Sarcoidosis is a multisystem inflammatory disorder of unknown etiology and, in general, self-limited.(
There is controversy between the relation of sarcoidosis and cancer. The main hypothesis is that the immunological dysfunction and the chronic inflammation may contribute to the development of malignancies. According to the meta-analysis presented by Bonifazi et al. (2015)(
It has been previously described the development of sarcoidosis after a cancer diagnosis, mimicking metastatic implants.(
KCT, Caucasian, 48-years-old woman in a screening mammogram it was detected a 3,3cm nodule in the left breast classified as BIRADS-4C. The core biopsy of the breast lesion revealed a grade 2 invasive ductal carcinoma, ER 100%, PR 5%, HER2-negative, ki67 25%. She had clinically and radiologically negative axillary lymph nodes.
She had a positive familiar history of cancer, her mother had breast cancer at the age of 62-yearsold, maternal grandmother with thyroid cancer at 58-years-old and paternal aunt had gynecological cancer at 62-years-old.
She was treated with left breast lumpectomy and sentinel lymph node dissection. The anatomopathological examination confirmed the histological subtype, size and the negative sentinel lymph node. She was then referred to the oncology department for adjuvant treatment evaluation.
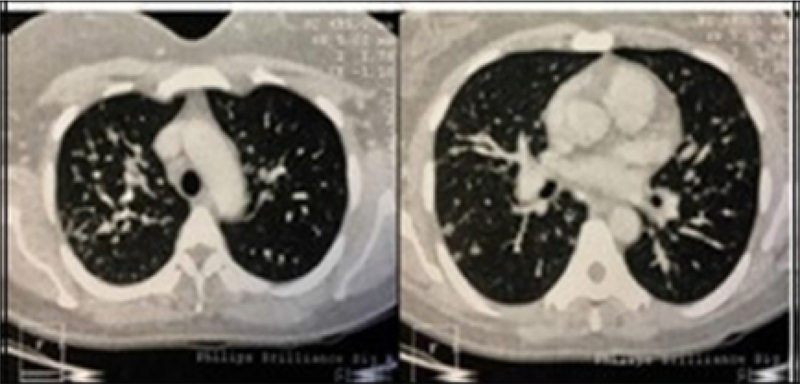
Her computerized tomography (CT scan) was ordered, evidencing interstitial pulmonary lesions, thickening in the peribronchial region and micronodules in the right lung and liver. These findings were described as suspected for metastatic lesions and lymphangitic carcinomatosis. At that moment she was asymptomatic, the clinical condition was not concordant with the suggested diagnosis by the CT images (
Figure 1 Chest CT showing images described as lymphangitic carcinomatosis.
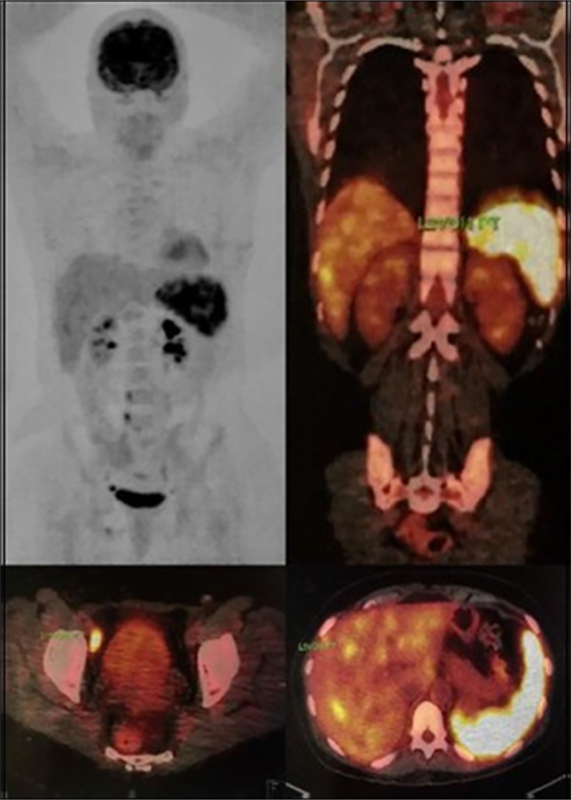
Figure 2 PET/CT evidencing intense FDG uptake in the spleen, iliac and inguinal lymph nodes and absence of contrast uptake in the lungs.
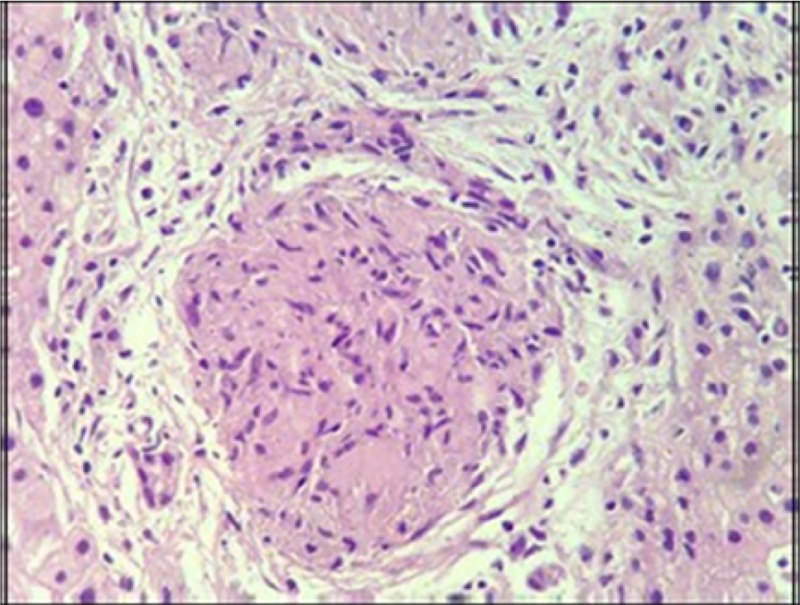
Considering the areas shown in the PET/CT, it was necessary to evaluate the histology of the metabolic active lesions. We proceeded with a liver biopsy in which the histological examination revealed a histiocytic infiltrate with formation of an epithelioid granuloma without necrosis, confirming the diagnosis of sarcoidosis (
Figure 3 Liver biopsy evidencing a sarcoidosis granuloma.
With these results, the final stage of the patient was pT2pN0. Patient was treated with adjuvant chemotherapy with docetaxel and cyclophosphamide for four cycles, followed by radiotherapy. She is currently disease free in hormone therapy (Tamoxifen 20mg/day) without major side effects.
Sarcoidosis and breast cancer are distinct diseases that affect females, mainly in middle age.(
The correlation between sarcoidosis and carcinogenesis remains unclear and several chronological associations are described. High frequency of sarcoidosis after lymphoma and breast cancer was observed.(
The difference between sarcoidosis and malignancy can be challenge. Although breast involvement is uncommon, palpable masses show the same characteristics that breast tumors. The possibility of axillary lymphadenopathy is also common to both conditions. Conventional imaging exams such as mammography and ultrasound have little value in disease differential.(
Metastatic lesions are the most important differential diagnosis to be excluded.(
In this case, the atypical and diffuse distribution FDG uptake was not compatible with the common pattern for breast cancer to metastasize and dissociated of the clinical condition. We would expect a patient with multiple metastasis to be symptomatic of the disease. Histological evaluation of a tissue biopsy remains as the gold standard for differentiating metastasis from other diseases.(
This case highlights the importance of the clinical evaluation and the complementary nature of imaging tests. Complementary tests should be interpreted in the light of the clinical findings to prevent misdiagnosis and over treatment.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No citations found for this article.
No references with the required fields found.
Dados de acesso insuficientes para visualização no mapa.