Taxanes are widely used for breast cancer treatment.
Premedication with dexamethasone and diphenhydramine may be associated with several adverse events, such as insomnia, weight gain, and acne, with potential impacts on QoL.
To address this knowledge gap, we conducted a prospective study with the primary endpoint of assessing patient-reported QoL in two comparative groups: one group that kept and another that omitted premedication according to the presence or absence of HSR. We hypothesized that premedication omission during weekly paclitaxel therapy would be related to fewer adverse events overall and higher QoL in breast cancer patients. We used the European Organization for Research and Treatment of Cancer's (EORTC) 30-item Core Quality of Life questionnaire (QLQ-C30) and 23-item Quality of Life Questionnaire–Breast Cancer Module (QLQ-BR23) at to perform these comparisons.
The current was a single-center, prospective, phase-2 study conducted at the Oncology Center at Hospital São Lucas, located in the city of Porto Alegre, Brazil. The eligibility criteria for enrollment were female breast cancer patients who would receive a standard weekly dose of paclitaxel (80mg/m2) as part of the neoadjuvant, adjuvant or palliative treatments, aged between 18 and 75 years, with performance status scores from 0 to 2, and ability to provide informed consent prior to enrollment. The exclusion criteria were chronic use of corticosteroids, prior use of taxane, combination of paclitaxel with another chemotherapy agent simultaneously, a taxane regimen other than on a weekly schedule, and other neoplasms. The combination of paclitaxel and trastuzumab was allowed.
The clinical trial was approved by the institutional Ethics Committee according to local regulation, and all patients provided written informed consent before enrollment. The trial was registered at the publicly-available Brazilian study registry Plataforma Brasil (under registration number 56605322.7.0000.5336).
Patients were included in the study from April 2022 to April 2024. All patients received intravenous dexamethasone 10 mg and diphenhydramine 50 mg 30 minutes prior to paclitaxel infusion as prophylaxis to HSR in the first 3 of the 12 planned weeks of treatment. If no HSR occurred after the third week of paclitaxel, premedication was allowed to be discontinued for the remaining 9 weeks of treatment, as long as agreed upon by the attending physician. Therefore, the patients were divided split into two groups for subsequent comparisons using the per protocol principle: one group that discontinued premedication and one group that did not, regardless of the reason for premedication continuation.
We interviewed patients on weeks 1, 2, 3, 4, 5, 9, and 12 of treatment in face-to-face appointments to assess QoL using self-reported descriptive and evaluative measurements. We used three different questionnaires at every time point, as described below.
We selected the validated Portuguese version of the QLQ-C30 to address health-related QoL in cancer patients in general. This questionnaire is composed of a global health/QoL (GH/QoL) scale, as well as functioning and symptoms scales. We used the combination of items 29 and 30 as the main QLQ-30 measurement of QoL, according to EORTC guidance. The higher the score, the higher the QoL.
The validated Portuguese version of the QLQ-BR23 was selected to evaluate specific QoL factors in breast cancer patients. The multi-item scales are divided into 2 groups: functional (body image, sexual functioning, sexual enjoyment, and future perspective) and symptom-focused (systemic therapy side effects, breast symptoms, arm symptoms, and upset by hair loss). We used the combination of items 1, 2, 3, 4, 6, 7, and 8 (that is, the systemic therapy side effects [BRST] scale) as the main QLQ-BR23 measurement of QoL. Higher scores represent greater symptom burden.
Items from the QLQ-C30 and QLQ-BR23 were scaled and scored according to the scoring manual methodology: patients provided their answers to both questionnaires on a 4-point scale (from 1 [“not at all”] to 4 [“very much”]), except for the GH/QoL, which is a 7-point scale (from 1 [“very poor”] to 7 [“excellent”]). Linear transformation was used to standardize the raw score, so that the overall scores ranged from 0 to 100.
The 14-item modified Dexamethasone Symptom Questionnaire (DSQ) was developed by the University of Toronto to evaluate the frequency of adverse events related to the use of dexamethasone
The patients were physically evaluated and treated for HSRs by trained oncology fellows on call at the Oncology Center. The severity of the HSRs was graded according to the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE), version 5.0.
The primary endpoint of the current study was the comparison of QoL between the group that kept and the group that omitted premedication using scores for the main QLQ-C30 and QLQ-BR23 measurements, as aforementioned. We analyzed questionnaires from interviews conducted in weeks 3, 4, 5, 9, and 12, when the patients had already been split into the 2 groups.
The study secondary endpoints were the evaluation of the frequency of severe HSRs according to the CTCAE in patients who withdrew premedication, the frequency of HSRs of any grade during the 12 weeks of treatment in both groups, and the frequency of highest-grade adverse events in both groups according to the DSQ.
We conducted an exploratory analysis comparing GH/QoL scores in weeks 1 and 12 in each patient to analyze if there was a detriment in QoL over time. We also analyzed weight gain during the 12 weeks of treatment.
For the GH/QoL scale of the QLQ-C30 and the BRST of the QLQ-B23, the statistical analyses were based on a linear mixed effects model comparing the 2 groups of patients from weeks 3 to 12 of treatment. The models were developed with treatment, a time effect, and treatment-time interactions as fixed effects, as well as a patient-specific random effect. Parameter estimates were based on a restricted maximum likelihood method.
The Chi-squared test of independence was used to evaluate the association between the two groups and the incidence of subjects who had at least 1 toxicity score of “3” or “4” in the DSQ, indicating high toxicity. The analysis was conducted based on data collected from weeks 4 to 12 of treatment.
All statistical tests were performed on an exploratory basis, and all p-values lower than 0.05 were deemed statistically significant. No correction for multiplicity was made. Data analysis was performed using the R (R Foundation for Statistical Computing) software, version 4.3.3.
We recruited 60 patients. Data were analyzed according to the per protocol principle: 32 patients were allocated to the group that omitted premedication after the first 3 weeks of treatment, and 28 patients were allocated to the group that kept premedication throughout the 12 weeks of treatment. The baseline characteristics of all patients (and according to group) are summarized in
| With premedication(N = 28) | Without premedication(N = 32) | Overall(N = 60) | |
|---|---|---|---|
| Mean age (years) | 51.3 (8.27) | 54.4 (9.97) | 53.0 (9.28) |
| Median age in years (minimum–maximum) | 51.0 (31.0–69.0) | 53.5 (34.0–73.0) | 52.0 (31.0–73.0) |
| Age (years): n (%) | |||
| < 40 | 1 (3.6) | 2 (6.3) | 3 (5.0) |
| 40–59 | 22 (78.6) | 22 (68.8) | 44 (73.3) |
| 60–69 | 5 (17.9) | 5 (15.6) | 10 (16.7) |
| ≥ 70 | 0 (0) | 3 (9.4) | 3 (5.0) |
| ECOG performance status: n (%) | |||
| 0 | 18 (64.3) | 16 (50.0) | 34 (56.7) |
| 1 | 10 (35.7) | 15 (46.9) | 25 (41.7) |
| 2 | 0 (0) | 1 (3.1) | 1 (1.7) |
| Stage at diagnosis: n (%) | |||
| I | 3 (10.7) | 4 (12.5) | 7 (11.7) |
| II | 16 (57.1) | 15 (46.9) | 31 (51.7) |
| III | 5 (17.9) | 11 (34.4) | 16 (26.7) |
| IV | 4 (14.3) | 2 (6.3) | 6 (10.0) |
| Chemotherapy protocol: n (%) | |||
| Weekly paclitaxel | 2 (7.1) | 1 (3.1) | 3 (5.0) |
| AC-T dose dense | 12 (42.9) | 18 (56.3) | 30 (50.0) |
| AC-T | 3 (10.7) | 4 (12.5) | 7 (11.7) |
| Weekly paclitaxel + trastuzumab | 4 (14.3) | 5 (15.6) | 9 (15.0) |
| AC-TH | 7 (25.0) | 4 (12.5) | 11 (18.3) |
| Mean Body Mass Index (kg/m2) | 29.1 (5.24) | 28.0 (5.46) | 28.5 (5.34) |
| Median Body Mass Index in kg/m2 (minimum–maximum) | 29.1 (20.2–40.3) | 27.1 (17.9–45.1) | 27.9 (17.9–45.1) |
Abbreviations: AC-T; AC-TH; ECOG, Eastern Cooperative Oncology Group.
All patients completed weeks 1 to 12 of paclitaxel, with a total of 418 infusions. One patient needed a paclitaxel dose reduction to 60 mg/m2 from weeks 9 to 12 due to grade-3 fatigue. All patients received dexamethasone and diphenhydramine as premedication in the first 3 weeks of treatment, and HSRs occurred in 10 of the 60 patients (16.7%) in this period, all grade 1. Therefore, premedication was kept in those patients. After the third week of paclitaxel, the remaining 50 patients met the criteria for premedication omission given the absence of HSR. However, premedication was kept in 18 of these patients (36%). The reason to keep premedication in patients who had not experienced HSRs were chemotherapy-related symptoms such as nausea (24%), rash (12%), and preference of the attending physician (20%). No additional episodes of HSRs occurred on weeks 3 to 12 of paclitaxel in either group.
Compliance to the QoL assessment was high. Missing data from 2 patients at weeks 10 and 12 were excluded from the analysis.
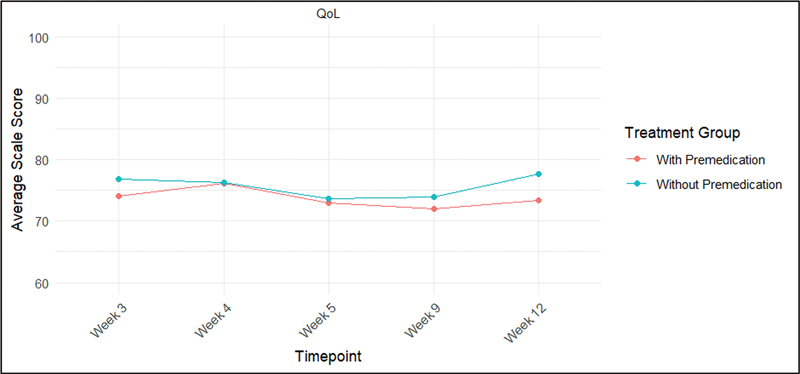
We first assessed global health using the combined score from items 29 and 30 of the QLQ-C30 (first primary endpoint). The scores at weeks 3, 4, 5, 9, and 12 for each group are presented in
Fig. 1 Evolution of average quality of life (QoL) scores over time (from week 3). Note: “QoL” represents the combination of items 29 and 30 from the European Organization for Research and Treatment of Cancer's (EORTC) 30-item Core Quality of Life questionnaire (QLQ-C30). Higher scores represent higher levels of quality of life.
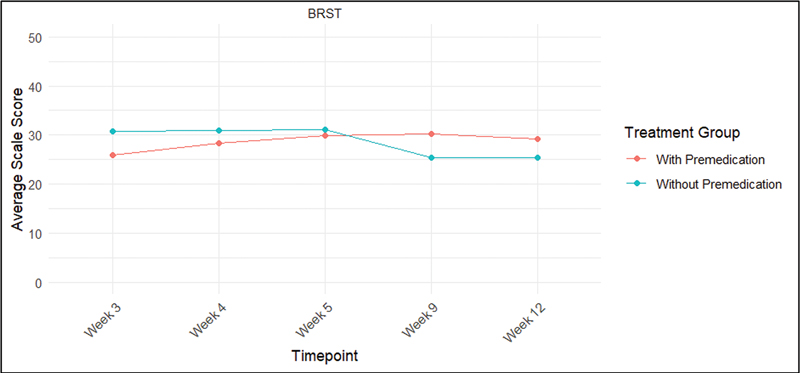
Next, we evaluated systemic symptoms using the BRST scores of the QLQ-BR23 (second primary endpoint). There were no statistically significant differences regarding the average QoL scores in the comparison of the 2 groups during weeks 3, 4, 5, 9, and 12 (p = 0.278; linear mixed effects model) (
Fig. 2 Evolution of systemic therapy side effects (BRST) scores over time (from week 3). Note: “BRST” represents the combination of items 1, 2, 3, 4, 6, 7, and 8 from the EORTC's 23-item Quality of Life Questionnaire–Breast Cancer Module (QLQ-BR23). Higher scores represents greater symptom burden.
As exploratory analyses, we evaluated global changes in QoL throughout the combined scores on items 29 and 30 of the QLQ-C30 at weeks 1 (baseline) and 12 (end of treatment) in the 2 groups (
| With premedication | Without premedication | |||
|---|---|---|---|---|
| Week | Average QoL score | Change from week 1 | Average QoL score | Change from week 1 |
| 1 | 76.5 | − | 76.3 | − |
| 12 | 73.4 | -3.1 | 77.6 | 1.3 |
Note: “QoL” combines information from items 29 and 30 of the European Organization for Research and Treatment of Cancer's (EORTC) 30-item Core Quality of Life questionnaire (QLQ-C30).
We also analyzed, in an exploratory way, the different subdomains and symptoms from the QLQ-C30 and QLQ-BR23 (
Another difference was observed in the sexual enjoyment (BRSEF) score. For the group of patients receiving premedication, there was an 8.93-point decrease in the average score from weeks 3 to 12 (95%CI: -18.3–0.459; p 0.0614). On the other hand, the group of subjects not receiving premedication showed an increase in the BRSEF score of 5.21 points (95%CI: -2.34–12.8; p = 0.169), raising the hypothesis that premedication may contribute to worsening sexual health in breast cancer patients.
We also described QoL measures according to patient subgroups, which were devided according to age, clinical stage, and chemotherapy protocol received (
The incidence of high toxicity scores according to the DSQ (secondary endpoint) is presented in
| Weeks 4 to 12 with premedication (N = 28): n (%) | Weeks 4 to 12 without premedication (N = 32): n (%) | p-value† | |
|---|---|---|---|
| Heartburn | 15 (53.6) | 12 (37.5) | 0.2119 |
| Insomnia | 15 (53.6) | 16 (50.0) | 0.7824 |
| Nausea | 5 (17.9) | 8 (25.0) | 0.5029 |
| Vomiting | 0 (0.0) | 1 (3.1) | 0.3455 |
| Appetite decrease | 9 (32.1) | 5 (15.6) | 0.1313 |
| Appetite increase | 10 (35.7) | 17 (53.1) | 0.1762 |
| Hiccup | 3 (10.7) | 3 (9.4) | 0.8630 |
| Weight decrease | 0 (0.0) | 1 (3.1) | 0.3455 |
| Weight increase | 3 (10.7) | 5 (15.6) | 0.5767 |
| Agitated | 15 (53.6) | 15 (46.9) | 0.6048 |
| Acne | 6 (21.4) | 3 (9.4) | 0.1921 |
| Mucositis | 4 (14.3) | 5 (15.6) | 0.8848 |
| Drowsiness | 10 (35.7) | 12 (37.5) | 0.8861 |
| Dizziness | 4 (14.3) | 5 (15.6) | 0.8848 |
Notes: The percentages are based on N; † p-value based on the Chi-squared test of independence.
The present was one of the first studies to address QoL as a primary endpoint using two comparative groups, one that kept premedication and another that omitted premedication, in breast cancer patients receiving weekly paclitaxel. We found that premedication omission did not lead to increased incidence of HSRs. However, contrary to our hypothesis, we were not able to demonstrate statistically significant differences in QoL scores between the two groups, as assessed using items 29 and 30 of the QLQ-C30 and the BRST score. On the other hand, the exploratory analyses suggested an impact of premedication on certain subdomains/symptoms (such as sexual enjoyment and breast symptoms), and this raised questions regarding the adequacy of the questionnaires to detect QoL differences in the context that they were used in the current study, as discussed below.
Premedication withdrawal in patients who did not present HSRs was a safe strategy in the present study, with no cases of HSR, nor need of rescue medications during the remaining weeks of treatment. This result is in accordance with those of previous trials. For example, a study
Few previous studies have evaluated QoL related to premedication in breast cancer patients receiving chemotherapy as a primary endpoint. A trial
Another possible explanation for the lack of differences in QoL between the two groups of patients could be the fact that standard questionnaires to measure QoL may be too general and not accurate enough to detect changes in QoL specifically related to the use of premedication. This underscores the need to develop more sensitive and applicable questionnaires geared towards premedication-related aspects to be used in future randomized trials.
Even though the current study did not meet the prespecified primary endpoint, it enabled important insights related to the use of premedication in this setting. Because of the wealth of information collected throughout the study, we were able to perform exploratory analyses that, although not definitive, may assist in the decision-making process related to the use of premedication in the clinical practice and may inform the design of future studies focused on specific symptoms and/or subdomains of interest. For example, we did not find a deterioration in QoL over time during treatment (QLQ-C30 items 29/30 and BRST scores) in either of the two groups, but, contrasting with the opposite group, patients who did not receive premedication had a sharper decline in BRBS scores (that is, breast symptoms) and improvement in BRSEF scores (that is, sexual enjoyment). Such observations could be relevant with the aim of maintaining the QoL of patients during treatment.
The QoL in patients receiving chemotherapy commonly decreases during treatment, but the impact seems to be temporary, especially in early-stage disease, with improvement after cytotoxic treatment completion.
In summary, in the current study, premedication withdrawal in breast cancer patients treated with weekly paclitaxel was not related to statistically significant differences in global health status and breast cancer QoL scales when compared to patients that kept premedication. Nevertheless, certain domains, especially sexual functioning, seem to deteriorate in patients who received premedication. Future prospective and randomized trials exploring tailored questionnaires with specific domains and visual scales may be more accurate in detecting QoL differences related to premedication. The use of these improved tools may reduce the QoL-reporting disparities potentially observed in our study, which was conducted in a low-to-middle-income population.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
1. Mamounas, E P and Bryant, J and Lembersky, B. Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer: results from NSABP B-28. J Clin Oncol [online]. 2005, vol. 23, p. 3686-3696. https://doi.org/10.1200/JCO.2005.10.517 Ver referência
2. Sparano, J A and Wang, M and Martino, S. Weekly paclitaxel in the adjuvant treatment of breast cancer. N Engl J Med [online]. 2008, vol. 358, p. 1663-1671. https://doi.org/10.1056/NEJMoa0707056 Ver referência
3. Braverman, A S and Rao, S and Salvatti, M E and Adamson, B and McManus, M and Pierre, S. Tapering and discontinuation of glucocorticoid prophylaxis during prolonged weekly to biweekly paclitaxel administration. Chemotherapy [online]. 2005, vol. 51, p. 116-119. https://doi.org/10.1159/000085618 Ver referência
4. Berger, M J and Vargo, C and Vincent, M. Stopping paclitaxel premedication after two doses in patients not experiencing a previous infusion hypersensitivity reaction. Support Care Cancer [online]. 2015, vol. 23, p. 2019-2024. https://doi.org/10.1007/s00520-014-2556-x Ver referência
5. Vardy, J and Chiew, K S and Galica, J and Pond, G R and Tannock, I F. Side effects associated with the use of dexamethasone for prophylaxis of delayed emesis after moderately emetogenic chemotherapy. Br J Cancer [online]. 2006, vol. 94, p. 1011-1015. https://doi.org/10.1038/sj.bjc.6603048 Ver referência
6. Hwang, S Y and Chang, S J and Park, B W. Does chemotherapy really affect the quality of life of women with breast cancer?. J Breast Cancer [online]. 2013, vol. 16, p. 229-235. https://doi.org/10.4048/jbc.2013.16.2.229 Ver referência
7. Barroso-Sousa, R and Vaz-Luis, I and Di Meglio, A. Prospective Study Testing a Simplified Paclitaxel Premedication Regimen in Patients with Early Breast Cancer. Oncologist [online]. 2021, vol. 26, p. 927-933. https://doi.org/10.1002/onco.13960 Ver referência
8. Parinyanitikul, N and Tanpipattanakul, W and Poovorawan, N. Incidence of infusion hypersensitivity reaction after withholding dexamethasone premedication in early breast cancer patients not experiencing two previous cycles of infusion hypersensitivity reaction for weekly paclitaxel chemotherapy. Support Care Cancer [online]. 2018, vol. 26, p. 2471-2477. https://doi.org/10.1007/s00520-018-4087-3 Ver referência
9. Aaronson, N K and Ahmedzai, S and Bergman, B. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst [online]. 1993, vol. 85, p. 365-376. https://doi.org/10.1093/jnci/85.5.365 Ver referência
10. Fayers, P M and Aaronson, N K and Bjordal, K and Groenvold, M and Curran, D and Bottomley, A. The EORTC QLQ-C30 Scoring Manual. 3rd edition. European Organization for Research and Treatment of Cancer, 2001.
11. Baccarin, ALdC and Irene, M N and Cubero, DdIG. The feasibility of dexamethasone omission in weekly paclitaxel treatment for breast cancer patients. Support Care Cancer [online]. 2019, vol. 27, p. 927-931. https://doi.org/10.1007/s00520-018-4381-0 Ver referência
12. Wagner, L and Gray, R and Garcia, S. Abstract GS6-03: Symptoms and health-related quality of life on endocrine therapy alone (E) versus chemoendocrine therapy (C+E): TAILORx patient-reported outcomes results. Cancer Res [online]. 2019, vol. 79, p. GS6-GS03. https://doi.org/10.1158/1538-7445.SABCS18-GS6-03 Ver referência
13. International Breast Cancer Study Group. Impact of adjuvant therapy on quality of life in women with node-positive operable breast cancer. Lancet [online]. 1996, vol. 347, p. 1279-1284. https://doi.org/10.1016/S0140-6736(96)90936-8 Ver referência
14. Instituto Brasileiro de Geografia e Estatística (IBGE).. Educação 2023. Rio de Janeiro: IBGE; 2024. Available from: . Access in: June 2024 [online]. Available from: <https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=2102068>.
15. Hollen, P J and Gralla, R J and Kris, M G and McCoy, S and Donaldson, G W and Moinpour, C M. A comparison of visual analogue and numerical rating scale formats for the Lung Cancer Symptom Scale (LCSS): does format affect patient ratings of symptoms and quality of life?. Qual Life Res [online]. 2005, vol. 14, p. 837-847. https://doi.org/10.1007/s11136-004-0833-8 Ver referência
Dados de acesso insuficientes para visualização no mapa.