Quality of life encompasses several categories within the individual and social spheres. It is based on the understanding of fundamental human needs, both material and spiritual, and has its most relevant focus on the concept of health promotion.
Breast cancer impair many women's quality of life. In 2020, it became the most common neoplasm in women, accounting for more than 2.26 million cases and more than 685 thousand deaths worldwide.
Female cancer survivors face physical, psychological, and social hardship. After diagnosis, women worldwide share concerns about the treatment and healing process, body image, interpersonal relationships, and fear of the unknown.
In this sense, spirituality has shown to be a protective factor against mental disorders and for better quality of life, being a common emotional support for cancer patients.
Religiosity and spirituality are different but complementary. Brazil is the second most religious country in the world, with approximately 94% of the population declaring themselves religious.
A cross-sectional study, conducted at a Cancer Center, from February 2021 to August 2022. This study was approved by the ethics and research committee under number 3077/20. All patients with breast cancer treated at the institution who signed the informed consent form were included in the project. After signing the informed consent form, these women received the research link generated on the Research Electronic Data Capture (REDCap, Vanderbilt University) system for completion of two questionnaires: the Spiritual/Religious Coping (SRCOPE)
The SRCOPE scale is a questionnaire covering 92 questions that describes how people use their faith to cope with stress, relating it to quality of life and physical and mental health, as shown in
The WHOQOL - SRPB questionnaire is part of the WHO instrument for assessing quality of life and includes Spirituality, Religion, and Personal Beliefs addressed in 31 questions, as shown in
Patients' age, education, religion, chosen treatment, and tumor's characteristics, such as histological type, were also collected. All the surgeries in which the breast was removed (with or without sparing the nipple), were classified as radical, regardless of the procedure performed in the axilla. All data obtained were entered into the institutional REDCap system. Quantitative variables were expressed in summary measures of position and dispersion, such as mean and standard deviation (SD), or minimum and maximum values. Qualitative variables were expressed in absolute and relative frequencies (%).
For the hypothesis, the Mann-Whitney U and Kruskal-Wallis tests were performed. Spearman's Ro test was performed to assess the correlation between age and the scores of the questionnaires. Statistically significant values were considered for p-values < 0.05.
There were 49 female patients included in the study. Their mean age was 54 years (32–74, 54 ± 10). Of that total, 32 patients (65.3%) were married, 1 (2%) lived in civil partnership, and 5 (10.2%) were separated or divorced. About schooling, 45 participants answered: 73.6% had completed university, 6.1% had not completed university, 6.1% had completed high school, 2% had not completed high school, and 4% had completed elementary school. Regarding religion, 51% identified as catholic, 24.5% were spiritist, 8.2% evangelical, and 16.3% followed other religions (
| Characteristics | n | % |
|---|---|---|
| Marital status Single Married Civil partnership Divorced | 49 11 32 1 5 | 100% 22.4% 65.3% 2% 10.2% |
| Schooling Incomplete elementary school Complete elementary school Incomplete high school Complete high school Incomplete university Complete university Did not respond |
0 2 1 3 3 36 4 |
0% 4% 2% 6.1% 6.1% 73.6% 8.2% |
| Religion Catholic Evangelical Spiritist Others |
25 4 12 8 |
51% 8.2% 24.5% 16.3% |
| Histological tumor type Ductal carcinoma in situ Ductal invasive carcinoma / NST Lobular invasive carcinoma Others |
2 37 2 8 |
4.1% 75.5% 4.1% 16.3% |
| Treatment received* CT neoadjuvant CT adjuvant Conservative surgery Radical surgery Sentinel node biopsy Axillary lymphadenectomy Intraoperative RT (intrabeam) External RT Hormone therapy Immediate reconstructive surgery Delayed reconstructive surgery |
12 20 26 25 31 15 5 28 39 7 9 |
24.5% 40.8% 53.1% 51% 63.3% 30.6% 10.2% 57.1% 79.5% 14.3% 18.4% |
Abbreviations: CT, chemotherapy; NST, nonspecial subtype; RT, radiotherapy.
Note: * Patients underwent more than one treatment; therefore, percentages were calculated based on the total (n = 49).
Invasive ductal carcinoma or nonspecial type was the most prevalent among the patients, corresponding to 75.5% (n = 37) of the cases. Among the treatments given, there was no significant difference between the number of patients who underwent conservative (n = 26) or radical breast (n = 25) surgery, nor regarding immediate (n = 7) or delayed (n = 9) reconstruction. However, more patients underwent sentinel lymph node testing (n = 31), adjuvant chemotherapy (n = 20), external radiation therapy (n = 28), and hormone therapy (n = 39). Many patients underwent a combination of these treatments, so the relative frequency calculated in
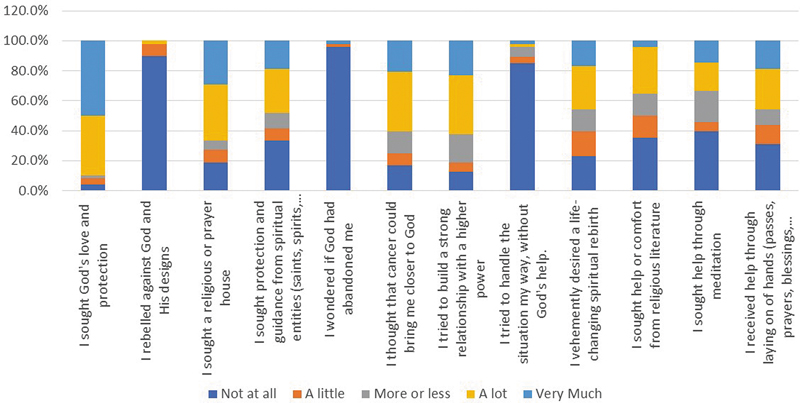
The SRCOPE was answered by 48 patients, with a higher adherence for completion than the WHOQOL-SRPB questionnaire (n = 37). Both assessment instruments contained questions that sought to understand the importance of factors such as optimism, hope, faith, well-being, motivation, forgiveness, and connection to God or to a higher spiritual Being during the patients' treatment. According to the SRCOPE scale's answers, only 2% of the patients felt anger against God and His designs, 48% sought protection and guidance from spiritual entities (saints, spirits, amulets, among others). God's love and protection was sought by 50 and 39.6% of the patients, respectively. There was a search for support in a religious or prayer house by 66.7% of the patients. These data are shown in
Fig. 1 Description of patients' responses to questions 12, 8, 4, 2, 74, 76, 38, 36, 70, 72, 58, and 20 of the SRCOPE scale, expressed in percentages.
Regarding their feelings about God, 2.1% of the patients felt abandoned by God, 4.2% tried to deal with the situation without God's help, while 60.4% of the patients thought that the disease could bring them closer to God, and 62.5% tried to build a stronger relationship with a superior Being (
Other results from the SRCOPE scale not shown in
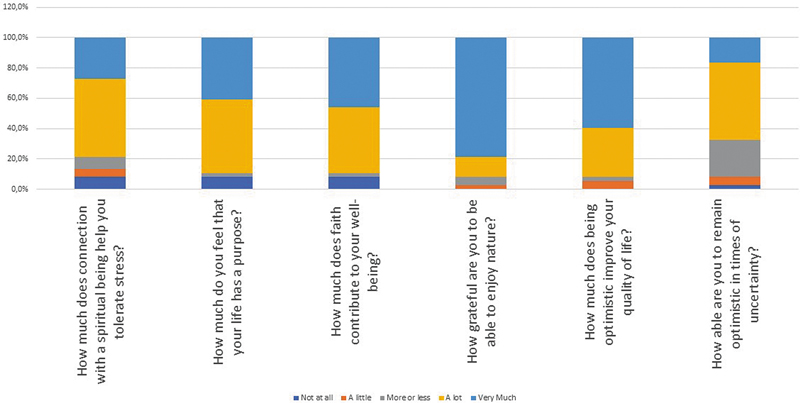
Only 37 patients answered the WHOQOL–SRPB questionnaire. For 91.9% of the respondents, there was a contribution of faith to their well-being, and connection with a spiritual being helps them tolerate stress, by feeling that their life has a purpose (
Fig. 2 Description of patients' responses to questions 29, 7, 2, 28, 27, and 12 of the WHOQOL – SRPB questionnaire, expressed in percentages.
When the hypothesis tests were applied, no correlation was observed between the scores obtained in the SRCOPE and WHOQOL-SRBP and marital status, schooling, religion, and treatment type, except for intraoperative radiotherapy, which showed a positive correlation with the SRCOPE score (p = 0.018), as shown in
| Marital status | Schooling | Religion | Tumor histology | CT adjuvant | CT neoadjuvant | Conservative surgery | Radical surgery | SNB | ALD | Intraop RT | External RT | HT | Immediate reconstructive surgery | Delayed reconstructive surgery | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SRCOPE scale | 0.368 | 0.647 | 0.164 | 0.832 | 0.616 | 0.291 | 0.569 | 0.942 | 0.706 | 0.230 | 0.018* | 0.959 | 0.662 | 0.131 | 0.284 |
| Search for meaning (F1) | 0.823 | 0.647 | 0.015* | 0.460 | 0.356 | 0.902 | 0.127 | 0.326 | 0.482 | 0.403 | 0.275 | 0.715 | 0.717 | 0.005* | 0.272 |
| Strategies of control (F2) | 0.533 | 0.775 | 0.510 | 0.222 | 0.249 | 0.703 | 0.860 | 0.942 | 0.177 | 0.518 | 0.290 | 0.411 | 0.242 | 0.091 | 1 |
| Seek support in God (F3) | 0.956 | 0.586 | 0.401 | 0.401 | 0.714 | 0.326 | 0.664 | 0.984 | 0.923 | 0.815 | 0.092 | 0.747 | 0.523 | 0.203 | 0.567 |
| Seek spiritual support (F4) | 0.902 | 0.204 | 0.441 | 0.774 | 0.564 | 0.476 | 0.534 | 0.967 | 0.804 | 0.316 | 0.016* | 0.942 | 0.540 | 0.031* | 0.835 |
| Transformation of yourself and/or your life (F5) | 0.322 | 0.689 | 0.404 | 0.871 | 0.217 | 0.098 | 0.431 | 0.757 | 0.754 | 0.322 | 0.085 | 0.596 | 0.755 | 0.287 | 0.272 |
| Religions' actions toward spirituality (F6) | 0.511 | 0.422 | 0.006* | 0.401 | 0.368 | 0.694 | 0.357 | 0.695 | 0.167 | 0.024* | 0.207 | 0.795 | 1 | 0.492 | 0.250 |
| Seek spiritual growth/knowledge (F7) | 0.456 | 0.174 | 0.364 | 0.72 | 0.698 | 0.088 | 0.885 | 0.613 | 0.914 | 0.578 | 0.025* | 0.835 | 0.475 | 0.668 | 0.190 |
| WHOQOL-SRPB | 0.715 | 0.967 | 0.365 | 0.731 | 0.135 | 0.350 | 0.395 | 0.841 | 0.906 | 0.848 | 0.140 | 0.819 | 0.259 | 0.880 | 0.319 |
| Connection to a high being or spiritual force (T1) | 0.392 | 0.379 | 0.124 | 0.373 | 0.276 | 0.662 | 0.312 | 0.722 | 0.699 | 0.176 | 0.106 | 0.915 | 1 | 0.747 | 0.407 |
| Meaning of life (T2) | 0.876 | 0.803 | 0.923 | 0.651 | 0.843 | 0.805 | 0.643 | 0.914 | 0.389 | 0.270 | 0.153 | 0.400 | 0.259 | 0.620 | 0.202 |
| Admiration (T3) | 0.638 | 0.967 | 0.968 | 0.651 | 0.819 | 0.227 | 0.761 | 0.654 | 0.960 | 0.614 | 0.248 | 0.725 | 0.894 | 0.503 | 0.245 |
| Wholeness and integration (T4) | 0.876 | 0.222 | 0.100 | 0.651 | 0.350 | 0.531 | 0.737 | 0.722 | 0.578 | 0.392 | 0.071 | 0.531 | 0.747 | 0.813 | 0.542 |
| Spiritual strength (T5) | 0.689 | 0.379 | 0.340 | 0.599 | 0.237 | 0.458 | 0.620 | 0.889 | 0.302 | 0.226 | 0.036* | 0.772 | 0.582 | 0.747 | 0.855 |
| Inner peace (T6) | 0.200 | 0.647 | 0.656 | 0.317 | 0.61 | 0.213 | 0.227 | 0.654 | 0.933 | 0.664 | 0.914 | 0.551 | 0.065 | 0.560 | 0.202 |
| Hope and optimism (T7) | 0.116 | 0.478 | 0.951 | 0.574 | 0.02* | 0.506 | 0.267 | 0.411 | 0.853 | 0.741 | 0.914 | 0.472 | 0.160 | 0.714 | 0.061 |
| Faith (T8) | 0.433 | 0.257 | 0.631 | 0.110 | 0.098 | 0.293 | 0.378 | 0.298 | 0.775 | 0.986 | 0.846 | 0.112 | 0.719 | 0.880 | 0.347 |
Abbreviations: ALD, axillary lymphadenectomy; CT, chemotherapy; HT, hormone therapy (Mann-Whitney test); RT, radiotherapy. Intraop, intraoperative; SNB, sentinel node biopsy; SRCOPE scale, Spiritual/Religious Coping scale; WHOQOL – SRPB, World Health Organization's quality of life instrument - spirituality, religion and personal beliefs module.
Note: * Significance level p-value ≤ 0.05.
When the questionnaires' domains were assessed separately, a positive correlation between intraoperative radiotherapy and the domains of seeking spiritual support (p = 0.016), personal spiritual growth/knowledge (p = 0.025), and spiritual strength (p = 0.036) could be observed. Also, that there was a positive correlation between axillary lymphadenectomy and religious actions toward spirituality (p = 0.024) was found, as well as between adjuvant chemotherapy and hope and optimism (p = 0.02). A positive relationship between immediate reconstructive surgery and seeking meaning (p = 0.005) and seeking support (p = 0.032) was also observed. Although there is no statistical difference, there is a tendency to positively relate hormone therapy with inner peace (p = 0.065), and late reconstructive surgery with hope and optimism (p = 0.061), as shown in
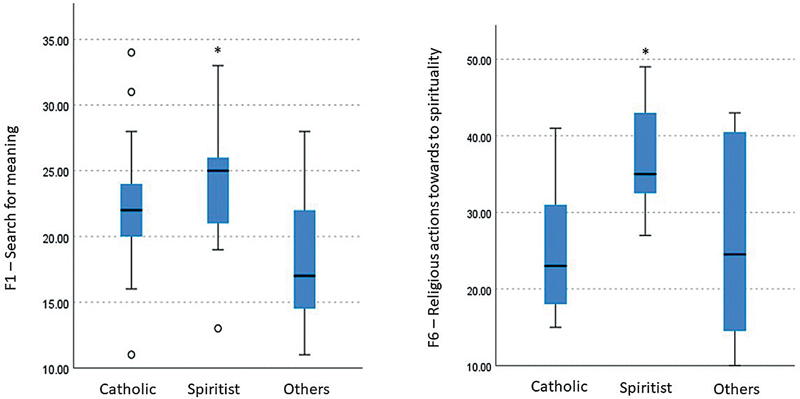
When we assessed the type of religion of the patients, although there was no correlation with the scores of the questionnaires, a positive relationship was observed with search for meaning (p = 0.015) and religious actions toward spirituality (p = 0.006), as shown in
Fig. 3 Relationship between religion and domains F1 (search for meaning) and F6 (religious actions toward spirituality) of the SRCOPE scale. Kruskal-Wallis test. Spiritist F1 (p = 0.007) and F6 (p = 0.001) charts.
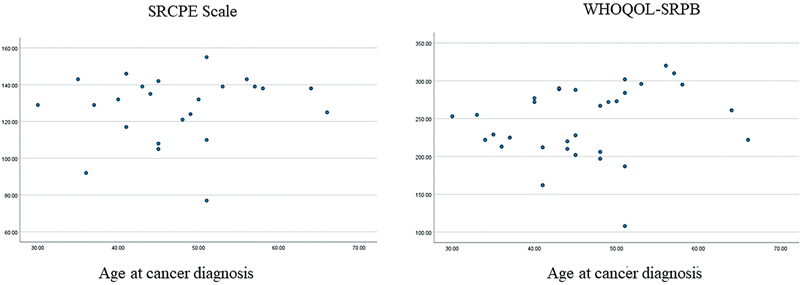
Fig. 4 Correlation between age at cancer diagnosis and SRCOPE and WHOQOL-SRPB scores. Spearman correlation (SRCOPE: 0.276; WHOQOL-SRPB: 0.117).
Studies have shown an association between spirituality and quality of life.
According to Ferreira et al. spirituality is related to the feeling of transcendence, while religiosity involves a natural tendency toward religious feelings and sacred things. Both are coping tools that help patients deal with cancer, positively influencing their quality of life. Furthermore, both religiosity and spirituality can appear after disease diagnosis, when patients feel a lack of meaning to life, or they can be present since before the diagnosis and be a source of strength and hope during treatment.
Data from this study showed that most of the patients sought love and protection from God and/or from spiritual entities at some time during their treatment. Additionally, more than 60% of the patients in this study tried to reach a strong relationship with God or another higher entity, 89% of them believe that faith contributes to well-being, and 78.4% believe that connecting with a spiritual being helps them tolerate stress. These data are close to the results showed by other studies, which relate a positive image of God with hope and optimism,
In addition, most of the patients in this study used spirituality and religiosity as tools to help them coping throughout their treatment and follow-up. It was observed that most of them felt optimistic, which promoted improvement in their quality of life. This fact was corroborated by Purnell et al., who demonstrated a positive correlation between the feeling of peace and meaning with quality of life.
Although less significant, in this study, 2.1% of the patients felt abandoned and rebelled against God. The feeling that they were being punished for their mistakes and need to ask God for forgiveness also reveals that the diagnosis and the confrontation with this disease lead to negative feelings and bring into play questions that are often linked to historical, cultural, and personal beliefs. According to Paredes and Pereira, a traumatic event, such as the diagnosis of breast cancer, can arouse both posttraumatic stress and growth, the latter being related to greater spirituality.
The present study was unprecedented in assessing the correlation between various aspects of breast cancer treatment, with responses to the SRCOPE and WHOQOL-SRPB scales. Search for meaning and spiritual support was found to be correlated with immediate reconstructive surgery. Furthermore, the presence of religious actions with axillary lymphadenectomy, as well as hope and optimism with adjuvant chemotherapy.
Hypothetically, these connections may be related to expectation toward less mutilating treatment, with immediate reconstructive surgery, and toward cure, with adjuvant chemotherapy and axillary lymphadenectomy. Gall and Bilodeau assessed women before, during, and up to 1 year of surveillance after breast cancer treatment, and demonstrated that attachment to God remained stable and secure in the context of a stressor.
It is traditionally expected for older and married women to have higher degrees of religiosity/spirituality. However, like the results obtained by Majda et al., this study found no difference between the degree of spirituality/religiosity and marital status or educational level.
The present study also correlated search for meaning and religious actions with spiritism. Although not including spiritists, a study by Johnstone et al.
Spirituality and religiosity were also associated with fewer side effects to treatment, such as fatigue, pain, dyspnea, insomnia, poor appetite, and diarrhea.
Accordingly, the inclusion of religious/spiritual practices as a strategy to improve quality of life during cancer treatment should be discussed. This is a demand also perceived by oncology patients, who consider the recognition of spiritual needs an important part of treatment.
Online forms brought new perspectives that facilitated contact between researchers and patients even during the pandemic. Due to restrictions on the mobilization of patients and researchers during the COVID-19 pandemic, there was a reduction in recruitment, especially in older patients and those who did no know how to participate in the study remotely through an electronic device. Another barrier to the study were issues with personal information, such as outdated or missing e-mail and/or contact phone numbers, registered data that belonged to relatives and not to the patient, and misgivings when receiving a link to access the questionnaires. These limitations can be reviewed for the development of future studies to obtain a larger sample size.
It was found that spirituality and religiosity were important tools for patients to face cancer diagnosis and treatment. Seeking a religious or prayer house, as well as protection, love, and closeness to God or spiritual entities, the laying on of hands, prayers, meditation, and comfort through religious literature were present in their lives. It was also possible to demonstrate the need to identify the religious and spiritual needs of patients to create more comprehensive strategies and improve quality of life during and after cancer treatment.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Makluf, A SD and Dias, R C and Barra, AdA. Quality of life assessment in women with breast cancer [Avaliação da qualidade de vida em mulheres com câncer da mama]. Rev Bras Cancerol [online]. 2006, vol. 52, p. 49-58. https://doi.org/10.32635/2176-9745.RBC.2006v52n1.1909 Ver referência
2. Minayo, MCdS and Hartz, ZMdA and Buss, P M. Qualidade de vida e saúde: um debate necessário. Cien Saude Colet [online]. 2000, vol. 5, p. 7-18. https://doi.org/10.1590/S1413-81232000000100002 Ver referência
3. Sales, C and Paiva, L and Scandiuzzi, D and Anjos, A. Quality of Life of Breast Cancer Survivors: Social Functioning [Qualidade de vida de mulheres tratadas de câncer de mama: funcionamento social]. Rev Bras Cancerol [online]. 2001, vol. 47, p. 263-272. https://doi.org/10.32635/2176-9745.RBC.2001v47n3.2304 Ver referência
4. [online]. Available from: <https://www.iarc.who.int/cancer-type/breast-cancer/>.
5. Miller, K D and Siegel, R L and Lin, C C and Mariotto, A B and Kramer, J L and Rowland, J H. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin [online]. 2016, vol. 66, p. 271-289. https://doi.org/10.3322/caac.21349 Ver referência
6. . Cited: Dec 6, 2023 [online]. Available from: <https://www.gov.br/inca/pt-br/assuntos/cancer/numeros/estimativa/sintese-de-resultados-e-comentarios>.
7. . Cited: Dec 6, 2023 [online]. Available from: <https://www.gov.br/inca/pt-br/assuntos/gestor-e-profissional-de-saude/controle-do-cancer-de-mama/dados-e-numeros/mortalidade>.
8. Schreiber, J A and Brockopp, D Y. Twenty-five years later–what do we know about religion/spirituality and psychological well-being among breast cancer survivors? A systematic review. J Cancer Surviv [online]. 2012, vol. 6, p. 82-94. https://doi.org/10.1007/s11764-011-0193-7 Ver referência
9. Nguyen, J and Popovic, M and Chow, E and Cella, D and Beaumont, J L and Chu, D. EORTC QLQ-BR23 and FACT-B for the assessment of quality of life in patients with breast cancer: a literature review. J Comp Eff Res [online]. 2015, vol. 4, p. 157-166. https://doi.org/10.2217/cer.14.76 Ver referência
10. Ho, P J and Gernaat, S AM and Hartman, M and Verkooijen, H M. Health-related quality of life in Asian patients with breast cancer: a systematic review. BMJ Open [online]. 2018, vol. 8, p. e020512. https://doi.org/10.1136/bmjopen-2017-020512 Ver referência
11. Brady, M J and Cella, D F and Mo, F and Bonomi, A E and Tulsky, D S and Lloyd, S R. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J Clin Oncol [online]. 1997, vol. 15, p. 974-986. https://doi.org/10.1200/JCO.1997.15.3.974 Ver referência
12. Ferreira, L F and Freire, AdP and Silveira, A LC. A Influência da Espiritualidade e da Religiosidade na Aceitação da Doença e no Tratamento de Pacientes Oncológicos: Revisão Integrativa da Literatura. Rev Bras Cancerol [online]. 2020, vol. 66, p. 1-13. https://doi.org/10.32635/2176-9745.RBC.2020v66n2.422 Ver referência
13. Majda, A and Szul, N and Kołodziej, K and Wojcieszek, A and Pucko, Z and Bakun, K. Influence of Spirituality and Religiosity of Cancer Patients on Their Quality of Life. Int J Environ Res Public Health [online]. 2022, vol. 19, p. 4952. https://doi.org/10.3390/ijerph19094952 Ver referência
14. Panzini, R G and Bandeira, D R. Spiritual/religious coping scale (SRCOPE Scale): elaboration and construct validation [Escala de coping religioso-espiritual (Escala CRE): elaboração e validação de construto]. Psicol Estud [online]. 2005, vol. 10, p. 507-516. https://doi.org/10.1590/S1413-73722005000300019 Ver referência
15. Panzini, R G and Maganha, C and da Rocha, N S and Bandeira, D R and Fleck, M P. Validação brasileira do Instrumento de Qualidade de Vida/espiritualidade, religião e crenças pessoais. Rev Saude Publica [online]. 2011, vol. 45, p. 153-165. https://doi.org/10.1590/S0034-89102011000100018 Ver referência
16. Vallurupalli, M and Lauderdale, K and Balboni, M J and Phelps, A C and Block, S D and Ng, A K. The role of spirituality and religious coping in the quality of life of patients with advanced cancer receiving palliative radiation therapy. J Support Oncol [online]. 2012, vol. 10, p. 81-87. https://doi.org/10.1016/j.suponc.2011.09.003 Ver referência
17. Tate, D G and Forchheimer, M. Quality of life, life satisfaction, and spirituality: comparing outcomes between rehabilitation and cancer patients. Am J Phys Med Rehabil [online]. 2002, vol. 81, p. 400-410. https://doi.org/10.1097/00002060-200206000-00002 Ver referência
18. Gall, T L and Guirguis-Younger, M and Charbonneau, C and Florack, P. The trajectory of religious coping across time in response to the diagnosis of breast cancer. Psychooncology [online]. 2009, vol. 18, p. 1165-1178. https://doi.org/10.1002/pon.1495 Ver referência
19. Gall, T L and de Renart, R MM and Boonstra, B. Religious Resources in Long-Term Adjustment to Breast Cancer. J Psychosoc Oncol [online]. 2000, vol. 18, p. 21-37. https://doi.org/10.1300/J077v18n02_02 Ver referência
20. Schreiber, J A. Image of God: effect on coping and psychospiritual outcomes in early breast cancer survivors. Oncol Nurs Forum [online]. 2011, vol. 38, p. 293-301. https://doi.org/10.1188/11.ONF.293-301 Ver referência
21. Purnell, J Q and Andersen, B L and Wilmot, J P. Religious Practice and Spirituality in the Psychological Adjustment of Survivors of Breast Cancer. Couns Values [online]. 2009, vol. 53, p. 165. https://doi.org/10.1002/j.2161-007X.2009.tb00123.x Ver referência
22. Paredes, A C and Pereira, M G. Spirituality, Distress and Posttraumatic Growth in Breast Cancer Patients. J Relig Health [online]. 2018, vol. 57, p. 1606-1617. https://doi.org/10.1007/s10943-017-0452-7 Ver referência
23. Gall, T L and Bilodeau, C. Attachment to God and coping with the diagnosis and treatment of breast cancer: a longitudinal study. Support Care Cancer [online]. 2020, vol. 28, p. 2779-2788. https://doi.org/10.1007/s00520-019-05149-6 Ver referência
24. Johnstone, B and Yoon, D P and Cohen, D and Schopp, L H and McCormack, G and Campbell, J and Smith, M. Relationships among spirituality, religious practices, personality factors, and health for five different faith traditions. J Relig Health [online]. 2012, vol. 51, p. 1017-1041. https://doi.org/10.1007/s10943-012-9615-8 Ver referência
25. Brandão, M L and Fritsch, T Z and Toebe, T RP and Rabin, E G. Association between spirituality and quality of life of women with breast cancer undergoing radiotherapy. Rev Esc Enferm USP [online]. 2021, vol. 55, p. e20200476. https://doi.org/10.1590/1980-220X-REEUSP-2020-0476 Ver referência
26. Sheppard, V B and Walker, R and Phillips, W and Hudson, V and Xu, H and Cabling, M L. Spirituality in African-American Breast Cancer Patients: Implications for Clinical and Psychosocial Care. J Relig Health [online]. 2018, vol. 57, p. 1918-1930. https://doi.org/10.1007/s10943-018-0611-5 Ver referência
27. Toledo, G and Ochoa, C Y and Farias, A J. Religion and spirituality: their role in the psychosocial adjustment to breast cancer and subsequent symptom management of adjuvant endocrine therapy. Support Care Cancer [online]. 2021, vol. 29, p. 3017-3024. https://doi.org/10.1007/s00520-020-05722-4 Ver referência
28. Kang, K A and Kim, S J. Spiritual Care Expectations Among Cancer and Noncancer Patients with Life-Threatening Illnesses. Cancer Nurs [online]. 2023, vol. 47, p. E269-E278. https://doi.org/10.1097/NCC.0000000000001213 Ver referência
29. Park, S and Sato, Y and Takita, Y and Tamura, N and Ninomiya, A and Kosugi, T. Mindfulness-Based Cognitive Therapy for Psychological Distress, Fear of Cancer Recurrence, Fatigue, Spiritual Well-Being, and Quality of Life in Patients With Breast Cancer-A Randomized Controlled Trial. J Pain Symptom Manage [online]. 2020, vol. 60, p. 381-389. https://doi.org/10.1016/j.jpainsymman.2020.02.017 Ver referência
30. Greenlee, H and DuPont-Reyes, M J and Balneaves, L G and Carlson, L E and Cohen, M R and Deng, G. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin [online]. 2017, vol. 67, p. 194-232. https://doi.org/10.3322/caac.21397 Ver referência
31. Cramer, H and Lauche, R and Klose, P and Lange, S and Langhorst, J and Dobos, G J. Yoga for improving health-related quality of life, mental health and cancer-related symptoms in women diagnosed with breast cancer. Cochrane Database Syst Rev [online]. 2017, vol. 2017, p. CD010802. https://doi.org/10.1002/14651858.CD010802.pub2 Ver referência
32. Breitbart, W. Spirituality and meaning in supportive care: spirituality- and meaning-centered group psychotherapy interventions in advanced cancer. Support Care Cancer [online]. 2002, vol. 10, p. 272-280. https://doi.org/10.1007/s005200100289 Ver referência
Dados de acesso insuficientes para visualização no mapa.