Bone metastases are common in advanced stages of cancers such as those of the prostate, breast, and lung, frequently leading to significant and progressive pain. Effective management of this pain is a critical therapeutic goal in oncology, and it typically requires a multidisciplinary approach. Palliative options include external-beam radiotherapy, analgesics, and surgery.
Radionuclide bone pain therapy is mainly indicated for patients with symptomatic bone metastases that are osteoblastic or mixed in nature. The most frequent indications are prostate cancer and breast cancer, which together account for more than 80% of the cases of bone metastasis. Approximately 65 to 75% of the patients with advanced prostate or breast cancer develop painful bone metastases during the course of their disease. Lung, thyroid, and kidney cancers may also lead to multifocal osteoblastic bone metastases that are candidates for systemic radionuclide therapy. For therapy to be indicated, there must be a correlation between the patient's pain symptoms and the presence of osteoblastic lesions on bone scintigraphy; conditions such as vertebral collapse, nerve compression, or predominantly-osteolytic lesions respond less predictably. In Brazil, Beta-emitting agents, such as Sm-153 and Sr-89, have been primarily used for these indications.
Samarium-153 has been extensively used in Brazil for the palliation of metastatic bone pain, demonstrating clinical effectiveness and favorable cost-effectiveness across public and private healthcare settings.
Radiopharmaceutical therapy enables the simultaneous treatment of multiple skeletal metastases, allows for repeated dosing, and it can be combined with other systemic treatments. Since its introduction in the 1980s, it has become an integral component of multidisciplinary palliative care.
The coronavirus disease 2019 (COVID-19) pandemic caused extensive disruptions in cancer care. In Brazil, the public and private sectors faced significant constraints: elective procedures were delayed or suspended, and resources were reallocated toward emergency response. These changes affected access to diagnostic and therapeutic services for chronic conditions, including cancer.
The impact of the COVID-19 pandemic on cancer management was multifaceted. There were dramatic reductions in diagnostic services, delays in elective surgeries, and suspension of screening programs, leading to later-stage diagnoses. Non-urgent medical visits and procedures dropped sharply, and patients often avoided healthcare settings due to fear of infection. As a result, more cases presented at advanced stages with painful bone metastases. Cancer treatments were also affected: the volumes of surgeries and systemic therapy decreased, while the use of oral regimens increased. Access to radionuclide therapy and radiotherapy was hampered by supply-chain interruptions and logistical barriers. Collectively, these effects contributed to excess mortality and increased suffering among cancer patients, even among those not directly infected with COVID-19.
Understanding how specific oncologic interventions—such as radiopharmaceutical therapy—were affected can inform future contingency planning and guide the development of health policies. The current study evaluates national trends in the use of Beta-emitting radionuclide therapy for bone pain, comparing the public (Unified Health System, Sistema Único de Saúde, SUS, in Portuguese) and private (Supplementary Health) sectors, and assessing the impact of the COVID-19 pandemic and the subsequent recovery.
The present is a retrospective observational study based on routinely-collected administrative data from national health databases in Brazil. The study was conducted and reported in accordance with the Reporting of Studies Conducted Using Observational Routinely-Collected Data (RECORD) statement, an extension of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline tailored for studies using secondary health data.
Data from the SUS were obtained from its Computer Sciences Department (Departamento de Informática do SUS, DATASUS, in Portuguese), specifically the Outpatient Information System (Sistema de Informações Ambulatoriais de Saúde, SIA, in Portuguese). The procedure analyzed was 03.03.12.005-3–Treatment of Bone Pain/Metastasis with Radiopharmaceutical (per treatment – excluding thyroid cancer). This code is limited to outpatient billing; inpatient billing via the Hospital Admission Authorization (Autorização de Internação Hospitalar, AIH, in Portuguese) system is not permitted. The dataset of the Hospital Information System (Sistema de Informações Hospitalares do SUS, SIH/SUS, in Portuguese) was also reviewed, confirming the absence of inpatient records for this procedure.
For the Supplementary Health system, data were extracted from the Data Pannel of the Information Exchange in Supplementary Health Pattern (Painel de Dados do Padrão de Troca de Informações na Saúde Suplementar, D-TISS, in Portuguese) of the Brazilian National Supplementary Health Agency (Agência Nacional de Saúde Suplementar, ANS, in Portuguese). The D-TISS system receives data through mandatory electronic submissions from all health insurance operators in Brazil, who receive standardized procedure records from their network of accredited hospitals, clinics, and laboratories. This dataset covers inpatient and outpatient procedures, and it is updated and validated centrally by ANS. All procedures are registered in the D-TISS using standardized codes of the the Unified Supplementary Health Terminology (Terminologia Unificada da Saúde Suplementar, TUSS, in Portuguese), which ensure national uniformity of health-procedure recording in the private sector. Only procedures with codes corresponding to Beta-emitting radionuclide therapy were extracted for this analysis, matching the SUS criteria.
The following TUSS codes were included: 4.07.10.07-6–Treatment of Bone Metastases (Strontium-89) and 4.07.10.08-4–Treatment of Bone Metastases (Samarium-153). Both outpatient and inpatient procedures were aggregated. Only Beta-emitting radiopharmaceuticals were considered, as Alpha-emitting agents are not available in the SUS and were excluded to ensure comparability across systems.
Regarding radiopharmaceutical availability during the study period, Sr-89 was discontinued globally in 2018, resulting in its clinical use in Brazil ending around 2019 due to a lack of supply and shifting preference toward newer agents. And Sm-153 was discontinued by some international manufacturers in 2021, but national production in Brazil (under the name SAMAR-IPEN) continued, with a temporary interruption in 2021. During this period, emergency imports were permitted under Collegiate Directory Resolution RDC n° 567/2021 of the Brazilian Health Regulatory Agency (Agência Nacional de Vigilância Sanitária, ANVISA, in Portuguese), which regulated the exceptional importation of unregistered radiopharmaceuticals. As of the current study's end, there was no public record of permanent discontinuation of SAMAR-IPEN, and Sm-153 remains available for palliative bone pain therapy in Brazil.
The present study covered the period from January 2015 to December 2023, encompassing 3 distinct stages: prepandemic (January 2015–February 2020), pandemic (March 2020–December 2022), and postpandemic (January–December 2023), as defined according to the most recent data available in the D-TISS database. Although the DATASUS updates its data more frequently, the time range and period definitions were standardized to enable a consistent temporal comparison between systems.
All procedures associated with the selected codes from the Management System of the Table of Procedures, Medications, and Orthoses, Prostheses and Auxiliary Means of Locomotion of the SUS ((Sistema de Gerenciamento da Tabela de Procedimentos, Medicamentos e OPM do SUS, SIGTAP, in Portuguese) and TUSS were included. Monthly aggregated counts were used. No individual-level variables (such as age, sex, and diagnosis) were accessed or linked across datasets. Missing data were not applicable, and no imputation was performed.
Monthly procedure counts for each system were summarized as median and interquartile range (IQR) values. The Mann–Whitney U test was used to compare monthly procedure volumes between SUS and the Supplementary Health system during the prepandemic period (January 2015–February 2020).
Additionally, to evaluate differences in monthly procedure volumes across the three periods within each health system, the Kruskal-Wallis test was applied. Where appropriate, pairwise Mann–Whitney U tests were used to identify which periods differed significantly.
To assess the impact of the pandemic, we used an interrupted time series (ITS) approach. Segmented linear regression models were fitted for each system, with March 2020 as the interruption point. The models estimated immediate changes in level (intercept) and postinterruption trend (slope). Wilcoxon signed-rank tests were also used to compare the monthly volumes observed during the pandemic to projected values based on prepandemic trends. In the postpandemic period (2023), no procedures were recorded in the SUS, preventing a formal statistical comparison with the Supplementary Health system. All analyses were performed using the Python software (free and open source), version 3.X, with the following packages: pandas, scipy, and statsmodels.
The current study used publicly-available, anonymized, and aggregated data. In accordance with Resolution no. 510/2016 of the Brazilian National Health Council (Conselho Nacional de Saúde, CNS, in Portuguese), ethical approval was not required.
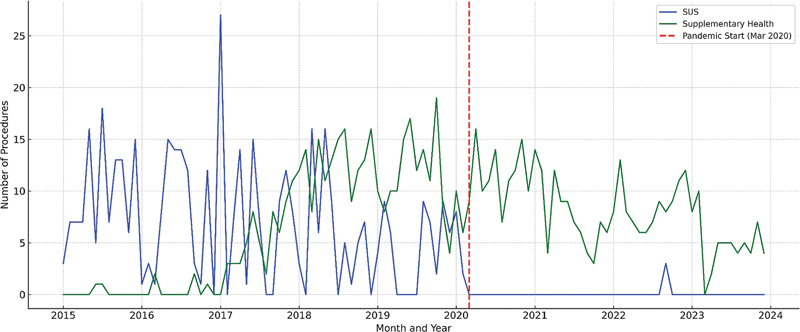
Between January 2015 and December 2023, 434 procedures referring to Beta-emitting radionuclide therapy for bone pain in cancer patients were recorded in the SUS, and 749, in the Supplementary Health system.
Fig. 1 Line plot showing the monthly number of Beta-emitting radionuclide therapy procedures for bone pain in the in the Unified Health System (Sistema Único de Saúde, SUS, in Portuguese) and the Supplementary Health (private) system (2015–2023). The shaded area indicates the pandemic period (March 2020–December 2022).
| Period | SUS: total | SUS: median (IQR) | Supplementary Health (private) system: total | Supplementary Health system: median (IQR) |
|---|---|---|---|---|
| Prepandemic (January 2015–February 2020) | 421 | 7 (1–11) | 362 | 5 (0–11) |
| Pandemic (March 2020–December 2022) | 13 | 0 (0–0) | 328 | 9 (7–12) |
| Postpandemic (January–December 2023) | 0 | 0 (0–0) | 59 | 5 (4–7) |
| Total | 434 | 2 (0–8) | 749 | 6 (3–10) |
Abbreviations: IQR, interquartile range; SUS, Sistema Único de Saúde (Brazilian Unified Health System).
The Mann–Whitney U test was applied to compare monthly procedure volumes between the SUS and the Supplementary Health system during the prepandemic period. The test yielded U = 1809.0 and p = 0.21, indicating no statistically significant difference between the two systems.
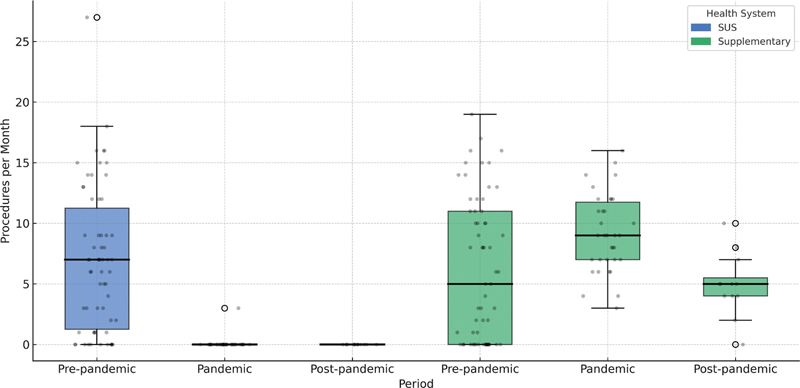
The Kruskal-Wallis test identified a highly-significant difference in monthly procedure volumes across the three periods in the SUS (H = 58.32; p < 0.001) and in the Supplementary Health system (H = 8.93; p = 0.012). These differences are visually represented in
Fig. 2 Boxplots representing the distribution of monthly Beta-emitting radionuclide therapy procedures for bone pain across three periods—prepandemic, pandemic, and postpandemic—in the SUS and Supplementary Health systems. The Boxes show median and interquartile range (IQR) values; the whiskers indicate the range of the values found.
Pairwise comparisons using the Mann–Whitney U test revealed a highly significant reduction in monthly procedures from the pre-pandemic to the pandemic period in the SUS (U = 2042.5, p < 0.001). In the Supplementary Health system, there was a statistically significant increase in procedure volumes from the pre-pandemic to the pandemic period (U = 542.5, p = 0.022), followed by a significant decline from the pandemic to the post-pandemic period (U = 82.0, p = 0.0017). These trends are also clearly demonstrated in the boxplots in
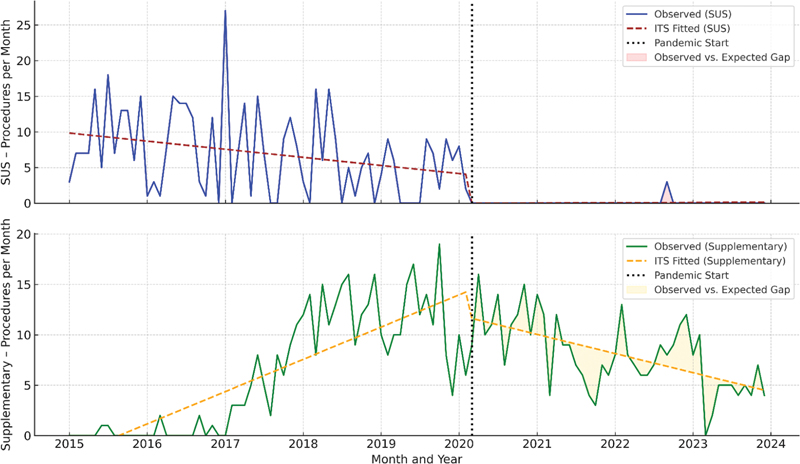
Observed versus expected volumes (ITS analysis): Segmented regression models using ITS were applied to assess the impact of the pandemic on monthly procedural volumes (
Fig. 3 Interrupted time series (ITS) analysis of the monthly radionuclide therapy procedures in the SUS and Supplementary Health systems (2015–2023). Segmented regression models (ITS) illustrating the impact of the coronavirus disease 2019 (COVID-19) pandemic (vertical dashed line in March 2020) on monthly procedure volumes in the SUS and Supplementary Health systems. The solid lines represent data observed; the dashed lines show modeled trends before and after the interruption point.
For the Supplementary Health system, the ITS model identified a significant immediate increase in procedure volumes following the pandemic onset (level change β = 5.50; p < 0.001), followed by a gradual decline postinterruption (slope β = −0.099; p = 0.003), which is consistent with a transient compensatory effect and subsequent normalization. The prepandemic trend remained stable (p = 0.521).
A comparison of the monthly values observed during the pandemic with those projected from prepandemic trends further confirmed the effect: the SUS demonstrated a highly-significant shortfall in procedures compared to the expectations (Wilcoxon signed-rank test; p = 0.000000000116), while the values observed for the Supplementary Health system remained statistically aligned with the projections (p = 0.62). This indicates that the pandemic's disruption was specific and substantial in the public sector, whereas the private sector maintained service levels consistent with prepandemic expectations.
To compare the impact between systems, the mean monthly change from the prepandemic to the pandemic periods was calculated for each system: the SUS experienced a mean reduction of 8.0 procedures per month, while the Supplementary Health system exhibited a mean increase of 7.2 procedures per month. The Wilcoxon signed-rank test showed this difference was highly significant (p < 0.0000000001), underscoring the asymmetric impact of the pandemic across the 2 health systems in Brazil.
The COVID-19 pandemic led to a significant global reduction in nuclear medicine procedures, including radionuclide therapy—a trend also observed in Brazil.
Procedure volumes were statistically similar between the 2 systems prior to the pandemic (p = 0.21), indicating comparable access to these therapies in this period. The divergence observed after March 2020 coincided with the pandemic, and it may reflect differences in the capacity of each health system to adapt to service disruptions.
Several factors contributed to the pronounced reduction in radionuclide therapy procedures within the SUS. During the pandemic, the SUS absorbed most of the COVID-19 cases in Brazil, requiring the reallocation of healthcare resources—staff, beds, and equipment—to the management these patients. As a result, non-emergency services, including many oncology and palliative treatments, were deprioritized. Delays and cancellations in cancer screening, diagnosis, and surgery further compounded these challenges, resulting in fewer patients being referred for radionuclide therapy, often at more advanced disease stages.
Additionally, radionuclide therapy is only indicated for patients who meet strict clinical criteria (including confirmed multifocal osteoblastic metastases, preserved bone marrow reserve, and adequate renal function). The pandemic led to reduced diagnostic workups, delayed patient presentation, and further limitations in therapy eligibility—by decreasing the number of referrals and by increasing the proportion of patients who arrived with advanced or unfavorable disease profiles.
It is notable that, while procedure volumes in the Supplementary Health system initially increased during the pandemic, they gradually declined thereafter. This trend could be associated with evolving clinical practices, changes in institutional workflows, or the availability of alternative therapies such as Alpha-emitting agents in the private sector. However, our dataset does not enable us to draw conclusions regarding the underlying causes of these patterns.
Internationally, similar reductions in nuclear medicine activity were observed, and disparities in the ability of health systems to maintain service continuity during the pandemic have been widely reported. Supply chain disruptions (such as shortages of radioisotopes and protective equipment), changes in patient behavior due to fear of infection, and institutional constraints contributed to global declines in radionuclide therapy, particularly in public sector settings.
The current study is subject to several limitations inherent to analyses based on aggregated, routinely-collected administrative data (RECORD design). The primary objective was to compare the use of Beta-emitting radionuclide therapy for bone pain in the public and private health systems throughout the prepandemic, pandemic, and postpandemic periods in Brazil. Accordingly, the analysis was restricted to procedural counts as recorded in national health databases, without access to patient-level clinical information, tumor types, stage at diagnosis, or outcomes. Assessment of clinical appropriateness, effectiveness, or other individual-level factors was therefore not possible.
For the SUS, only outpatient billing data were available; inpatient procedures and those billed under alternative codes may not have been captured, potentially resulting in an underestimation of the true number of procedures. In the Supplementary Health system, both inpatient and outpatient procedures were included via the D-TISS database, but this source may be subject to reporting inconsistencies and does not guarantee comprehensive coverage of all private operators.
Only Beta-emitting radiopharmaceuticals (Sm-153 and Sr-89) were considered, as Alpha-emitting agents were not uniformly available or comparable between systems during the study period. The analysis did not adjust for the withdrawal of Sr-89 or supply interruptions of Sm-153, which may have affected procedural volumes regardless of the pandemic context. Notably, records of Sm-153 procedures persisted in the Supplementary Health system data even after the temporary interruption of national production in 2021, with entries continuing to appear through 2023. This persistence may reflect the use of imported products (permitted via emergency regulatory provisions for the private sector) or possible delays and errors in D-TISS data entry.
Finally, the exclusive use of procedural volumes as the outcome precludes any inference about clinical benefit, patient survival, or quality of life, and the findings should be interpreted as service-use trends within the limits of administrative data.
Future research should examine regional variations regarding the impact of the pandemic on access to radionuclide therapy, as well as long-term trends associated with the incorporation of new technologies such as Alpha-emitting agents. It is equally important to advance the use and validation of administrative data from the Supplementary Health sector (D-TISS), given its growing relevance for national health analyses. Particular attention should be given to the identification and correction of potential data entry or coding errors, which may affect the accuracy of procedural counts and trend analyses. Additionally, research should assess potential regional disparities in the access to palliative radionuclide therapy across Brazil, leveraging public and private health data. Developing robust and interoperable data strategies is crucial to ensure the equitable and sustained provision of palliative therapies in both health sectors, and to strengthen resilience in the face of future public health emergencies.
The current study demonstrates that the COVID-19 pandemic caused a marked and sustained reduction in access to Beta-emitting radionuclide therapy for bone pain within the SUS, with procedure volumes falling to 0 in 2023. In the Supplementary Health system, procedure volumes increased during the pandemic and later declined, resulting in an overall shift in service distribution between sectors.
Prior to the pandemic, there was no statistically significant difference in access between the public and private health systems. The divergence observed after 2020 highlights the different abilities of each sector to respond to healthcare disruptions.
Continuous monitoring of the access to palliative radionuclide therapy, assessment of regional disparities, and evaluation of the impact of new technologies are important steps for future research and health policy planning. Ensuring equitable and resilient access to essential oncologic services across all sectors remains a public health priority.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Mercadante, S and Klepstad, P and Kurita, G P and Hjermstad, M J and Sloan, P and Caraceni, A. Multidisciplinary approach to pain management in cancer patients: a European Society of Medical Oncology (ESMO) position paper. Ann Oncol [online]. 2018, vol. 29, p. iv16-iv21. https://doi.org/10.1093/annonc/mdy115 Ver referência
2. Paes, F M and Serafini, A N. Systemic metabolic radiopharmaceutical therapy in the treatment of metastatic bone pain. Semin Nucl Med [online]. 2010, vol. 40, p. 89-104. https://doi.org/10.1053/j.semnuclmed.2009.10.003 Ver referência
3. Etchebehere, E C and Pereira, C A and Lima, M C. Treatment of bone pain secondary to metastases using samarium-153-EDTMP. Sao Paulo Med J [online]. 2004, vol. 122, p. 208-212. https://doi.org/10.1590/S1516-31802004000500006 Ver referência
4. Sapienza, M T and Ono, C R and Guimarães, M IC and Watanabe, T and Costa, P A and Buchpiguel, C A. Retrospective evaluation of bone pain palliation after samarium-153-EDTMP therapy. Rev Hosp Clin Fac Med Sao Paulo [online]. 2004, vol. 59, p. 321-328. https://doi.org/10.1590/S0041-87812004000600003 Ver referência
5. Resche, I and Chatal, J F and Pecking, A. A dose-controlled study of 153Sm-EDTMP in the treatment of patients with painful bone metastases. Eur J Cancer [online]. 1997, vol. 33, p. 1583-1591. https://doi.org/10.1016/s0959-8049(97)00155-x Ver referência
6. Lewington, V J. Bone-seeking radionuclides for therapy. J Nucl Med [online]. 2005, vol. 46, p. 38S-47S.
7. Fischer, M and Kampen, W U. Radionuclide Therapy of Bone Metastases. Breast Care (Basel) [online]. 2012, vol. 7, p. 100-107. https://doi.org/10.1159/000337634 Ver referência
8. Maringe, C and Spicer, J and Morris, M. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study. Lancet Oncol [online]. 2020, vol. 21, p. 1023-1034. https://doi.org/10.1016/S1470-2045(20)30388-0 Ver referência
9. Araujo, S EA and Leal, A and Centrone, A FY. Impact of COVID-19 pandemic on care of oncological patients: experience of a cancer center in a Latin American pandemic epicenter. Einstein (Sao Paulo) [online]. 2020, vol. 19, p. eAO6282. https://doi.org/10.31744/einstein_journal/2021AO6282 Ver referência
10. Freudenberg, L S and Paez, D and Giammarile, F. Global Impact of COVID-19 on Nuclear Medicine Departments: An International Survey in April 2020. J Nucl Med [online]. 2020, vol. 61, p. 1278-1283. https://doi.org/10.2967/jnumed.120.249821 Ver referência
11. Sud, A and Jones, M E and Broggio, J. Collateral damage: the impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann Oncol [online]. 2020, vol. 31, p. 1065-1074. https://doi.org/10.1016/j.annonc.2020.05.009 Ver referência
12. . Available from: . Accessed 23 Jul 2025 [online]. Available from: <https://www.drugshortagescanada.ca/discontinuance/63929>.
13. Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária (ANVISA). Voto n° 183/2022/SEI/DIRE5/ANVISA. ANVISA, 2022.
14. Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária (ANVISA). Resolução - RDC n° 567, de 29 de setembro de 2021. Diário Oficial da União, 2021.
Dados de acesso insuficientes para visualização no mapa.