Although lung cancer is the leading cause of death worldwide, advances in immunotherapy and molecular-targeted therapies are improving patient outcomes.[
The central nervous system (CNS) has been a frequent site of metastases from lung cancer.[
Up to now the best treatment approach to manage these patients is not well-defined.[
We aimed to evaluate survival outcomes of patients with CNS metastases from lung adenocarcinoma harboring EGFR-activating mutations, previously untreated with EGFR-TKIs (EGFR-TKI naïve), who were treated with a multidisciplinary approach in a Brazilian public academic cancer center.
We performed a retrospective analysis of all consecutive patients with CNS metastases of lung adenocarcinoma harboring EGFR-activating mutations, treated at Instituto do Câncer do Estado de São Paulo Cancer (ICESP), between 2009 and 2017.
Electronic records of all patients who received an EGFR-TKI were reviewed. We collected data on clinical and demographical characteristics of patients, smoking status, type of EGFR-activating mutation, treatment received and survival outcomes.
The study was approved by local Research Ethic Committees.
Patients were included in case of CNS metastases of histologically confirmed lung adenocarcinoma harboring an EGFR-activating mutation and who had not received any treatment including any chemotherapy or any EGFR-TKI before of the diagnosis of brain metastases (EGFR-TKI naïve). In order to confirm the EGFR status and following the local recommendation, Sanger sequencing was performed in archived or new formalin-fixed paraffinembedded samples. The CNS involvement was diagnosed based on computed tomography scans, magnetic resonance imaging and/or cerebrospinal fluid findings.
Exclusion criteria included the previous use of EGFRTKIs, diagnosis of another malignancy (with the exception of non-melanoma skin cancer, carcinoma in situ of the cervix and carcinoma ductal in situ of the breast) and lack of sufficient data to assess patients' outcomes after treatment.
Multidisciplinary tumor board discussions guided individual patient treatments. All patients received an EGFR-TKI as standard systemic treatment for lung adenocarcinoma harboring EGFR-activating mutations at our Institution. Two EGFR TKIs were available during this study, depending on the time period: erlotinib or gefitinib. Erlotinib or gefitinib were given orally at daily doses of 150mg and 250mg, respectively. Administered dose reductions followed the publicly available recommendations.
Other treatment strategies received by patients could include surgery for resection of brain metastasis, intrathecal chemotherapy, whole brain radiation therapy (WBRT), and/or stereotactic radiosurgery (SRS). SRS was the preferred local treatment for those patients presenting 1-4 lesions, measuring less than 4cm in those patients neurologically sTable. Surgery was indicated in neurologically unsTable patients. WBRT was administered in those patients not candidates for neither SRS nor surgery, and EFGR-TKIs were not administered concurrently with WBRT.
The primary objective of the study was to evaluate the overall survival of patients with CNS metastases of lung adenocarcinoma harboring EGFR-activating mutations. Secondary objectives were to characterize the treatment strategies received, evaluate the progression-free survival and prognostic factors associated with survival.
Overall survival was defined as the time from the initiation of the EGFR-TKI until death from any cause. Progression-free survival was the time from initiation of the EGFR-TKI until clinical or radiological progression, or death from any cause. Patients without these events were censured at time of last follow-up.
Descriptive statistics was used to present patient and treatment characteristics. Qualitative variables were compared between groups using Chi-squared test or Fisher Exact test, whenever appropriate. Quantitative variables were compared with Student t-test.
Survival estimates were performed using the Kaplan-Meier method. The logrank test was used to compare survival curves. Potential factors associated with overall survival were evaluated using univariable and multivariable analyses by Cox proportional hazards model. Evaluated factors were: EGFR-TKI (gefitinib vs erlotinib), EGFR-activating mutations (exon 21 vs exon 19), radiation therapy to the brain (yes vs no), upfront radiation therapy to the brain (yes vs no), ECOG-PS (3-4 vs 0-2), number of brain metastases (2-4 vs 1; >4 vs 1), size of the largest brain metastasis (>1cm vs = 1cm), and diseasespecific graded prognostic assessment (dsGPA) (2-3.5 vs 0-1.5). Briefly, dsGPA is a tool to evaluate prognosis of patients with brain metastases, largely used in the daily clinical practice in order to estimate survival endpoints and better select the most appropriate treatments, based on the number of metastatic brain lesions, besides age, performance status and the presence of extracranial metastastic spread.[
Thirty-five consecutive patients met the eligibility criteria and were included in the present study. Median age was 63 years (range 35-90). Twentysix patients (74%) were female and 9 (26%) were male. Half of patients were non-smokers. ECOGPS was 0-1 in 17 patients (48.5%) and 2 in 9 patients (25.7%). Most patients (65.7%) had dsGPA 2.0-3.5. The majority of the patients had an EGFR exon 19 deletion (N=25; 71.4%) or an EGFR exon 21 L858R mutation (N=9; 25.7%). Only one patient had an EGFR exon 18 G719A mutation. Patients' characteristics are summarized in
| N | % | |
|---|---|---|
| Age at diagnosis Median (range) | 63 (35-90) | |
| Sex Female | 26 | 74.2 |
| Male | 9 | 25.7 |
| Never smoker | 19 54.2 | |
| ECOG-PS 0-1 | 17 | 48.5 |
| 2 | 9 | 25.7 |
| 3-4 | 9 | 25.7 |
| Extracranial metastases Yes | 33 | 94.3 |
| No | 2 | 5.7 |
| Number of brain metastases 1 | 5 | 14.2 |
| 2-4 | 10 | 28.5 |
| > 4 | 15 | 42.8 |
| Leptomeningeal only | 1 | 2.8 |
| Not available | 4 | 11.4 |
| Largest brain metastasis = 1cm | 6 | 17.1 |
| > 1cm | 24 | 68.5 |
| Not available | 4 | 11.4 |
| dsGPA 0-1.5 | 11 | 31.4 |
| 2.0-3.5 | 23 | 65.7 |
| EGFR mutation EGFR exon 19 deletion | 25 | 71,4 |
| EGFR exon 21 L858R mutation | 9 | 25.7 |
| EGFR exon 18 G719A mutation | 1 | 2.8 |
Abbreviations: N = number; ECOG-PS = Eastern Cooperative Oncology Group Performance Status; dsGPA = disease-specific graded prognostic assessment; EGFR = epidermal growth factor receptor.
All patients had received an EGFR TKI. Twenty-three patients (65.7%) received erlotinib and 12 (34.2%), gefitinib. Four patients who had received erlotinib required dose reductions due to toxicities. Median treatment time with EGFR TKI was 7.6 months (interquartile range [IQR], 2.2-11.6 months). The treatment duration of erlotinib and gefitinib did not differ (median treatment time: 7.5 and 8.3 months, respectively; p=0.836).
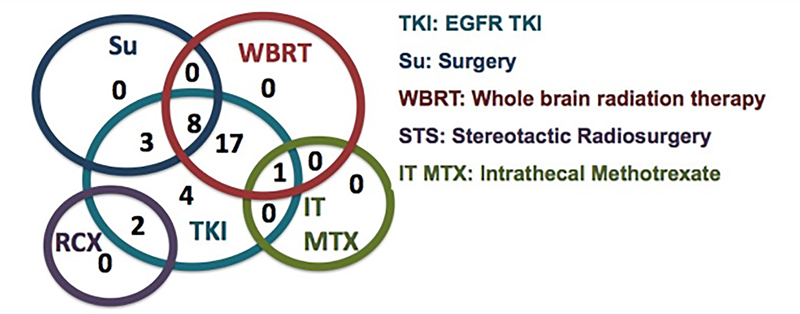
Eleven patients were treated with surgery for brain metastases. Most patients (N=26) received WBRT, while only 2 were treated with SRS and 7 received no radiation therapy. Twenty-four patients received upfront radiation therapy (WBRT or SRS), followed by an EGFR-TKI. Eleven patients received upfront EGFR-TKI, followed by WBRT (N=4) or no radiation therapy (N=7). Only one patient was treated with intrathecal chemotherapy with methotrexate, due to leptomeningeal involvement.
Figure 1 Venn diagram of the treatments received by all 35 patients with central nervous system metastases of lung adenocarcinoma harboring an EGFR-activating mutation.
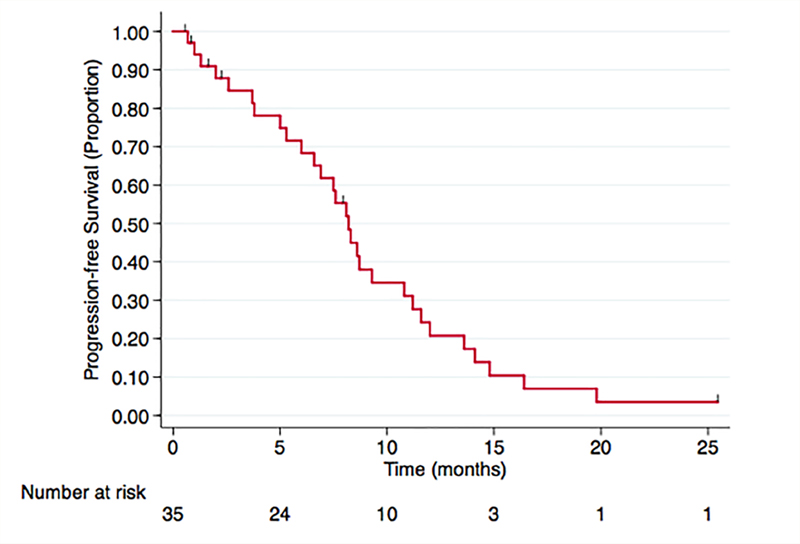
After a median follow-up of 10.6 months, 29 patients presented disease progression or death. Median PFS was 8.2 months. Six-month was 68.3% (95% confidence interval [CI], 49%-81.5%) and 1-year PFS, 20.7% (95% CI, 8.4% - 36.6%). The Kaplan-Meier curve for PFS is presented in
Figure 2 Progression-free survival of patients with central nervous system metastases of lung adenocarcinoma harboring an EGFR-activating mutation after treatment initiation with an EGFR tyrosine kinase inhibitor.
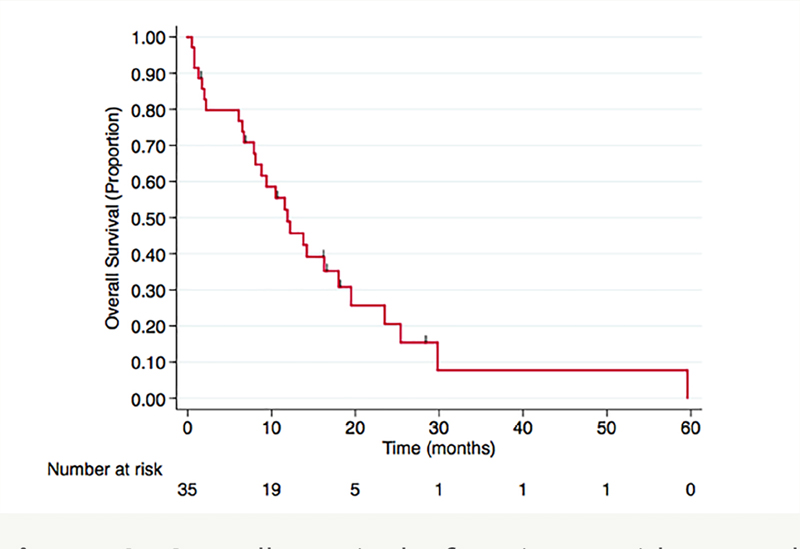
Twenty-seven deaths occurred during the study period. Median OS for all the study population was 11.9 months, and 6-month and 1-year OS were 79.7% (95% CI, 62%-89.7%) and 48.9% (95% CI, 31.1%-64.5%), respectively.
Figure 3 Overall survival of patients with central nervous system metastases of lung adenocarcinoma harboring an EGFR-activating mutation after treatment initiation with an EGFR tyrosine kinase inhibitor.
In the univariable analysis, poor ECOG-PS (ECOG PS 3-4) (HR, 2.74; 95% CI, 1.17-6.38; p=0.019) and unfavorable dsGPA (dsGPA 0-1.5) (HR, 3.15; 95% CI, 1.28-7.71; p=0.012) were associated with inferior OS. Moreover, radiation therapy to brain metastases (WBRT or SRS) had a trend towards improved overall survival (HR, 0.43; 95% CI, 0.16-1.10; p=0.081) in comparison with no radiation therapy. None of the other factors had statistically significant association with OS.
ECOG-PS and administered radiation therapy were included in the multivariable analysis. The dsGPA was not included in the multivariable analysis because it was associated with both ECOG-PS (?2 test, p=0.010) and administered radiation therapy (?2 test, p=0.013). Patients with unfavorable dsGPA received less radiation therapy (45% did not receive radiation therapy vs 8% in the favorable dsGPA).
In the multivariable analysis, poor ECOG-PS remained independently associated with inferior OS (HR, 2.86; 95% CI, 1.12-6.74; p=0.016). The trend towards superior OS (HR, 0.40; 95% CI, 0.15-1.06; p=0.066) of patients treated with radiation therapy was also confirmed. Results of the univariable and multivariable analyses by Cox proportional hazards model are summarized in
|
| Univariable analysis | Multivariable analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p value | HR (95% CI) | p value | ||
| EGFR mutation Exon 21 vs Exon 19 | 1.00 (0.50 - 2.00) | 0.991 |
|
| |
| EGFR TKI Gefitinib vs Erlotinib | 1.06 (0.45 - 2.51) | 0.878 |
|
| |
| RT Yes vs No | 0.43 (0.16 - 1.10) | 0.081 | 0.40 (0.15 - 1.06) | 0.066 | |
| Upfront RT Yes vs No | 0.78 (0.34 - 1.78) | 0.561 |
|
| |
| ECOG-PS 3-4 vs 0-2 | 2.74 (1.17 - 6.38) | 0.019 | 2.86 (1.21 - 6.74) | 0.016 | |
| No. of brain metastases 2-4 vs 1 | 0.78 (0.22 - 2.77) | 0.711 |
|
| |
| > 4 vs 1 | 0.60 (0.19 - 1.88) | 0.388 |
|
| |
| Largest brain metastasis > 1cm vs = 1cm | 0.83 (0.30 - 2.30) | 0.729 |
|
| |
| dsGPA 0-1.5 vs 2-3.5 | 3.15 (1.28 - 7.71) | 0.012 |
|
| |
Abbreviations: OS = overall survival; HR = hazard ratio; CI = confidence interval; EGFR = epidermal growth factor receptor; TKI = tyrosine kinase inhibitor; RT = radiation therapy; No. = number; ECOG-PS = Eastern Cooperative Oncology Group Performance Status; 1Cox proportional hazards model
CNS metastases from lung cancer are associated with shorter survival, with median OS ranging from 3 to 15 months.[
Our results showed that EGFR-TKI naïve patients with CNS metastases from lung adenocarcinoma achieve favorable outcomes in comparison with previous literature from patients without driver mutations, when treated with a multidisciplinary approach consisting of an EGFR-TKI, combined or not with radiation therapy (WBRT or SRS) and/or surgery.
However, the median OS of 11.9 months observed in the present study is shorter than that observed in previous studies with similar patients.[
Another important finding of our study was the trend towards improved OS of patients who received radiation therapy in the multivariable analysis (HR, 0.40; 95% CI, 0.15-1.06; p=0.066). However, no difference was seen between upfront radiation therapy followed by EGFR-TKI and upfront EGFR-TKI followed by salvage radiation therapy. The study by Magnuson et al. (2017) also suggested an important role of radiation therapy, favoring upfront radiation therapy.[
Despite the low CNS penetration of first (erlotinib and gefinitib) and second- generation (afatinib), previous prospective and retrospective studies have shown CNS response rates ranging from 35% to 80%.[
Although WBRT was the most common modality of radiation therapy in the present study, some studies suggest that SRS is an appropriate alternative for patients with up to 10 brain metastases.[
The main limitations of our study are its retrospective nature and the small sample size. Even though it has been analyzed a period between 2009 and 2017, only a small number (35 patients) met the eligibility criteria, possibly leading to selection and treatment biases. Patients with poor ECOG performance status and/or unfavorable dsGPA may have received less aggressive treatments, another source of biases. As strengths, our results represent real-life data from a developing country population. We highlight that most of previous data on lung adenocarcinoma patients harboring EGFR- activating mutations come from developed countries where other treatment lines are also available. Despite the benefit of multidisciplinary approaches for CNS metastases, in comparison with the results from previous literature, we can conclude that additional strategies are necessary to improve survival in our population. This could include efforts for earlier diagnosis and treatment access as well as availability of subsequent treatment lines.
In conclusion, patients with CNS metastases of lung adenocarcinoma harboring EGFR-activating mutations may derive promising progression-free survival and overall survival, when treated with a multidisciplinary approach that includes an EGFRTKI. This treatment approach, however, should be individualized, considering patient characteristics, tumor biology aspects and healthcare resources available.
IASLC 18th World Conference on Lung Cancer (WCLC), Yokohama, Japan.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.