Cancer patients face challenges that go beyond the tumor, including malnutrition. Malnutrition can be defined as a state resulting from a deficit of nutrients that leads to changes in body composition, mental state, and function; can damage the clinical outcome; and has a multifactorial etiology.
Unintentional weight loss in hospitalized patients used in isolation is already a negative prognostic indicator, and studies indicate that approximately 31-87% of individuals diagnosed with cancer show substantial loss of body weight, which is a marker for malnutrition.
Currently, it is estimated that, on average, the malnutrition rate in cancer patients varies from 20% to 80%; in addition, approximately 20% of cancer patients die due to malnutrition/cachexia.
The main complications related to malnutrition include a delay in the healing process; impaired absorption and binding of proteins, hepatic metabolism, and renal elimination of drugs and their metabolites; worsening of the immune response; increased rates of infections and postoperative complications; increased risk of developing pressure injury; increased length of hospital stay; increased risk of mortality; and a considerable increase in hospital costs. In addition to negatively impacting patient metabolism, involution of the nutritional status can also affect cancer treatment outcomes.
An epidemiological study carried out in Spain showed through the Global Subjective Assessment produced by the patient (ASG-PPP) that 96.7% of the patients were at nutritional risk and lacked early nutritional intervention. The authors observed that the patients with the greatest weight loss were those with tumors in the esophagus, stomach, or larynx.
Nutritional support aims to significantly improve the response to treatment, contain weight loss and malnutrition, reduce the risk of complications, reduce morbidity and mortality, and provide a better quality of life for cancer patients. Among nutritional interventions, oral nutritional therapy (ONT) has been highlighted as its main objective is to increase the patient’s dietary intake.
Oral nutritional supplements (ONS) are the main pillar of ONT. Available for oral consumption, these supplements can be found in ready-to-eat models (in tetra-pack packaging or in cans) or in powder form for reconstitution, and they are intended to complement food intake. ONS are indicated for patients who do not achieve their food intake requirements or for those who show weight loss; thus, their use helps the patients to recover their nutritional status.[14] Supplements are considered as the first option, since they have physiological properties and are less invasive than other treatment methods; however, they should only be used as an aid for recovery or maintenance of nutritional status and not as an exclusive method of feeding or replacing meals.
There are several types of nutritional supplements, which are divided into standard and specialized formulas, according to their purpose and composition. Currently, the nutritional supplement industry has a wide variety of products, including normal to hypercaloric; normal to hyperprotein; free of sucrose or sugar; fortified with immunomodulatory nutrients; free or high in fat; with or without flavor; with or without dietary fiber; and even products aimed at certain audiences or those with specific clinical conditions such as cancer patients, those with kidney or liver failure, among others.
Several studies indicate that nutritional intervention should be an adjunct to cancer treatment. Moreover, a multidisciplinary approach allows better adherence to ONT, which is a key factor for successful treatment and recovery of patients.
A previous study has evaluated 13 randomized clinical trials of oral nutritional intervention (nutrition counseling, ONT, or both) in patients diagnosed with cancer at nutritional risk/malnourished during anticancer treatment or palliative care and compared oral nutritional intervention with usual care.
According to Paccagnella et al. (2010)
Additionally, a retrospective study that aimed to evaluate the impact of nutritional supplementation on the length of hospital stay, hospital costs, and readmission of the patient showed that the use of ONS reduced the length of hospital stay by an average of 2-3 days, reduced hospital costs by US$4,734, and decreased the probability of these patients being readmitted within 30 days of discharge.
In practice, ONT requires multidisciplinary work, considering that each specialty is responsible for a different part of the process. For example, the Medicine Department (except for professional nutritionists) is often the area in charge of prescribing supplements, and nurses and their assistants are responsible for their delivery and administration. However, these specialties have different views on supplementation; supplements can be considered as a medicine or as a product that supplements nutrition. The different understandings about the purpose of the supplement, when passed on to the patient, can cause some confusion about its real benefit; moreover, a variable representation about such a relevant treatment has an impact on the importance of ONT, resulting in increased efforts to be made to prevent or treat malnutrition and to plan follow-up care.
It is essential that nutritional care is present from the early stages of the disease’s natural history, and its integration in the therapeutic strategy in the battle against cancer is essential.
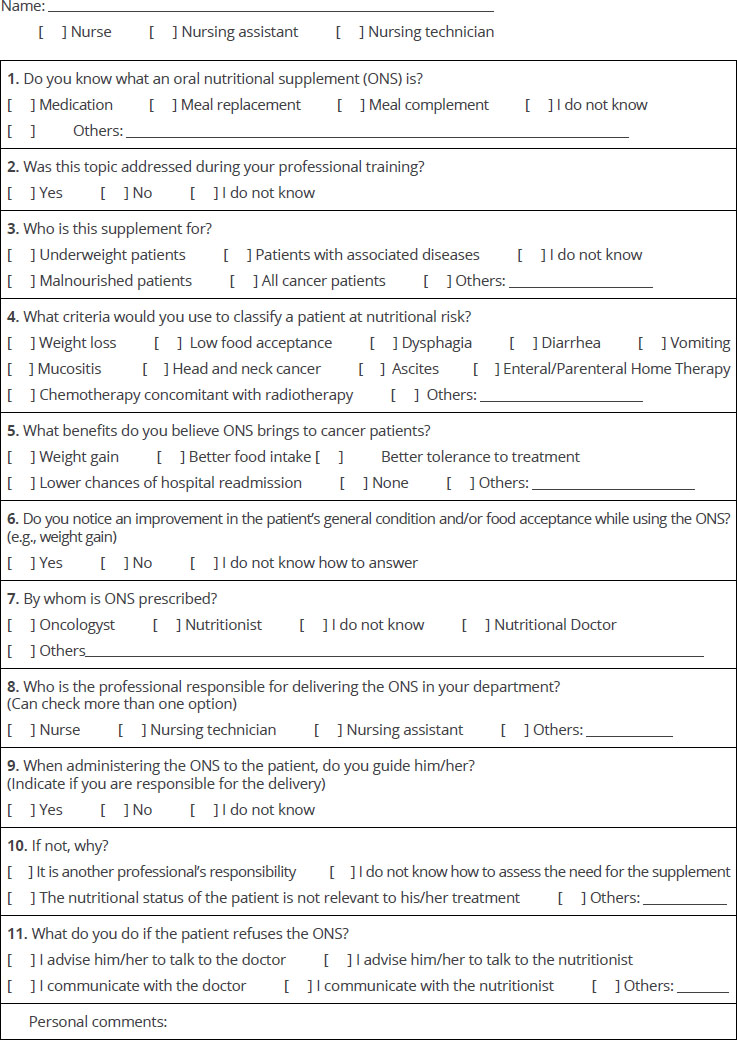
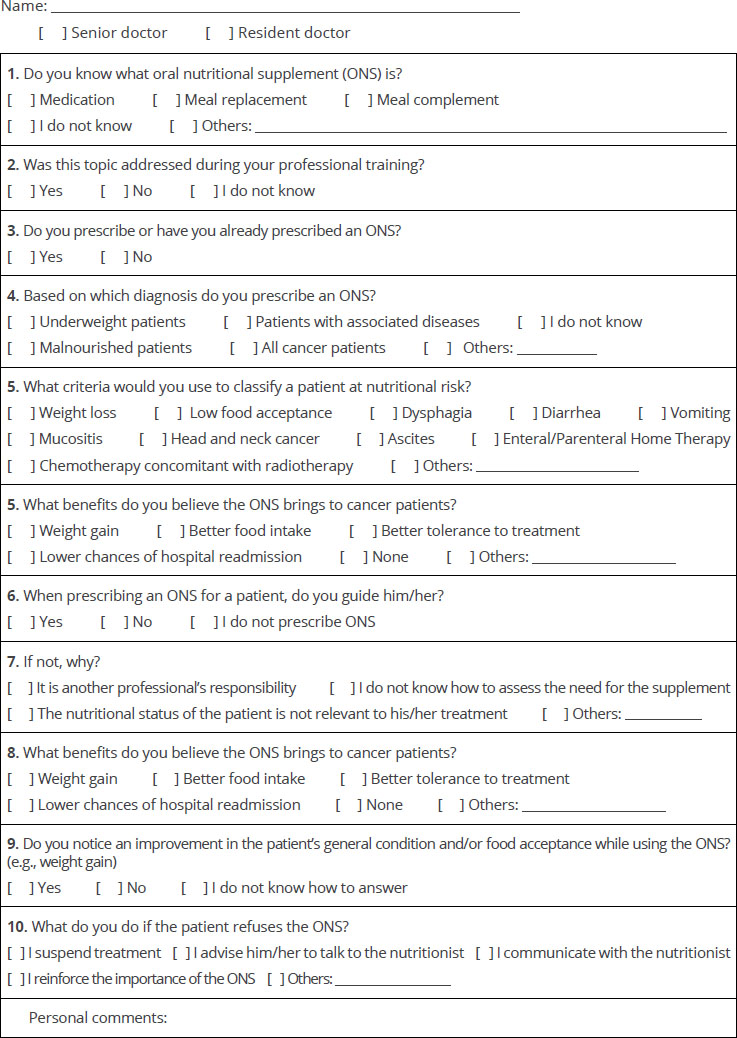
This was a descriptive cross-sectional study. Data collection was performed through the application of a semi-structured questionnaire (
All participants completed the free and informed consent form prior to completing the questionnaires. The administration of the questionnaires was carried out between October and December 2020.
Physicians and nurses were invited to answer a semi-structured questionnaire that included questions regarding their profession and specialty, what ONS means to them, knowledge of the importance of ONT for the patient, whether this topic was addressed during their professional training, modalities and personal safety for prescription (physicians), conduct towards ONT, self-confidence to resolve possible doubts from patients, and open questions/criticisms and suggestions if the professional feels the need to report something that was not addressed.
Statistical analysis was performed using the software package IBM SPSS Statistic, version 22.0 (Chicago, IL, USA). Continuous variables were presented as the median or mean and standard deviation for non-normally and normally distributed data, respectively. Normality was tested using the Kolmogorov-Smirnov test. Ordinal or nominal variables were presented in absolute numbers and as a percentage of the total. Absolute and relative frequencies were calculated for categorical variables. For the analysis of categorical variables, the chi-squared test or Fisher’s exact test was used, when appropriate. Comparison of the averages of continuous variables between the evaluation methods was performed using the Student’s t-test or the nonparametric Mann-Whitney test for independent samples, as appropriate.
A total of 105 professionals were included in this study, including 34 physicians (32.4%) and 71 nursing staff (67.6%). Among the nursing staff, 35 were nursing technicians (33.3%), 35 were nurses (33.3%), and only 1 was a nursing assistant (1%). In the physician category, 11 were physicians (10.5%), and 23 were residents (21.9%).
| Variable | Category | N (%) |
|---|---|---|
| Do you know what ONS is? | Medication | 0 |
| Meal replacement | 1 (1.4) | |
| Meal complement | 68 (95.8) | |
| I do not know | 2 (2.8) | |
| Was this topic addressed during your professional training? | Yes | 30 (42.9) |
| No | 34 (48.6) | |
| I do not know | 6 (8.6) | |
| Who is this supplement for? | Underweight patients | 31 (43.7) |
| Patients with associated diseases | 8 (11.3) | |
| I do not know | 7 (9.9) | |
| Malnourished patients | 40 (56.3) | |
| All cancer patients | 9 (12.7) | |
| What criteria would you use to classify a patient at nutritional risk? | Weight loss | 61 (85.9) |
| Low food acceptance | 62 (87.3) | |
| Dysphagia | 38 (53.5) | |
| Diarrhea | 33 (46.5) | |
| Vomiting | 30 (42.3) | |
| Mucositis | 35 (49.3) | |
| Head and neck cancer | 30 (42.3) | |
| Ascites | 12 (16.9) | |
| Enteral/Parenteral home therapy | 20 (28.2) | |
| Chemotherapy concomitant with radiotherapy | 19 (26.8) | |
| What benefits do you believe the ONS brings to cancer patients? | Weight gain | 56 (78.9) |
| Better food intake | 37 (52.1) | |
| Better tolerance to treatment | 46 (64.8) | |
| Lower chances of hospital readmission | 19 (26.8) | |
| None | 0 | |
| Do you notice an improvement in the patient’s general condition and/or food acceptance while using the ONS? | Yes | 48 (67,6) |
| No | 5 (7,0) | |
| I do not know | 18 (25,4) | |
| By whom is ONS prescibed? | Doctor | 11 (15,5) |
| Nutricionist | 62 (87,3) | |
| I do not know | 1 (1,4) | |
| Nutritional Doctor | 31 (43,7) | |
| Who is the professional responsible for delivering the ONS in your department? | Nurse | 18 (25,4) |
| Nursing technician | 62 (87,3) | |
| Nursing assistant | 25 (35,2) | |
| When administering the ONS to the patient, do you guide him? | Yes | 53 (79,1) |
| No | 10 (14,9) | |
| I do not know | 4 (6,0) | |
| If not, why? | It is another professional’s responsibility | 5 (35,7) |
| I do not know how to assess the need for the supplement | 4 (28,6) | |
| The nutritional status of the patient is not relevant to his/her treatment | 0 | |
| What do you do if the patient refuses the ONS? | I advise him/her to talk to the doctor | 4 (5,6) |
| I advise him/her to talk to the nutritionist | 47 (66,2) | |
| I communicate the doctor | 6 (8,5) | |
| I communicate the nutritionist | 40 (56,3) |
Legend: ONS: Oral nutritional supplements.
| Variable | Category | N (%) |
|---|---|---|
| Do you know what ONS is? | Medication | 0 |
| Meal replacement | 1 (2,9) | |
| Meal complement | 33 (95,8) | |
| I do not know | 0 | |
| Was this topic addressed during your professional | Yes | 9 (26,5) |
| No | 25 (73,5) | |
| I do not know | 0 | |
| Do you prescribe or have you already prescribe an ONS? | Yes | 18 (52,9) |
| No | 16 (47,1) | |
| Based on which diagnosis do you prescribe the ONS? | Underweight patients | 12 (35,3) |
| Patients with associated diseases | 1 (2,9) | |
| I do not know | 7 (20,6) | |
| Malnourished patients | 20 (58,8) | |
| All cancer patients | 2 (5,9) | |
| What criteria would you use to classify a patient at nutritional risk? | Weight loss | 34 (100,0) |
| Low food acceptance | 31 (91,2) | |
| Dysphagia | 23 (67,6) | |
| Diarrhea | 17 (50,0) | |
| Vomiting | 16 (47,1) | |
| Mucositis | 22 (64,7) | |
| Head and neck cancer | 21 (61,8) | |
| Ascites | 10 (29,4) | |
| Enteral/Parenteral home therapy | 13 (38,2) | |
| Chemotherapy concomitant with radiotherapy | 16 (47,1) | |
| When prescribing the ONS to the patient, do you guide him/her? | Yes | 13 (38,2) |
| No | 7 (20,6) | |
| I do not prescribe ONS | 14 (41,2) | |
| If not, why? | It is another professional’s responsibility | 9 (42,9) |
| I don’t know how to assess the need for the supplement | 12 (57,1) | |
| The nutritional status of the patient is not relevant to his/her treatment | 0 | |
| What benefits do you believe the ONS brings to cancer patients? | Weight gain | 26 (76,5) |
| Better food intake | 12 (35,3) | |
| Better tolerance to treatment | 28 (82,4) | |
| Lower chances of hospital readmission | 26 (76,5) | |
| None | 0 | |
| Do you notice an improvement in the patient’s general condition and/or food acceptance while using the ONS? | Yes | 27 (79,4) |
| No | 1 (2,9) | |
| I do not know | 6 (17,6) | |
| What do you do if the patient refuses the ONS? | I suspend | 1 (2,9) |
| I advise him/her to talk to the nutritionist | 21 (61,8) | |
| I communicate the nutritionist | 4 (11,8) | |
| I reinforce the importance of the ONS | (23,5) |
Legend: ONS: Oral nutritional supplements.
| Variable | Category | Doc. N (%) | Nur. N (%) | p-value |
|---|---|---|---|---|
| Do you know what ONS is? | Medication | 0 | 0 | |
| Meal replacement | 1 (2,9) | 1 (1,4) | 1,000 | |
| Meal complement | 33 (95,8) | 68 (95,8) | ||
| I do not know | 0 | 2 (2,8) | ||
| Was this topic addressed during | Yes | 9 (26,5) | 30 (42,9) | |
| your professional training? | No | 25 (73,5) | 34 (48,6) | 0,028 |
| I do not know | 0 | 6 (8,6) | ||
| Based on which diagnosis do you prescribe the ONS? | Underweight patients | 12 (35,3) | 31 (43,7) | 0,546 |
| Who is this supplement for? | Patients with associated diseases | 1 (2,9) | 8 (11,3) | 0,266 |
| I do not know | 7 (20,6) | 7 (9,9) | 0,140 | |
| Malnutrition patients | 20 (58,8) | 40 (56,3) | 0,976 | |
| All cancer patients | 2 (5,9) | 9 (12,7) | 0,497 | |
| What criteria would you use to classify | Weight loss | 34 (100,0) | 61 (85,9) | 0,028 |
| a patient at nutritional risk? | Low food acceptance | 31 (91,2) | 62 (87,3) | 0,747 |
| Dysphagia | 23 (67,6) | 38 (53,5) | 0,245 | |
| Diarrhea | 17 (50,0) | 33 (46,5) | 0,897 | |
| Vomiting | 16 (47,1) | 30 (42,3) | 0,799 | |
| Mucositis | 22 (64,7) | 35 (49,3) | 0,203 | |
| Head and neck cancer | 21 (61,8) | 30 (42,3) | 0,096 | |
| Ascites | 10 (29,4) | 12 (16,9) | 0,223 | |
| Enteral/Parenteral home therapy | 13 (38,2) | 20 (28,2) | 0,415 | |
| Chemotherapy concomitant with radiotherapy | 16 (47,1) | 19 (26,8) | 0,065 | |
| What benefits do you believe the ONS | Weight gain | 26 (76,5) | 56 (78,9) | 0,979 |
| brings to cancer patients? | Better food intake | 12 (35,3) | 37 (52,1) | 0,159 |
| Better tolerance to treatment | 28 (82,4) | 46 (64,8) | 0,106 | |
| Lower chances of hospital readmission | 26 (76,5) | 19 (26,8) | < 0,001 | |
| None | 0 | 0 | 1,000 | |
| Do you notice an improvement in the | Yes | 27 (79,4) | 48 (67,6) | 0,502 |
| patient’s general condition and/or | No | 1 (2,9) | 5 (7,0) | 0,502 |
| acceptance while using the ONS? | I do not know | 6 (17,6) | 18 (25,4) | |
| When prescribing the ONS to the patient, do you guide him/her? | Yes | 13 (38,2) | 53 (79,1) | |
| When administering the ONS to the patient, do you guide him/her? | No | 7 (20,6) | 10 (14,9) | |
| I do not know | - | 4 (6,0) | < 0,001 | |
| I do not prescribe ONS | 14 (41,2) | - | ||
| If not, why? | It’s another professional’s assigment | 9 (42,9) | 5 (35,7) | |
| I don’t know how to assess the need for the supplement | 12 (57,1) | 4 (28,6) | 0,012 | |
| The nutritional status of the patient is not relevant to his treatment | 0 | 0 |
Legend: ONS, oral nutritional supplements; Doc, doctors; Nur, nursing;
p-value< 0,005 According to Fisher’s exact test.
The adherence of patients to ONT as a way to prevent and cope with malnutrition is directly linked to the knowledge of the team involved in the prescription, administration, and guidance of the patient, since they are responsible for transmitting all the necessary information for such a treatment. A team that does not have a unified view can create confusion for the main beneficiary of the treatment: the patient; this can lead to a reduced effectiveness and a poor adherence to the treatment by the patient.
A systematic review by Baldwin et al. (2012)[18] suggests that the use of ONS is associated with significant reductions in complications associated with unintentional weight loss, length of hospital stay, and mortality rates. Therefore, nutritional assistance is a great ally against malnutrition. In addition, the report on recommending procedures for ONS for malnourished clinical or surgical patients or those at risk of malnutrition prepared by the Ministry of Health of Brazil
Although doctors have the view that one of the benefits of ONS is the decrease in the chances of hospital readmission, most of the nursing team does not believe in this benefit. A study directed by Kaegi-Braun et al. (2021)
In contrast to the results obtained by Brindisi et al. (2020)
The nutritional risk criteria used in the questionnaires were based on a proprietary institutional tool. This study points out that several symptoms and conditions are neglected by professionals. For example, the presence of ascites, defined as the presence of free fluid of pathological origin in the abdominal cavity,
The professionals also did not believe that patients with comorbidities, such as diabetes mellitus, would benefit from ONS. According to the Guidelines of the Brazilian Society of Diabetes,
Physicians participating in this study collectively believed that patients who present with weight loss are eligible to receive ONS; however, in clinical practice, most patients are referred for nutritional monitoring only when there is a severe loss of weight. There are also many patients who are not provided with nutritional consultation and do not receive a medical prescription for food support. A study by Lorton et al. (2020)
Although the literature is clear regarding the nutritional status depletion that systemic treatment can cause, physicians and nurses in this study believe that there are no such negative effects. However, Carniatto et al. (2018)
Physicians as well as nurses and technicians do not consider enteral and parenteral nutritional therapy at home as a risk factor for malnutrition; however, the presence of nutritional support is not synonymous with the treatment being adequate. Mazur et al. (2014)
Even without training on the proposed subject, most physicians and nursing staff notice the improvement in the nutritional status of patients who use ONS. However, even without adequate training, they felt able to guide patients regarding the consumption of ONS that they prescribed and administered, respectively. These findings corroborate the results presented by Spiro et al. (2016),
When nutritional care takes place in a multidisciplinary way, health outcomes are more favorable to the patient’s quality of life. Such care should involve all health professionals such as dietitians, physicians, and nurses at all levels of care involving nutritional screening, assessment, planning, implementation, evaluation and ultimately the monitoring of evidence- based care delivery.
The study by Vrkatić et al. (2022)
Continuing education in cancer nutrition is essential for every multidisciplinary team, since nutrition is an important part of treatment and not just a complement.[36] Nutritional education interventions, such as the creation of workshops, protocols and discussion of clinical cases, increase the quality of nutritional therapy, this study also points out that there was an improvement in clinical practice after the application of training for physicians, impacting on a shorter period of fasting and greater achievement of nutritional goals.
Nutritional diagnosis must be carried out in parallel with disease diagnosis so that early nutritional intervention is possible, thus affording better clinical outcomes.
The present study has some limitations, such as the use of a questionnaire designed for this study, based on other similar research, but not validated. In addition, the research was conducted with only one medical specialty, since other specialties, such as surgeons, have greater knowledge about nutritional supplements due to institutional protocols that encompass this type of nutritional therapy. Finally, the nursing staff evaluated was only those who had care with the inpatient.
There is a great difference in knowledge about ONS among medical and nursing professionals. Interdisciplinary technical training is essential for the success of ONT as a tool for preventing and combating malnutrition. Although nutrition is not a part of the curriculum in other areas of health care, hospitals must carry out training to improve knowledge regarding this topic so that ONT can be implemented.
TMM Final approval of manuscript, Manuscript writing
CRK Collection and assembly of data, Conception and design, Data analysis wand interpretation, Final approval of manuscript, Manuscript writing
JPF Final approval of manuscript, Manuscript writing
Appendix 1 – Questionnaire for Nursing Staff
Appendix 2 – Questionnaire for Medical Staff
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Toledo, DO and Piovacari, SMF and Horie, LM and Matos, LBN and Castro, MG and Ceniccola, GD. Campanha ‘Diga não à desnutrição’: 11 passos importantes para combater a desnutrição hospitalar. BRASPEN J [online]. 2018, vol. 33, p. 86-100.
2. Cederholm, T and Bosaeus, I and Barazzoni, R and Bauer, J and Van Gossum, A and Klek, S. Diagnostic criteria for malnutrition. ESPEN Consensus Statement. Clin Nutr [online]. 2015, vol. 34, p. 335-40.
3. Cederholm, T and Jensen, GL and Correia, MITD and Gonzalez, MC and Fukushima, R and Higashiguchi, T. GLIM criteria for the diagnosis of malnutrition - a consensus report from the global clinical nutrition community. Clin Nutr [online]. 2019, vol. 38, p. 9-1.
4. Uster, A and Ruefenacht, U and Ruehlin, M and Pless, M and Siano, M and Haefner, M. Influence of a nutritional intervention on dietary intake and quality of life in cancer patients: a randomized controlled trial. Rev Nutr [online]. 2013, vol. 29, p. 1342-9.
5. Muscaritoli, M and Lucia, S and Farcomeni, A and Lorusso, V and Saracino, V and Barone, C. Prevalence of malnutrition in patients at first medical oncology visit: the PreMiO study. Oncotarget [online]. 2017, vol. 8, p. 79884-96.
6. Arends, J and Bachmann, P and Baracos, V and Barthelemy, N and Bertz, H and Bozzetti, F. ESPEN guidelines on nutrition in cancer patients. Clin Nutr [online]. 2017, vol. 36, p. 11-48.
7. Muscaritoli, M and Molfino, A and Gioia, G and Laviano, A and Fanelli, FR. The “parallel pathway”: a novel nutritional and metabolic approach to cancer patients. Intern Emerg Med [online]. 2011, vol. 6, p. 105-12. https://doi.org/10.1007/s11739-010-0426-1 Ver referência
8. Khalatbari-Soltani, S and Marques-Vidal, P. The economic cost of hospital malnutrition in Europe; a narrative review. Clin Nutr ESPEN [online]. 2015, vol. 10, p. e89-e94.
9. Zhang, X and Tang, T and Pang, L and Sharma, SV and Li, R and Nyitray, AG. Malnutrition and overall survival in older adults with cancer: a systematic review and meta-analysis. J Clin Oncol [online]. 2019, vol. 10, p. 874-83.
10. Segura, A and Pardo, J and Jara, C and Zugazabeitia, L and Carulla, J and Peñas, RDL. An epidemiological evaluation of the prevalence of malnutrition in Spanish patients with locally advanced or metastatic cancer. Clin Nutr [online]. 2005, vol. 24, p. 801-814.
11. Pelissaro, E and Damo, CC and Alves, ALS and Calcing, A and Kümpel, DA. Avaliação do estado nutricional em pacientes idosos oncológicos internados em um hospital de alta complexidade do Norte do Rio Grande do Sul. Sci Med [online]. 2016, vol. 26, p. ID22972.
12. Cibulski, TP and Becker, T and Baldissera, C and Basso, T and Kumpel, DA. Adesão à terapia nutricional oral de pacientes com neoplasias de cabeça e pescoço. BRASPEN J [online]. 2018, vol. 33, p. 215-20.
13. Piovacari, SMF and Barrére, APN. Nutrição clínica na oncologia. Atheneu, 2019.
14. Silva, MBR and Santos, HMC and Oliveira, AF. Características sensoriais e nutricionais de suplementos alimentares. Ciênc Biol Saúde [online]. 2014, vol. 35, p. 31-8.
15. Terapia nutricional oral. Atheneu, 2017.
16. Macrotema de Alimentos. Ministério da Saúde/Anvisa, 2020.
17. Ravasco, P. Nutrition in cancer patients. J Clin Med [online]. 2019, vol. 8, p. 1211.
18. Baldwin, C and Spiro, A and Ahern, R and Emery, PW. Oral nutritional interventions in malnourished patients with cancer: a systematic review and meta-analysis. J Natl Cancer Inst [online]. 2012, vol. 104, p. 371-85. https://doi.org/10.1093/jnci/djr556 Ver referência
19. Paccagnella, A and Morello, M and Mosto, MC and Baruffi, C and Marcon, ML and Gava, A. Early nutritional intervention improves treatment tolerance and outcomes in head and neck cancer patients undergoing concurrent chemoradiotherapy. Support Care Cancer [online]. 2010, vol. 18, p. 837-45.
20. Philipson, TJ and Snider, JT and Lakdawalla, DN and Stryckman, B and Goldman, DP. Impact of oral nutritional supplementation on hospital outcomes. Am J Manag Care [online]. 2013, vol. 19, p. 121-8.
21. Brindisi, MC and Noacco, A and Hansal, AAB and Gential, CH. Delivery of oral nutrition supplement in hospital: Evaluation of professional practices in evaluation of nutritional status and representations of ONS by the caregivers and patients. Clin Nutr ESPEN [online]. 2020, vol. 35, p. 85-9.
22. Muscaritoli, M and Molfino, A and Gioia, G and Laviano, A and Fanelli, FR. The “parallel pathway”: a novel nutritional and metabolic approach to cancer patients. Intern Emerg Med [online]. 2011, vol. 6, p. 105-12.
23. Ministério da Saúde (BR). Secretaria de Ciência, Tecnologia, Inovação e Insumos Estratégicos em Saúde. Suplementação nutricional oral para pacientes clínicos ou cirúrgicos desnutridos ou em risco de desnutrição. Ministério da Saúde, 2021.
24. Kaegi-Braun, N and Mueller, M and Schuetz, P and Mueller, B and Kutz, A. Evaluation of nutritional support and in-hospital mortality in patients with malnutrition. JAMA Network Open [online]. 2021, vol. 4, p. e2033433.
25. Júnior, DRA and Galvão, FHF and Santos, SA. Ascite – Estado baseado em evidências. Rev Assoc Med Bras [online]. 2009, vol. 55, p. 489-96.
26. Gregorini, FG and Stanich, P and Freitas, MMT. Avaliação do estado nutricional em pacientes hospitalizados com cirrose hepática. BRASPEN J [online]. 2016, vol. 31, p. 299-304.
27. Golbert, A and Vasques, ACJ and Faria, ACRA and Lottenberg, AMP and Joaquim, AG and Vianna, AGD. Diretrizes sociedade brasileira de diabetes. Clannad, 2019.
28. Lorton, CM and Griffin, O and Higgins, K and Roulston, F and Stewart, G and Gough, N. Late referral of cancer patients with malnutrition to dietitians: a prospective study of clinical practice. Support Care Cancer [online]. 2020, vol. 28, p. 2351-60.
29. Consenso nacional de nutrição oncológica. INCA, 2016.
30. Carniatto, LN and Miola, TM and Chulam, TC. Evolution of nutritional status of patients with head and neck cancer during radiotherapy or radiotherapy concerning chemotherapy. BRASPEN J [online]. 2018, vol. 33, p. 141-6.
31. Rebouças, LM and Callegaro, E and Gil, GOB and Silva, MLG and Maia, MAC and Salvajoli, JV. Impacto da nutrição enteral na toxicidade aguda e na continuidade do tratamento dos pacientes com tumores de cabeça e pescoço submetidos a radioterapia com intensidade modulada. Radiol Bras [online]. 2011, vol. 44, p. 42-6.
32. Mazur, CE and Schmidt, ST and Rigon, AS and Schieferdecker, MEM. Terapia nutricional enteral domiciliar: interface entre direito humano à alimentação adequada e segurança alimentar e nutricional. Demetra [online]. 2014, vol. 9, p. 757-69.
33. Spiro, A and Baldwin, C and Patterson, A and Thomas, J and Andreyev, HJN. The views and practice of oncologists towards nutritional support in patients receiving chemotherapy. Br J Cancer [online]. 2016, vol. 95, p. 431-4.
34. Xiaoyue, X and Parker, D and Ferguson, C and Hickman, L. Where is the nurse in nutritional care?. Contemp Nurse [online]. 2017, vol. 53, p. 267-70.
35. Vrkatić, A and Grujičić, M and Jovičić-Bata, J and Novaković, B. Nutritional knowledge, confidence, attitudes toward nutritional care and nutrition counseling practice among general practitioners. Healthcare [online]. 2022, vol. 10, p. 2222.
36. Liposits, G and Orrevall, Y and Kaasa, S and Osterlund, P and Ceder, T. Nutrition in cancer care: a brief, practical guide with a focus on clinical practice. J Oncol Pract [online]. 2021, vol. 17, p. 992-8.
37. Ferreira, HCC and Rodrigues, PL. Avaliação do conhecimento médico sobre terapia nutricional parenteral em um hospital público do Distrito Federal. BRASPEN J [online]. 2017, vol. 32, p. 387-93.
38. Muscaritoli, M and Arends, J and Bachmann, P and Baracos, V and Barthelemy, N and Bertz, H. ESPEN practical guideline: clinical nutrition in cancer. Clin Nutr [online]. 2021, vol. 40, p. 2913-98.
Dados de acesso insuficientes para visualização no mapa.