases are high grade lesions with a worse prognosis and high rates of metastatic spreading.
The most common pathway of metastasis in chondrosarcomas, as well as in other sarcomas, is the hematogenous route, with the lungs, by far, being the most affected site.
Gastric neoplasms are almost entirely primary tumors, mainly represented by gastric adenocarcinomas.
A few aspects of stomach metastases are described in the literature, in an attempt to distinguish them from primary tumors in the absence of a conclusive histopathological report. Three morphological features on upper digestive endoscopy have been reported: masses without ulceration, submucosal masses with elevation and central ulceration, and multiple masses of varying sizes and punctual ulceration.
The histopathological aspects of chondrosarcoma vary according to the type and degree of differentiation. Atypical chondrocytes with irregular sizes and shapes can be observed, with an amount of cartilaginous matrix, number of mitotic figures, and variable cellularity, mainly in conventional chondrosarcoma.
The severe gastrointestinal bleeding associated with the gastric lesion supported, in the present case, the surgical therapeutic approach. The observation of intraoperative lesions indicated the performance of a gastrectomy with lymphadenectomy, a common treatment for primary gastric neoplasms.
Furthermore, chondrosarcoma represents a set of neoplasms with high resistance to chemotherapy and radiotherapy. Therefore, the surgical approach has a major role in the treatment of chondrosarcomas, especially the primary ones.
In conclusion, a great benefit in the use of a surgical resection of the gastric lesion was observed in the present case, obtaining a resolution of the gastrointestinal bleeding and a survival of more than 5 years. Thus, in addition to the high chemotherapy and radiotherapy resistance of the chondrosarcomas, the present study supports the hypothesis that a surgical treatment may be considered in the presence of chondrosarcoma metastases in selected individuals.
kANG: Collection and assembly of data, Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
PHSN: Collection and assembly of data, Final approval of manuscript, Manuscript writing
DTM: Collection and assembly of data, Final approval of manuscript, Manuscript writing
CST: Collection and assembly of data, Final approval of manuscript, Manuscript writing
ISG: Data analysis and interpretation, Final approval of manuscript, Manuscript writing
MPSSC: Collection and assembly of data, Data analysis and interpretation, Final approval of manuscript
RMLVL: Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing
MLVC: Conception and design, Data analysis and interpretation, Final approval of manuscript, Manuscript writing, Provision of study materials or patient
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Sung, H and Ferlay, J and Siegel, RL and Laversanne, M and Soerjomataram, I and Jemal, A. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin [online]. 2021, vol. 71, p. 209-49.
2. Almubarak, MM and Laé, M and Cacheux, W and Cremoux, P and Pierga, JY and Reyal, F. Gastric metastasis of breast cancer: a single centre retrospective study. Dig Liver Dis [online]. 2011, vol. 43, p. 823-7.
3. El-Sourani, N and Troja, A and Raab, HR and Antolovic, D. Gastric metastasis of malignant melanoma: report of a case and review of available literature. Viszeralmedizin [online]. 2014, vol. 30, p. 273-5.
4. Mery, B and Espenel, S and Guy, JB and Rancoule, C and Vallard, A and Aloy, MT. Biological aspects of chondrosarcoma: leaps and hurdles. Crit Rev Oncol Hematol [online]. 2018, vol. 126, p. 32-6.
5. Konishi, H and Isetani, K and Satoh, T and Fukuda, S and Kodama, T and Kashima, K. A case of metastatic chondrosarcoma of the stomach. J Gastroenterol [online]. 1994, vol. 29, p. 495-500.
6. Chow, W and Frankel, P and Ruel, C and Araujo, DM and Milhem, M and Okuno, S. Results of a prospective phase 2 study of pazopanib in patients with surgically unresectable or metastatic chondrosarcoma. Cancer [online]. 2020, vol. 126, p. 105-11.
7. Chen, YC and Wu, PK and Chen, CM and Tsai, SW and Chen, CF and Chen, WM. Prognostic factors and survival in conventional chondrosarcoma: a single institution review. J Chin-Med Assoc [online]. 2020, vol. 83, p. 669-73.
8. Zając, AE and Kopeć, S and Szostakowski, B and Spałek, MJ and Fiedorowicz, M and Bylina, E. Chondrosarcoma-from molecular pathology to novel therapies. Cancers (Basel) [online]. 2021, vol. 13, p. 2390.
9. Bovée, JVMG and Flanagan, AM and Lazar, AJ and Nielsen, GP and Yoshida, A. Soft tissue and bone tumors. IARC Press, 2020.
10. Dong, Y and Wu, W and Kang, H and Xiong, W and Ye, D and Fang, Z. Risk factors of regional lymph node (RLN) metastasis among patients with bone sarcoma and survival of patients with RLN-positive bone sarcoma. Ann Transl Med [online]. 2021, vol. 9, p. 48.
11. Gupta, R and Sharma, MC and Attri, S and Guleria, S. Testicular metastasis of extraskeletal myxoid chondrosarcoma: report of first case. Urology [online]. 2008, vol. 71, p. 984.e1-e4.
12. Wu, ZH and Dai, JY and Shi, JN and Fang, MY and Cao, J. Thyroid metastasis from chondrosarcoma. Medicine (Baltimore) [online]. 2019, vol. 98, p. e18043.
13. Kim, JM and Wong, AJ and Lu, AJ and Pointdujour-Lim, R. Chondrosarcoma metastasis to the choroid. Ocul Oncol Pathol [online]. 2019, vol. 5, p. 234-7.
14. Johnston, FM and Beckman, M. Updates on management of gastric cancer. Curr Oncol Rep [online]. 2019, vol. 21, p. 67.
15. Weigt, J and Malfertheiner, P. Metastatic disease in the stomach. Gastrointest Tumors [online]. 2015, vol. 2, p. 61-4.
16. Kim, GH and Ahn, JY and Jung, HY and Park, YS and Kim, MJ and Choi, KD. Clinical and endoscopic features of metastatic tumors in the stomach. Gut Liver [online]. 2015, vol. 9, p. 615-22.
Dados de acesso insuficientes para visualização no mapa.