Malignant melanoma is a type of skin cancer associated with high mortality rates and low response to chemotherapy or radiotherapy. Immunotherapy with checkpoint inhibitors has provided substantial survival gains along with lower toxic effects and better quality of life for patients with advanced disease.[
Immunotherapy targeting immune checkpoints has changed the landscape of cancer treatment. Immune checkpoints, such as PD1, are inhibitory receptors expressed by T lymphocytes (T cells).[
By blocking these targets, unlike chemotherapy, that aims to directly destroy tumor cells, checkpoint inhibitors act indirectly by enhancing antitumor T cell response.[
Despite improving treatment response and survival rates for several types of cancer, nivolumab is associated with a collection of immune reactions known as immune-related adverse events (irAE), such as thyroid dysfunction, hepatitis, pneumonitis, hypophysitis and colitis.[
BP is a cutaneous autoimmune disorder that involves the expression of two autoantibodies against basement membrane zone (BMZ) autoantigens: BP180 (BPAG2) and BP230 (BPAG1). Both antigens are components of the hemidesmosome, which acts on adhesion between the dermis and the epidermis. The disease is characterized by immunoglobulins (IgG) and complement component C3 deposition in BMZ, and manifests with pruritus, urticariform eruptions, vesicles, subepidermal blisters and, in rare cases, erosive mucosal lesions.[
Drug-induced BP most often appears in the first 6 to 8 months of treatment, with or without prodromes of nonspecific pruritus.[
Diagnosis of BP relies on a combination of clinical criteria, immunopathologic examinations and serology.[
Indirect immunofluorescence study detects IgG circulating autoantibodies that bind to the epidermal side of the skin basement membrane, on salt-split human skin substrate. It is also possible to detect specific circulating anti-basement membrane antibodies (a-BP180/BP230 and a-NC16A) in serum samples by enzyme-linked immunosorbent assay (ELISA).[
In this report, we describe a case of PD-1 inhibitorinduced BP in a patient who received nivolumab as a third line treatment for metastatic melanoma. At first, a small blister appeared after 40 cycles of nivolumab, and evolved as several bullous lesions on his arms, back and abdomen. Immunopathologic examinations revealed the diagnosis of BP. Immunotherapy was suspended and full remission of the lesions was attained by treatment with prednisolone. However, after reintroduction of nivolumab, lesions returned with a diffuse pemphigoid-like pattern in multiple skin sites with local pain, indicating that BP emerged as an adverse event of immunotherapy.
A 62-year-old male patient was submitted to preoperatory tests for the resection of multiple nevus in his left auricular pavilion, in July of 2015, in which pulmonary nodules of secondary aspect were observed by chest X-ray. Afterwards, a biopsy guided by chest tomography of one pulmonary nodule was performed, with anatomopathological examination describing neoplastic cells with epithelioid morphology. Immunohistochemical analysis confirmed a malignant melanoma. PETCT indicated stage IV disease, with secondary involvement of lungs, pleura and left axillary lymph nodes. Genotyping of the BRAF gene showed presence of V600E mutation in exon 15.
The patient reported a previous diagnosis of malignant melanoma in 2007 on the left shoulder, with a Clark level II and with Breslow's thickness of 0.4mm. He was submitted to resection (pathology report does not describe margins of the lesion) and the follow up was performed by a dermatologist. At the time, he was not referred for evaluation with an oncologist. As comorbidities, he reported diabetes mellitus and gout both diagnosed in 2000, and systemic hypertension diagnosed in 1995, in use of diuretics anti-diabetic drugs.
First-line chemotherapy started in August 2015, with dacarbazine 1000mg/m2 on D1, every 03 weeks. Patient was treated for seven months, with partial response as best response, by RECIST.
In June 2016, the subject presented with hepatic, pulmonary and lymph node progression of metastasis, and was treated with vemurafenib 960mg daily as second line therapy. In the first evaluation of response to vemurafenib, in September 2016, PETCT showed exclusive progression of lymph node metastasis in the left axilla, associated with pain that limited mobility of the ipsilateral arm. Palliative radiotherapy was prescribed for better control of local pain, and the patient underwent conformational radiotherapy in the axilla, with a total dose of 3000cGy (300cGy for ten days), between September 21 and 30th, 2016. Shortly after radiotherapy, he started third-line treatment with nivolumab 3mg/kg, D1 every two weeks. The best response obtained was partial response (approximately 90% reduction of the lesions).
Around the 40th cycle of nivolumab, in March 2018, the patient presented with a blister, smaller than 1cm at its largest diameter, in the upper region of his right arm. In a follow-up visit two weeks later, the blister had evolved to an ulcerated healing lesion. One month later, it had changed to a flat, crusty lesion of 1.5cm with a small satellite bullous lesion aside it, along with another small bullous lesion in the anterior region of the same arm, and a grade 1 rash on his face.
In May 2018, several bullous lesions appeared on his arms, back and abdomen, affecting less than 10% of his skin, none with signs of secondary infections and some with a crusty appearance, with pruritus and mild local discomfort. The bullae were tense, and there were no urticarial lesions or mucosal lesions associated. Pruritus was not a prominent symptom. Immunotherapy was suspended on suspicion of the bullous lesions being caused by nivolumab treatment.
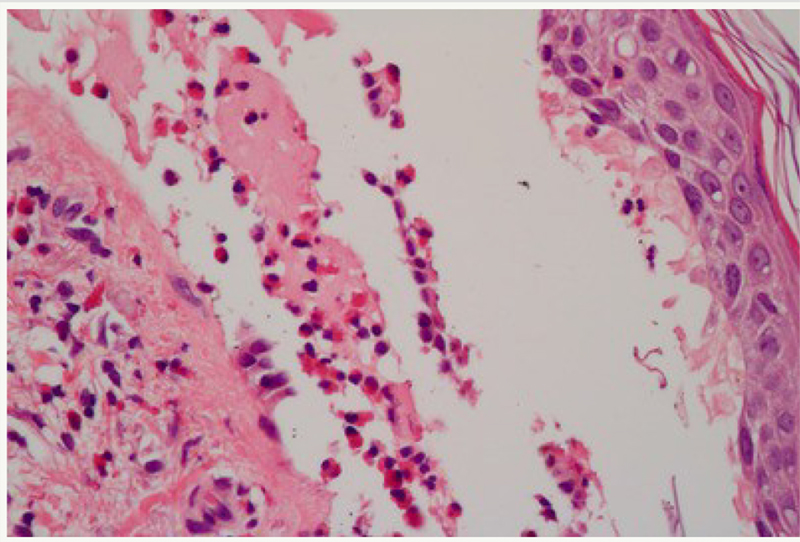
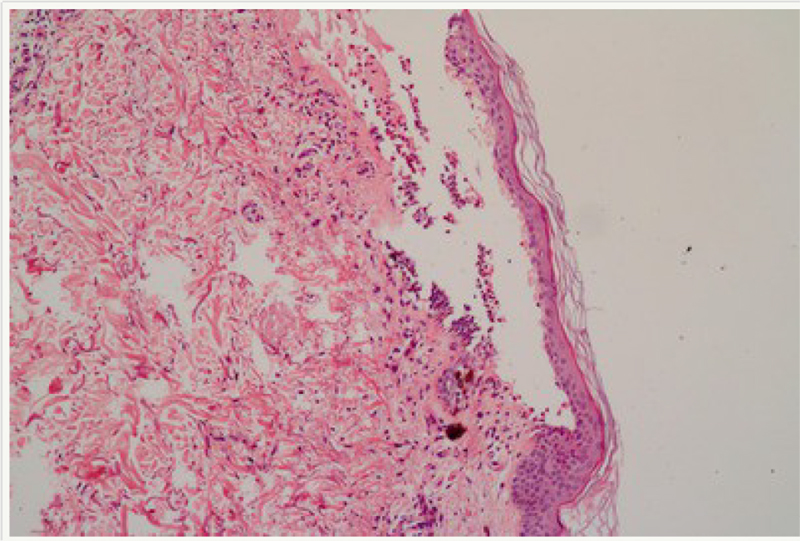
The patient was referred for evaluation by a dermatologist, who biopsied one of the lesions. The histopathological examination on May 2018 reported bullous dermatosis with subepidermal cleavage and perivascular mononuclear infiltrate with eosinophils (
Figure 1 Subepidermal cleft with inflammatory infiltrate containing numerous eosinophils.
Figure 2 Subepidermal cleft with inflammatory infiltrate containing numerous eosinophils.
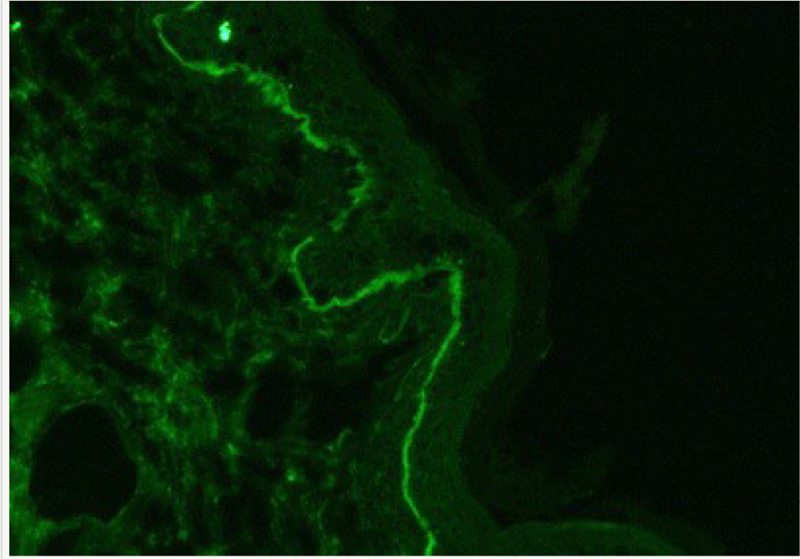
Figure 3 C3, linear in appearance, along the epithelium basement membrane.
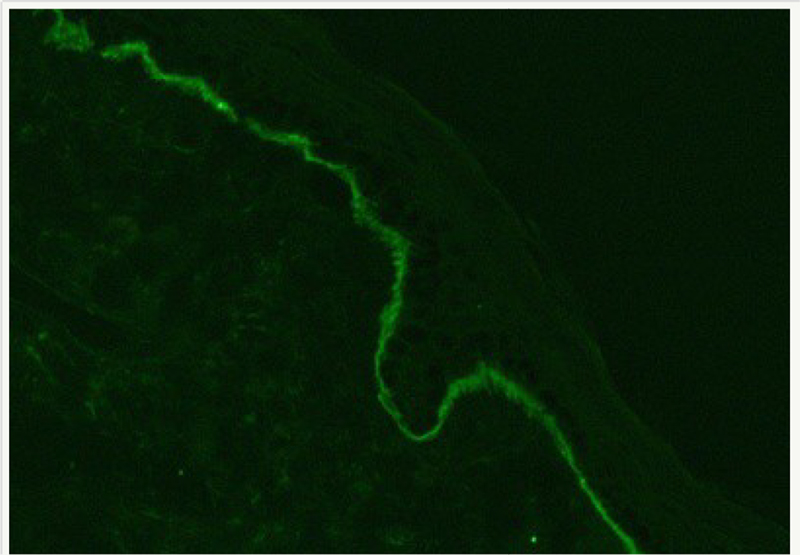
Figure 4 IgG, linear in appearance, along the epithelium basement membrane.
Subsequently, weaning of the corticoid was performed and nivolumab 3mg/kg, D1, every two weeks was resumed.
In the third cycle after reintroduction of nivolumab (August 2018), the patient presented again with a painless bullous lesion, on the back of his left hand. In October 2018, he complained of microblisters spread on his back and upper left limb (grade 3), in addition to grade 1 fatigue. Once again, nivolumab was stopped due to diffuse pemphigoidlike lesions in multiple skin sites with local pain, and prednisolone 80mg/day was prescribed for 10 days. The weaning of the corticoid was initiated, but dose reduction to less than 10mg/day was associated with the onset of new painful bullous lesions, and the patient was maintained on prednisolone 10mg/ day for approximately three months, when it was possible to progress to complete weaning.
After complete weaning of the corticoid, the patient was in clinical follow-up, without systemic treatment, with PET-CT of February 2019 showing stable disease. On April 03, 2019, patient presented with dysarthria and dizziness, and a single metastasis of 1.3cm was diagnosed in precentral gyrus topography (skull MRI). He underwent radiosurgery on April 09, 2019, with a total dose of 2,100cGy. PET-CT of April 15, 2019, showed that, in addition to central nervous system involvement, he also presented metastatic disease progression to the lungs and bone (only one lesion). Then, on February 05, 2019, fourth-line treatment was initiated, with an oral combination of trametinib 2mg daily, plus dabrafenib 150mg BID, daily.
In the last few years, checkpoint inhibitors have replaced conventional chemotherapy as metastatic melanoma therapy, bringing numerous benefits in survival and quality of life. However, despite the approval of nivolumab as first-line therapy for the treatment of certain tumors, side effects associated with its administration, such as pneumonitis, thyroid dysfunction and hepatitis have often been described.[
Few cases of association between nivolumab monoclonal antibody and bullous pemphigoid have been reported on the literature.[
The main differential diagnosis of bullous pemphigoid evidenced in the clinic are cicatricial pemphigoid, dermatitis herpetiformis, drug-induced bullous disorders, epidermolysis bullosa, epidermolysis bullosa acquisita, erythema multiforme and linear IgA dermatosis.[
In the anatomopathological examination of patient's biopsy, bullous dermatosis with eosinophils was observed in the infiltrate, confirmed with standard immunofluorescence compatible with bullous pemphigoid. Due to low volume, indirect immunofluorescence and salt split skin testing is not fully validated in our supporting Pathology Lab, and since the diagnosis of BP was confirmed by standard immunofluorescence, no further investigation was necessary.[
In this case report, signs of dermatological toxicity started to show after 40 cycles (9 months) of nivolumab, slightly later than expected for druginduced BP (typically 6 months) according to the available literature.[
Considering that the skin lesions started to show in parallel with introduction of nivolumab treatment, and that patient had been in use of all other medications for a long period previously to the rising of BP, we find it unlikely that the disease could be related to diuretic and anti-diabetic drugs. In addition, after full recovery from the first BP manifestations, there was recurrence of the bullous lesions when nivolumab treatment resumed, which strongly suggests that this clinical condition emerged as a cutaneous immune-related adverse event induced by nivolumab and not as a rare paraneoplastic manifestation of melanoma.[
BP has a chronic course and is characterized by periods of exacerbation and remission, but in the absence of adequate treatment, it is progressive and strongly associated with a high morbidity and mortality.[
Finally, it is also extremely important to follow the protocol concerning time to suspend, time to stop and time to resume (when appropriate) treatment with nivolumab in the presence of skin rash. With manifestations of skin rash degrees 1 and 2, it is possible to continue the treatment and to treat symptoms associated. Treatment should be suspended with the presence of a degree 3 cutaneous rash, and only resumed after grade 1 cutaneous lesions is achieved. In the occurrence of a grade 4 rash, nivolumab should not be resumed.
Bullous adverse events such as BP are associated with immunotherapy in 1% of patients and can lead to high morbidity and mortality. When generalized disease occurs, it may require systemic immunosuppressant drugs and often causes disruption of cancer treatment. Early detection of dermatological toxicity and autoimmune adverse events can reduce the need for systemic corticosteroids and the impact on cancer therapy, and immunological diagnostic studies are warranted in patients treated with checkpoint inhibitors who develop initial clinical
The adopted procedures were in accordance with the ethical standards and approved by the Research Ethics Committee of the Santo Antônio symptoms, such as pruritus.
Hospital (Salvador, Bahia, Brazil), with a CAAE 03588818.9.0000.0047. There were no Conflicts of Interest. The patient signed the informed consent approved by the Research Ethics Committee.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.